
Abstract
Clinical depression is a frequently chronic or recurrent illness that often requires several treatment trials before achieving remission. Identifying patient characteristics that might predict outcome to specific treatments for depression would clearly be clinically useful, through assisting the allocation of the right treatment to the right patient. Personality styles are one such patient characteristic with the potential to influence treatment outcome.
Many studies have examined the extent to which personality style may influence response to psychotherapy, including manualized psychotherapies such as cognitive behaviour therapy (CBT) and interpersonal psychotherapy (IPT) [1–4]. In essence, the profile of a poor psychotherapy responder weights neuroticism, perfectionism and depressive personality style components. Fewer studies, however, have considered any personality influence on response to antidepressant drugs. Neuroticism and harm avoidance have been associated with a poorer antidepressant treatment outcome [5, 6], but results have been inconsistent. As noted by several authors, many studies examining personality traits and treatment response have insufficient power to detect potential associations [6, 7].
Previously in this journal we reported the results of an online survey of 2962 Australian respondents who had ever received treatment for depression, examining retrospective self-reports of treatment effectiveness for a wide range of pharmacological, psychological and alternative strategies [8]. The current study further examines this dataset, investigating associations between personality dimensions assessed by our Temperament and Personality Questionnaire (T&P) [9] and retrospective self-reported treatment effectiveness. The eight personality styles assessed by the T&P were judged a priori as modulating the risk to depression onset and persistence (anxious worrying, perfectionism, personal reserve, irritability, social avoidance, rejection sensitivity, self-criticism and self-focus). The measure is a flexible one in that we previously quantified how those eight personality facets emerged from two high-order molar personality styles (i.e. neuroticism and introversion) [9], and progressively arborized until the eight-factor model emerged.
Method
Strategy
Because study nuances have been previously detailed [8], only relevant methodological issues will be described here. In essence, people accessing the Black Dog Institute website were invited (if they had received treatment for a lifetime episode of depression) to participate in an anonymous online survey. Participants were informed that the principal purpose of the study was to examine the relationship between personality styles and treatment response, with informed consent addressed by checking a box.
Those electing to participate were asked to respond to demographic questions, provide details of their depressive episodes and complete the 109-item T&P, detailed earlier [9]. The eight personality scales of the T&P have previously demonstrated high internal consistency and test–retest reliability [9]. Participants were asked whether they had consulted differing professionals for a depressive episode (e.g. general practitioner, psychiatrist, psychologist), and whether they had ever received any of a set of different treatments for depression, including antidepressant drugs; psychological therapies such as CBT and IPT and electroconvulsive therapy; and whether they had trialled self-help or alternative strategies. For each strategy trialled, they were required to rate its effectiveness on a 4 point scale (from ‘very effective’ to ‘not effective at all’) or, if relevant, record that the strategy had been ceased before its effectiveness could be judged.
Sample
We received 3486 consecutive fully completed returns before removing the questionnaire from the website. Because the current objective was to obtain regional data from those who were likely to have experienced clinical depression, we limited current analyses to a subset of 2692 subjects who met four criteria: (i) currently living in Australia; ≥18 years of age; (iii) first-time completers of the survey; and (iv) reporting a depressive episode lasting ≥2 weeks.
Data analyses
All analyses were conducted using the statistical software package SPSS version 14.0 (SPSS, Chicago, IL, USA). For each treatment examined, analyses were conducted among the sample of respondents who reported having ever trialled that treatment, excluding those who reported ceasing the treatment before its effectiveness could be judged. For the classes of antidepressants examined (i.e. selective serotonin re-uptake inhibitors (SSRIs), dual action serotonin and noradrenalin re-uptake inhibitors and tricyclic antidepressants (TCAs), a mean effectiveness score was computed by summing the effectiveness scores for all antidepressants tried in that class, and dividing this by the number of antidepressants in that class tried.
Pearson correlations were conducted between the eight personality scale scores and mean effectiveness ratings for the most commonly trialled treatments (i.e. the three antidepressant classes examined, and three psychological treatments). Second, in order to examine the individual impact of each personality style on treatment responsiveness to all trialled treatments and, after statistically controlling for the effect of age, gender and all seven other personality style scores, a series of linear regressions was conducted, with all eight personality scale scores, in addition to age and gender, as predictors of mean treatment effectiveness ratings. A linear regression was conducted for each treatment trialled by at least 100 respondents. Due to the exploratory nature of the analyses, statistical significance was set at p < 0.01.
Results
Sample description
Of the total sample of 2692, the mean age was 40.0 years (SD = 12.0 years, range = 18–77 years), 70.8% were female, 52.5% were married or living with a partner, while 45.9% were employed full-time and a further 20.1% were employed part-time. In terms of treatments for depression, 73.6% of subjects had received one or more antidepressant drug, 78.3% had received one or more psychological/counselling strategies, with 88.8% having received one or both such interventions. In terms of professionals ever consulted for a depressive episode, 83.1% of respondents reported that they had consulted a general practitioner; 57.9% a psychologist; 51.6% a psychiatrist (88.4% had consulted one or more of these three groups); while 34.8% had consulted one or more ‘other professionals’.
Personality and treatment effectiveness ratings
In our initial analyses we intercorrelated personality style scores with the self-reported effectiveness ratings for differing treatment modalities. Rather than table the very large matrix of coefficients, Table 1 reports the results of Pearson correlations between personality scale scores and effectiveness ratings for six of the most commonly trialled treatments (i.e. three classes of antidepressants, CBT and IPT/relationship therapy, and counselling). (Monoamine oxidase inhibitor (MAOI) antidepressants are not reported, due to the small number of 69 respondents who reported ever receiving an MAOI.) The large sample size generated a number of statistically significant coefficients but the associational strengths were, at best, low. Higher ‘self-criticism’ scores were associated with a diminished response to almost all tabulated treatments (with the exception of TCAs), higher ‘social avoidance’ and ‘personal reserve’ scores showed a similar – but not universal – pattern. In contrast, higher ‘perfectionism’ scores were associated with a better response to the three psychotherapies, but were not associated with response to the representative antidepressant drugs.
Pearson correlations between personality scale scores and ratings of treatment effectiveness
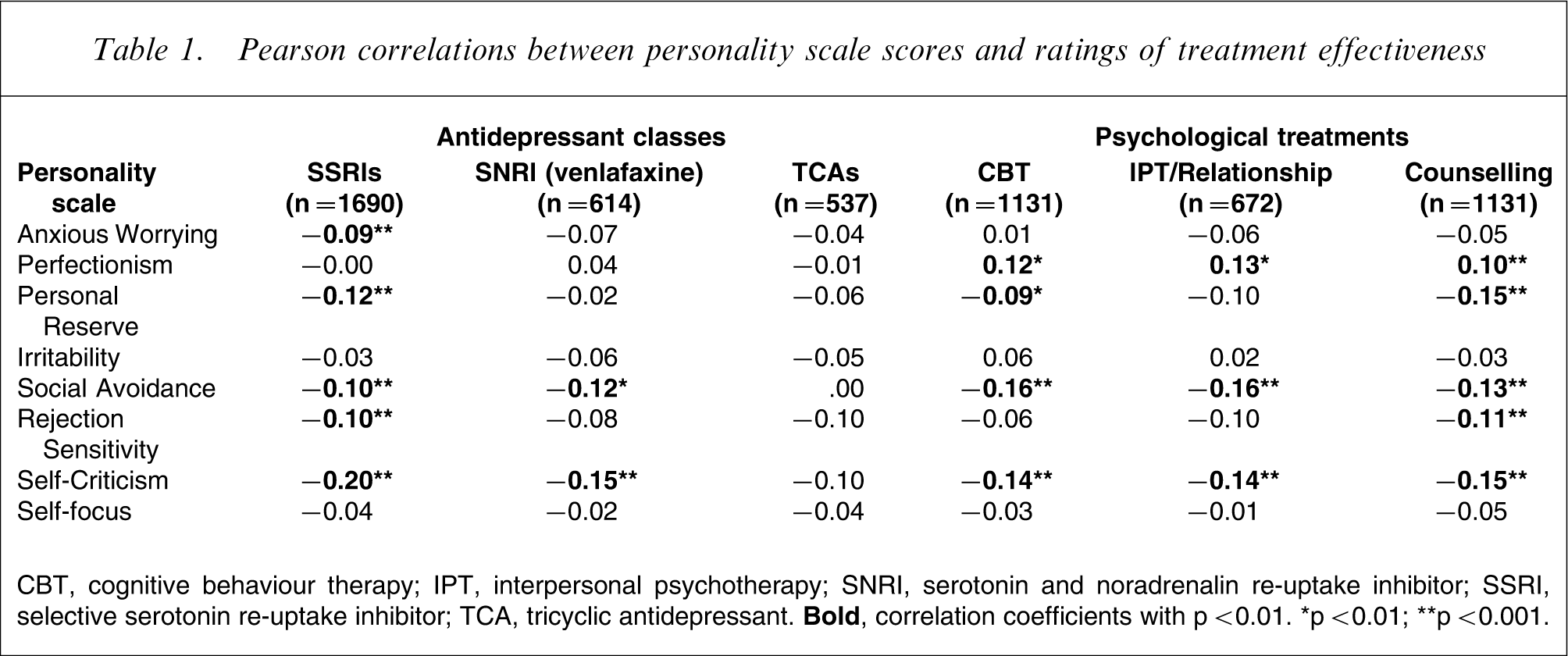
CBT, cognitive behaviour therapy; IPT, interpersonal psychotherapy; SNRI, serotonin and noradrenalin re-uptake inhibitor; SSRI, selective serotonin re-uptake inhibitor; TCA, tricyclic antidepressant.
We then undertook a series of linear regression analyses quantifying the individual impact of each personality style on treatment responsiveness to treatments trialled by ≥100 respondents, and after controlling for the effect of age, gender and all seven other personality style scores. Table 2 summarizes the results of those analyses, including the adjusted R2 values as estimates of the proportion of variance in the treatment effectiveness ratings accounted for by all eight personality dimensions, in addition to age and gender. Overall, very little of the variance in treatment effectiveness ratings was accounted for by the model, ranging from 1% (for TCAs) to 7% (for relaxation therapy).
Linear regressions (β coefficients) for predictors of ratings of treatment effectiveness, for all treatments trialled by ≥100 respondents
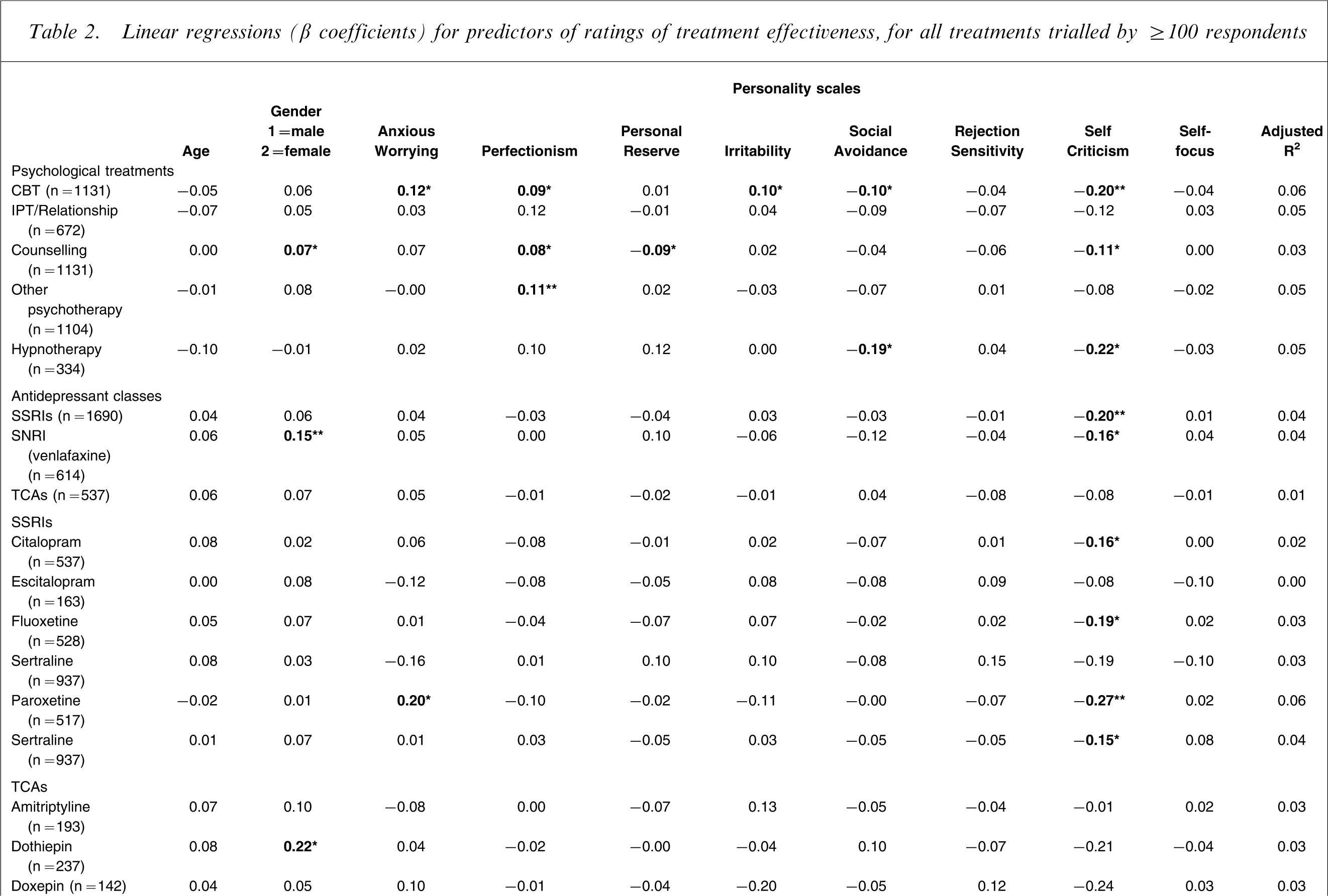
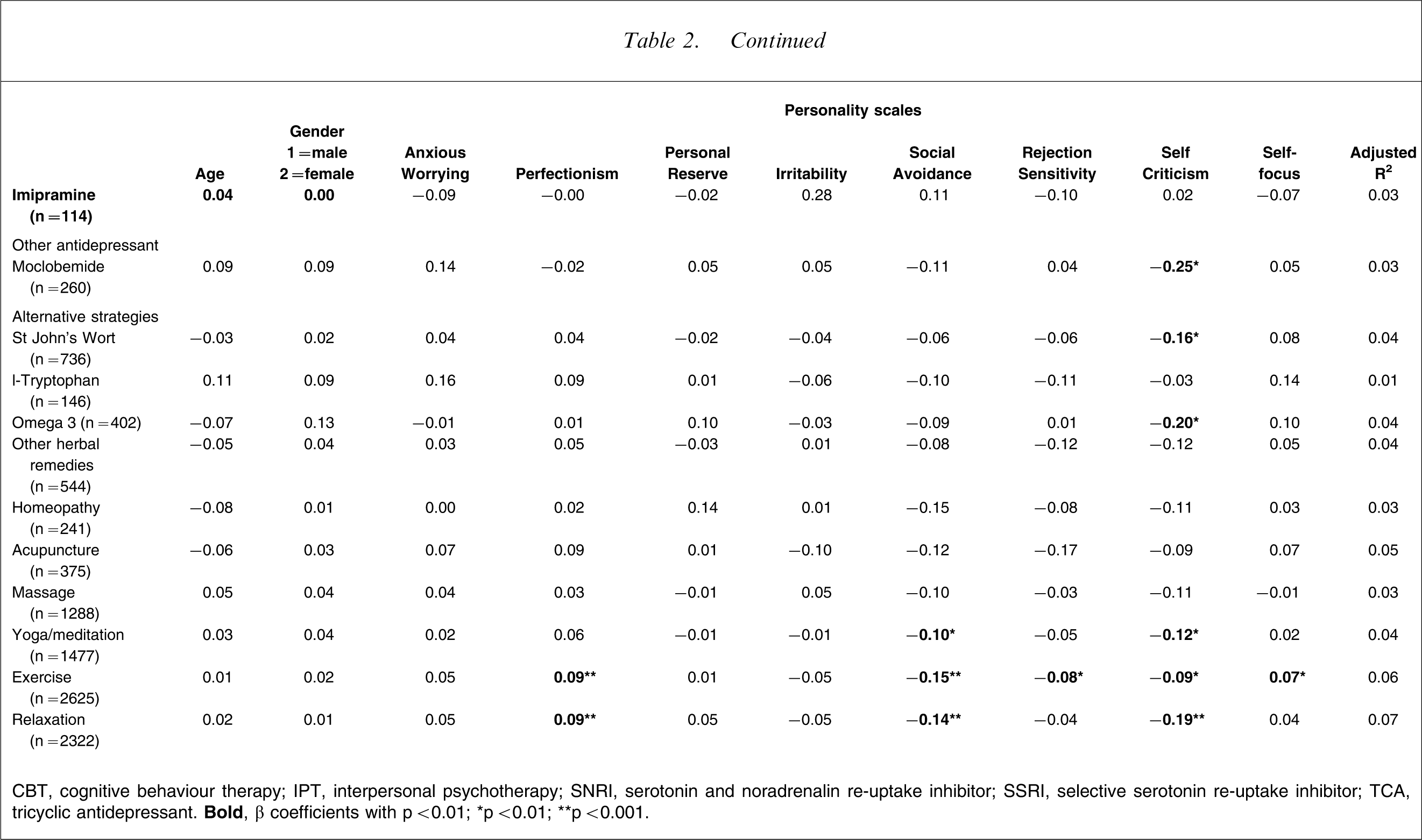
CBT, cognitive behaviour therapy; IPT, interpersonal psychotherapy; SNRI, serotonin and noradrenalin re-uptake inhibitor; SSRI, selective serotonin re-uptake inhibitor; TCA, tricyclic antidepressant.
In essence, subject age was not associated with response to any treatment, when statistically controlling for gender and the eight personality styles. Gender was weakly associated with response to counselling and two antidepressants (venlafaxine and dothiepin), with female subjects reporting a superior response to these treatments. Turning to the eight personality styles, higher ‘anxious worrying’ scores were associated with a superior response to CBT and the SSRI paroxetine. Higher ‘perfectionism’ scores were associated with a superior response to a number of non-drug approaches (i.e. CBT, counselling, ‘other psychotherapies’, exercise and relaxation) but were not associated with all drug therapies. Higher ‘personal reserve’ scores were weakly associated with a poorer response to counselling. Higher ‘social avoidance’ scores were associated with a poorer response to a number of non-drug approaches (i.e. CBT, hypnotherapy, yoga/meditation, exercise and relaxation). Higher ‘irritability’ scores were weakly associated with a superior response to CBT. Higher ‘rejection sensitivity’ scores were weakly associated with a poorer response to exercise, whereas higher ‘self-focus’ scores were weakly associated with a positive response to exercise. Higher ‘self-criticism’ scores were associated with a poorer response to 14 of the 27 individual treatments analysed, and to the class of SSRI antidepressants, and associated with poorer responses to both drug and non-drug responses.
Discussion
There are clearly a number of limitations to this study that require acknowledgment. First, the Web-based sample may limit the extent to which the results can be generalized beyond the current study. Subjects responding to such a survey may well differ from community-based and formal psychiatric samples. We did not apply any diagnostic measure to establish whether individuals met formal criteria for a clinical depressive disorder or depressive subtype. But, because 73% had trialled an antidepressant medication (and more than half had consulted a psychiatrist), we suggest that the majority of the sample would have experienced a major depressive episode. Third, we did not assess depression severity or chronicity. Mulder has suggested limitations to many studies examining personality and depression treatment response as a consequence of their rarely controlling for depression characteristics (e.g. chronicity, severity) that may influence outcome and be related to personality pathology [6]. In addition, data were self-report and retrospective. The validity of retrospective ratings of treatment effectiveness is not as precise as prospective ratings, preferably combined with clinician interview data. We did not establish when they had received specific treatments (risking retrospective recall problems especially for those who had been treated many years previously), nor the adequacy of treatments received (e.g. dose and duration), nor whether treatments were received individually or concurrently with other treatments.
Nevertheless, the Web-based strategy did ensure the large sample necessary to ensure that sufficient data were obtained for representative drug and non-drug antidepressant therapies, with the large sample subsets (in relation to differing treatments) being a distinct advantage to previous studies involving small samples or limiting consideration to single or few personality traits and/or single or few treatment interventions.
Turning to findings, while associations were at best weak, ‘self-criticism’ was the personality domain most consistently associated with a poor response to treatment, and was a consistent finding across drug therapies (i.e. SSRIs and venlafaxine) and three non-drug therapies (i.e. CBT, counselling and hypnotherapy). Specifically, it predicted a poor response to 14 of the 27 examined treatments. While we position ‘self-criticism’ as a personality style (essentially capturing low self-esteem, self-criticism, and relying on others to take control and provide reassurance), it is theoretically the personality dimension most susceptible to inflation by state depression. In a previous paper we reported a correlation of 0.48 between ‘self-criticism’ scales scores and depression severity, and a correlation of 0.27 between change in ‘self-criticism’ and change in depression severity scores (i.e. when state depression decreased, ‘self-criticism’ scale scores also decreased) [9]. Such potential confounding allows three explanations. First, that it is not high ‘self-criticism’ per se that predicts a poor response to antidepressant therapy but higher levels of depression severity. Second, that individuals who score high on such a dimension do not return to a pristine euthymic state but to a level where their personality style is effectively driving some level of ‘trait depression’, so suggesting less benefit from antidepressant strategies. Third, that while depression does inflate ‘self-criticism’ scores to some degree, having a self-critical personality style does predict a generally poorer response to drug and non-drug antidepressant therapies. The latter two explanations would appear more likely.
While previous studies have suggested a poorer antidepressant treatment outcome among patients high in neuroticism [10, 11], the present results did not identify any consistent associations between self-reported treatment effectiveness and high trait anxiety (here assessed as internalized ‘anxious worrying’ and externalized ‘irritability’). Although there was a low, statistically significant negative correlation between mean SSRI class effectiveness scores and ‘anxious worrying’, this association did not hold in linear regressions entering all eight personality scale scores as predictors of individual treatments. Rather, those scoring high on ‘anxious worrying’ were more likely to report a better response to the SSRI paroxetine and to CBT, and those scoring high on ‘irritability’ reported a better response to the SSRI citalopram and the serotonergic TCA imipramine. If those with such high trait anxiety are truly less responsive to antidepressants, or to a class of antidepressants, we might have expected a more consistent inferior response to have been evident across antidepressants examined. The present findings are consistent with results of previous studies that found a lack of association between pretreatment neuroticism and response to the SSRI fluoxetine [12, 13]; but they are inconsistent with a large recent study finding low neuroticism as a significant unique predictor of superior response to combined antidepressant and psychological treatment [7]. One potential explanation for the variation in associations between neuroticism, or related personality dimensions, and treatment response is variation in the time since the treatment trial. As noted in a review by Mulder, most studies finding high neuroticism as a predictor of worse treatment outcome have examined long-term outcomes, whereas those examining short-term response reported more equivocal results [6].
‘Shyness’ is the higher-order domain captured by two subordinate dimensions in our measure (i.e. ‘personal reserve’ and ‘social avoidance’). In the present study, those scoring higher on ‘personal reserve’ reported a poorer response to counselling, and those scoring high on ‘social avoidance’ reported a poorer response to CBT, hypnotherapy and several behavioural interventions (e.g. exercise and relaxation). These results are consistent with our previous findings of higher treatment resistance ratings for depressed patients high on social inhibition [14]. Previously we have also found that social inhibition influences expression of depression, with patients high on this trait reporting the further social withdrawal, reduced help-seeking, and lower perceived social support [14, 15]. It is plausible that these differences may contribute to the reported poorer response to non-drug treatments by those high on introversion.
Perfectionism has previously been associated with poor treatment response. The seminal National Institute of Mental Health study report indicated that those with high levels of perfectionism responded poorly to drug (i.e. imipramine) and two psychotherapies (CBT and IPT) [1, 16]. Such poor response has generally been viewed as reflecting reluctance to form a treatment alliance (reflecting a need to maintain control) and thus trust therapists and presumably benefit from any non-specific benefits of drug therapies. In the present study, however, we found associations between higher levels of perfectionism and superior response to several psychological and alternative therapies (but no drug treatment), somewhat counterintuitive when early literature findings are noted. Dunkley et al., however, have distinguished between dimensions of perfectionism, with a ‘self-critical’ perfectionism more closely associated with depressive symptoms than a ‘personal standards’ perfectionism related to conscientiousness [17, 18]. It is plausible that the ‘perfectionism’ scale in our T&P measure was tapping into conscientiousness, hence its weak association with superior response to treatments requiring active participation (e.g. CBT, counselling and exercise).
Higher rejection sensitivity scores were associated with a poorer response to counselling and SSRIs, but rejection sensitivity was no longer a significant predictor of response to these treatments when the other seven personality traits were statistically controlled for in the linear regressions. We have previously argued that such a personality style is the primary feature contributing to ‘atypical depression’, a depressive subtype held to show a selective response to MAOI drugs [19]. In the present study insufficient numbers of subjects had received an MAOI to provide any valid analysis.
Finally, it is worth noting the overall finding of only a small proportion of the variance in self-reported treatment effectiveness being accounted for by all personality dimensions, in addition to age and gender – in the order of 1–7%. This may be a reflection of the broad retrospective method of assessing treatment effectiveness used in the present Web-based study, and the methodological limitations noted here, but also highlights the role of other possible factors in predicting treatment response (such as depressive subtype, severity etc.).
The limitations to the present study have been noted earlier. Its advantages, however, lie in the large number of subjects surveyed and the breadth of treatments examined, and the data may allow more refined hypotheses for more methodologically rigorous studies. Our principal findings are worthy of some consideration and pursuit. First, a personality style of ‘self-criticism’ emerged as predictive of a poor response to the majority of therapies – including the theoretically most salient treatment (i.e. CBT). Clarification is required to know whether such a poor outcome is underpinned by such a personality style, or whether it emerges more from correlates of those so scoring (e.g. low self-esteem, a higher rate of deprivational and abusive development factors, higher trait and state depression, a greater chance of intrinsic treatment resistance). The present findings are consistent with the conclusion of Mulder's review of personality pathology and depression treatment outcome [6] – namely that the personality constructs found to be the most associated with treatment outcome are also those with the greatest overlap with depressive symptoms – in this case ‘self criticism’. Second, and perhaps the most important finding from the present study, the contribution of personality style to treatment response was overall slight or non-existent. If true, this finding requires close consideration. Although there is a large body of literature indicating a significant contribution of personality style to risk of depression (especially the non-melancholic disorders), the present study suggests a limited contribution to treatment response. If valid, there are important implications in suggesting that (drug and non-drug) antidepressant treatments may act more on the depressive state than on its causative factors (here ‘personality’). This issue requires close pursuit because it argues against treatments necessarily targeting causative factors and more for treatments that focus on the depressed state and essentially ignore any contributing personality style. As for any other counterintuitive finding, this interpretation is worthy of resolution in light of the clear treatment implications.
Footnotes
Acknowledgements
We thank the NHMRC (Program Grant 223708), NSW Department of Health and Pfizer International for funding support, and respondents to the survey.