
Abstract

Lesions of the central nervous system may present with symptomatology suggestive of psychiatric conditions. This has been dramatically demonstrated previously with psychiatric presentations of large anterior cranial fossa meningiomas, leading to the recommendation that patients presenting with psychiatric syndromes in middle to later life and those refractory to treatment should undergo imaging to avoid delay of appropriate treatment [1, 2]. With the ready availability of high-resolution neuroimaging, patients with persistent or severe psychiatric symptoms should be considered for radiological and/or electrophysiological investigation.
We present three patients seen at Royal Melbourne Hospital, and the Epilepsy Unit at the Austin Hospital, Melbourne, with brain lesions causing complex partial seizures that were initially diagnosed and treated as panic attacks according to DSM-IV criteria [3]. Only the onset of generalized seizures or poor response to treatment led to subsequent imaging or referral for video-electroencephalogram (EEG) monitoring, at which time the correct diagnosis was made, leading to the instigation of successful treatment.
Patient 1
A 46-year-old man was referred to the Department of Neurosurgery, Royal Melbourne Hospital after the identification of a right temporal lobe tumour on magnetic resonance imaging (MRI) performed for investigation of a generalized seizure. He had a significant past history of depression and a 20 year history of auditory hallucinations, mainly of hearing someone talking behind him.
One year prior to admission, he began to experience episodes that were diagnosed as panic attacks. In these episodes, which often occurred at night, he would ‘go blank’, hyperventilate, become stiff and frozen, and clench his jaw. He would then have an overwhelming desire to escape from the room, associated with a feeling of panic. After these events he was tired and it would take some time for him to return to his normal self. Between the episodes he was psychiatrically normal. Computed tomography performed at the time of the onset of these episodes was said to show an ‘old stroke’, presumably a hypodense region in the right temporal region, but this was not available for review by us.
These episodes were managed, by a psychiatrist, as panic disorder with paroxetine, with a poor clinical response, until the patient had a single generalized tonic–clonic seizure. An MRI showed a right temporal non-enhancing tumour (Figure 1). EEG indicated slowing over the right temporal lobe without epileptiform discharges. He was commenced on anti-epileptic medication (phenytoin) and subsequently underwent a right temporal craniotomy and resection of the tumour. Histopathology was diagnostic of an anaplastic oligoastrocytoma. He has subsequently completed adjuvant radiotherapy. He has had no further seizures, including those associated with panic, for 12 months, but had an episode of depression associated with commencing a second anti-epileptic medication (levetiracetam).
Patient 1: T1-weighted axial contrast-enhanced magnetic resonance imaging of the brain. There is a hypointense region in the right temporal lobe that did not enhance with contrast (arrow). Following resection the lesion was found to be an anaplastic oligoastrocytoma on histology.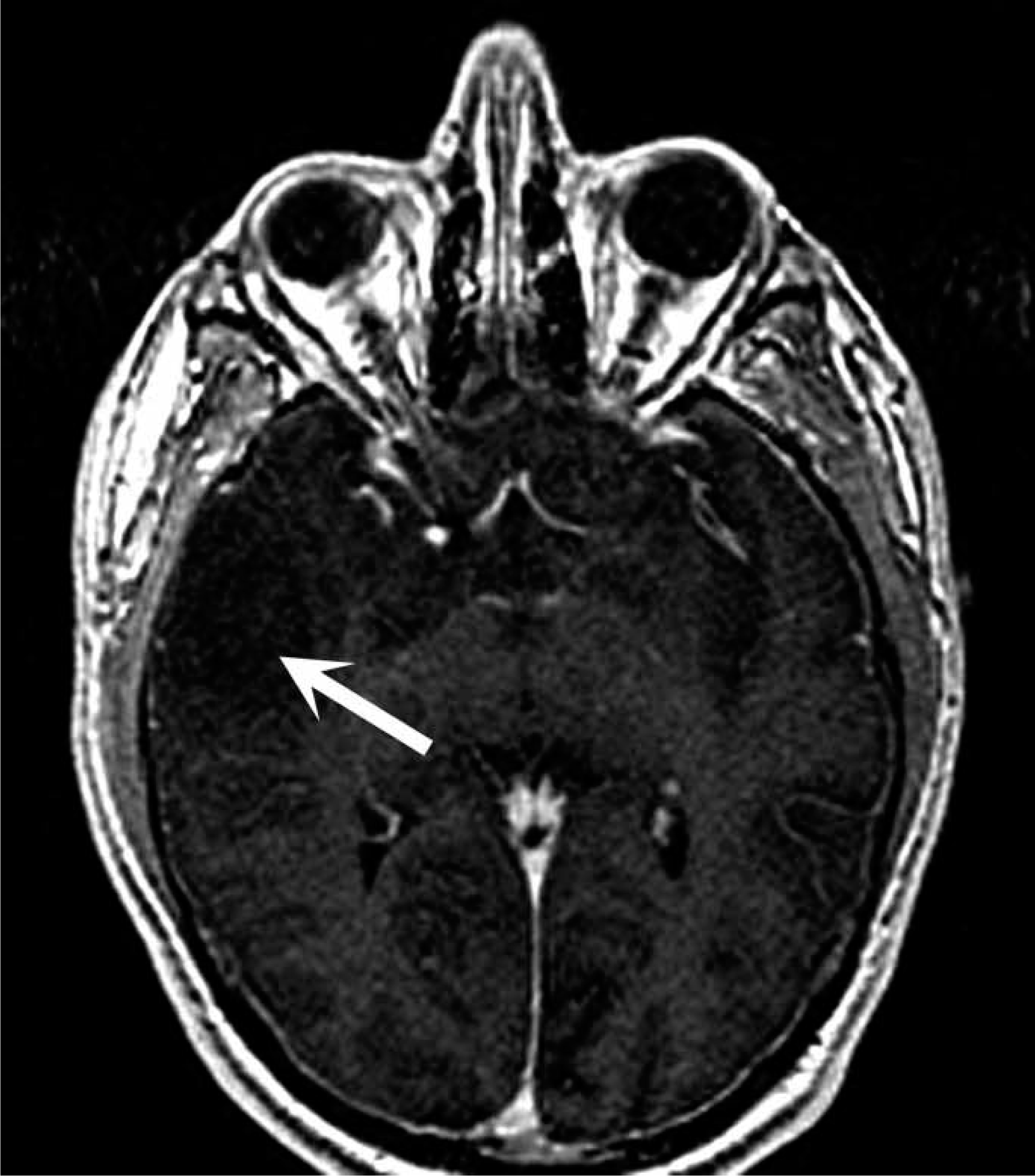
Patient 2
A 45-year-old man was referred to the Department of Neuropsychiatry, Royal Melbourne Hospital, with a 3 year history of episodes diagnosed and managed as panic attacks. The attacks were frequent, occurring almost daily, and would on occasion wake him from sleep. Treatment with the serotonin re-uptake inhibitor, paroxetine, had not altered the frequency or severity of the attacks. The only significant past history was of a motor vehicle accident 20 years previously during which he sustained a right frontal lobe injury requiring a craniotomy.
The episodes generally commenced with autonomic symptoms, including palpitations, a cold sweat, dry mouth, shallow breathing and a sense of impending doom. In association with these attacks he described a ‘funny feeling’ in his stomach that rose into his chest. At times he would also display unusual motor activity including repetitive rubbing of his fingers, chewing and lip smacking. He did not lose consciousness during these episodes but described a feeling of detachment. The episodes were followed by fatigue.
A routine EEG followed by video-EEG monitoring was performed. During the inter-ictal recording there were frequent epileptiform spikes over the right posterior frontal region. Several typical events were recorded during monitoring that were accompanied on the EEG by focal rhythmic seizure activity over this region. MRI demonstrated a large area of encephalomalacia in the right posterior frontal lobe, behind the region of the previous craniotomy (Figure 2), as well as signal abnormality in the right mesial temporal region. He was commenced on carbamazepine and has had no further events for over 12 months.
Patient 2: fluid-attenuated inversion recovery axial magnetic resonance imaging of the brain. There is a previous craniotomy with partial removal of the frontal lobe (white arrow) and signal change consistent with encephalomalacia in the region posterior to this (black arrow).
Patient 3
A 30-year-old woman was referred to the Epilepsy Unit at the Austin Hospital, Melbourne, following a generalized seizure. This seizure was associated with sleep deprivation and excessive alcohol intake, which was unusual for her. She had a history of depression and episodes that had been diagnosed and managed as panic attacks. These occurred at least weekly and usually in clusters of two or three per day. She had been referred to a psychologist 2 years previously for counselling to manage these episodes, which resulted in no significant change in their frequency of occurrence.
These episodes began 4 years prior to her first generalized seizure. The initial symptoms consisted of an olfactory or gustatory aura of either burning hair or coins. This was followed by a sense of fear or dread that she described as ‘as if my family were being killed in front of me’. Witnesses observed that the patient would usually stare and repeatedly swallow. She was unable to communicate during the episodes but did not lose consciousness. They lasted less than 1 minute and were followed by fatigue. They would often occur in clusters and without obvious provocation.
An EEG showed slowing and sharp waves over the right temporal lobe. MRI indicated a heterogenous lesion in the right parahippocampal gyrus consistent with a cavernous haemangioma (Figure 3). She was commenced on carbamazepine, which only partially controlled her seizures. Other anti-epileptic drugs, including lamotrigine and sodium valproate, also resulted in only partial control. On video-EEG monitoring and ictal single-proton emission computed tomography it was suggested that she would benefit from resection of the lesion in terms of seizure control.
Patient 3: T2-weighted coronal magnetic resonance imaging of the brain. There is a heterogenous lesion in the right parahippocampal gyrus (arrow) consistent with a cavernous haemangioma.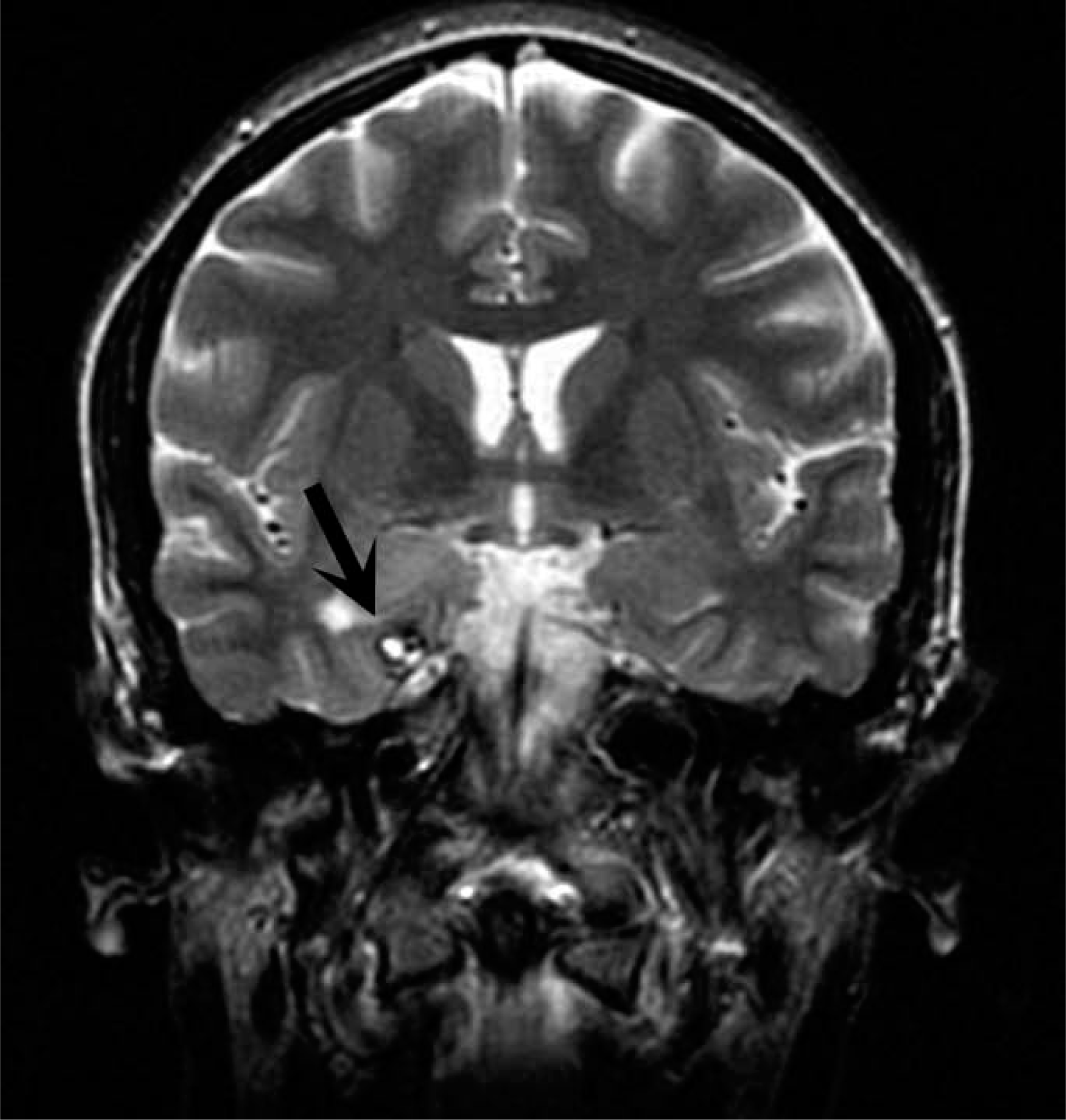
The patient underwent resection of the cavernous malformation with access through the middle temporal gyrus. The lesion was resected as a single piece with aspiration of surrounding haemosiderin-stained brain. The patient made an uncomplicated recovery and has been seizure free for more than 3 months on her usual medications.
Discussion
These three patients, although harbouring differing intracerebral pathology, presented with similar seizure-related symptomatology with features that led to misdiagnoses of panic attacks. A small number of similar reports in the literature have highlighted the diagnostic complexity of such cases and the importance of further investigation of patients presenting panic attacks that have atypical features or are resistant to treatment [4–9]. In addition to symptoms of anxiety or panic, on careful history such patients also manifest features suggestive of focal epilepsy, including auras, automatisms and post-ictal fatigue, which could reasonably have been considered an indication for early radiological or EEG investigation. The cases highlight the similar clinical symptomatology of panic attacks and seizures, particularly those arising in the frontal and temporal lobes.
Temporal and frontal lobe epilepsies may feature simple partial seizures, complex partial seizures, secondarily generalized seizures, or combinations of these seizure types. Simple partial seizures arising from the temporal lobe are typified by autonomic, psychological and sensory phenomena including olfactory and auditory hallucinations and déjà vu. There is not uncommonly an epigastric rising sensation or abdominal discomfort. Complex partial seizures of the temporal lobe often begin with these same symptoms followed by motor arrest and loss of awareness, typically accompanied by oroalimentary automatism. Post-ictal confusion is common [10]. Electrical stimulation studies of the temporal lobe have elicited panic and associated somatic signs and symptoms including dizziness, nausea, tachycardia, chest pain, altered temperature sensations and depersonalization [11]. Seizures with features similar to panic attack have been particularly linked to epilepsy arising in the right temporal lobe [12]. In the present series, patients 1 and 3 had lesions of the right temporal lobe. Patient 2, whose seizures appeared to arise in the right posterior frontal lobe, also exhibited abnormalities of the right mesial temporal lobe on MRI. Seizures in the posterior frontal lobe commonly rapidly spread to the temporal region.
Frontal lobe partial seizures are sometimes mistaken for psychogenic non-epileptic seizures (PNES) or ‘pseudoseizures’. They can occur several times a day and frequently arise out of sleep. Complex gestural automatisms are common. Complex partial seizures arising from the frontal lobe often have minimal or no post-ictal confusion. Rapid secondary generalization is a frequent feature, with status epilepticus a not-uncommon complication [10].
Based on these descriptions of temporal and frontal lobe seizures, the ‘panic attacks’ in each of the present three patients had features strongly suggestive of epilepsy. Two of the patients had a type of mass lesion, including an intrinsic brain neoplasm and a cavernous haemangioma, which has been associated with seizures in up to 80% of patients [13–17].
Panic attacks, like seizures, are unexpected, brief, paroxysmal, and self-limiting phenomena. DSM-IV classifies a panic attack as a discrete period of intense fear or discomfort that is associated with at least four of the following: palpitations, pounding heart or accelerated heart rate; sweating; trembling or shaking; sensations of shortness of breath or smothering; feeling of choking; chest pain or discomfort; nausea or abdominal distress; feeling dizzy, unsteady, lightheaded or faint; derealization or depersonalization; fear of losing control or going crazy; fear of dying; paraesthesias; chills or hot flushes [3]. Each of the present patients had episodes with features that also typified panic attacks, thus contributing to the diagnostic difficulty.
In addition to anxiety or panic occurring as a feature of the seizure or its aura, anxiety symptoms are common in patients with epilepsy [18, 19]. Anxiety may occur as a pre-ictal psychological reaction to symptoms that alert the patient to seizure onset, as a feature of the post-ictal state or as a distinct interictal behaviour [20]. Patients with epilepsy have a higher incidence of comorbid non-seizure panic attacks or anxiety disorders than the general population [18, 21, 22], and these may be misdiagnosed as seizures [23]. Anxiety or panic may be a feature of PNES in patients with or without co-existent epilepsy, where the differential diagnosis may be particularly difficult [24]. With careful clinical evaluation, these similar symptoms can often be differentiated. For example, the onset of ictal fear is paroxysmal and the duration is brief (30–120 s) [25], whereas panic attacks often build up over minutes with symptomatology lasting more than 5 min [26]. Furthermore, simple partial seizures characterized by fear, anxiety or autonomic symptoms generally progress to complex partial seizures, with change in consciousness, or generalize at some time [4].
Nonetheless, differentiating between seizures and panic attacks may be difficult on clinical grounds alone. The patients reported here were all initially diagnosed with, and had features of, panic attacks, yet all had atypical features to suggest seizures. Patient 1, with a right temporal anaplastic oligoastrocytoma, had paroxysmal panic with a significant past history of psychiatric illness, but also had oral automatisms and post-ictal fatigue. Patient 2, with post-traumatic right frontal encephalomalacia, had paroxysmal panic that was resistant to paroxetine, but also had episodes that would wake him from sleep, with manual and oral automatisms and post-ictal fatigue. Patient 3, with a right parahippocampal gyrus cavernoma, had paroxysmal panic that was resistant to psychotherapy, but the episodes were also preceded by an olfactory or gustatory aura and had oral automatisms and post-ictal fatigue. While there are differences between each presentation, a careful history from witnesses to the episodes elicited a history consistent with oral automatisms and post-ictal fatigue in all three patients.
In conclusion, when evaluating a patient with panic attacks, it is important to recognize that seizure symptomatology may also fulfil the DSM-IV criteria for panic disorder [3, 5] and that comorbid psychiatric illness and seizures is common [27]. Failure to make the correct diagnosis may lead to a failure to control symptoms, with prolonged suffering or delayed diagnosis of a neoplasm, or treatable lesion, as well as exposing the patient to the physical and medical risk of ongoing seizures. Patients with a first presentation of ‘panic attacks’ require a detailed history and clinical evaluation, with a high index of clinical suspicion for epilepsy. A detailed history from witnesses to the episodes can provide further information that leads to the diagnosis of a seizure disorder. With readily available access to imaging, any unusual presentation of psychiatric symptoms, or poor response to treatment, should warrant further investigation, including referral to a specialist epilepsy unit with video-EEG monitoring.