
Abstract
Jumping is a violent, highly lethal method of suicide, and common in places with high-rise residences, accounting for up to 60% of suicides in countries such as Singapore [1]. Case fatality is estimated at >30% for jumping from all types of structures [2] and at >90% for higher bridges [3–5]. Although, worldwide, most suicides by jumping occur from high-rise residences, a small number of sites, including bridges, develop iconic status as places for suicide. Grafton Bridge in Auckland, New Zealand, is one such site.
Grafton Bridge is a 97.5 m-long concrete arch bridge in central Auckland. The bridge links two major central city roads, rises approximately 80 m above a metropolitan motorway, and has pedestrian pathways on each side. At the recommendation of the then coroner, following suicides from the Bridge, safety barriers were erected in 1937. In 1996 the City Council acted upon community complaints that the barriers were unsightly, vandalized an historic structure, and impeded efforts to rescue people attempting to jump from the bridge. After consultation, the Council decided to remove the barriers with this decision supported by the Ministry of Health. In 2001 we showed that the removal of the safety barriers had resulted in a significant fivefold increase in the number and rate of suicide due to jumping from Grafton Bridge: prior to the removal of barriers only three suicides had occurred during the preceding 4 years, compared to 15 deaths in the 4 years following the removal of barriers [6]. This analysis convinced the City Council to reinstate barriers. New barriers, of an improved, curved glass design, and which extended the full length of the bridge, were installed in 2003. The aims of the present study were to gather data about suicide due to jumping from Grafton Bridge after reinstallation of safety barriers.
Methods
In New Zealand all suspected suicide deaths are investigated by a coroner, with coronial verdicts collated by the Department of Courts. We obtained data about suicide due to jumping from Grafton Bridge from the Department of Court's coronial records, and the mortality database of the New Zealand Health Information Service.
Results
Table 1 shows data for suicide due to jumping from Grafton Bridge for three time periods: (i) 1991–1995, when the original barriers were in place; (ii)1997–2002, when the barriers were removed; and (iii) 2003–2006 when barriers were re-installed. Table 1 lists the number of suicides within each period; the per annum number of suicides; and the per annum rates of suicide per 100 000 of population. Numbers and rates of suicide clearly increased in the period when the barriers were removed, compared to the numbers and rates when the original and new barriers were in place. A χ2 test of the rate of change in the rate of suicide over the three periods showed a highly significant difference between time periods (χ2(2) = 16.9, p < 0.0001). Pairwise comparisons showed that rates of suicide over the period when the barriers were removed were significantly higher than for the original barriers (χ2(1) = 4.8, p < 0.05) and the new barriers (χ2(1) = 14.0, p < 0.0001).
Rates of suicide due to jumping from Grafton Bridge 1991–2006
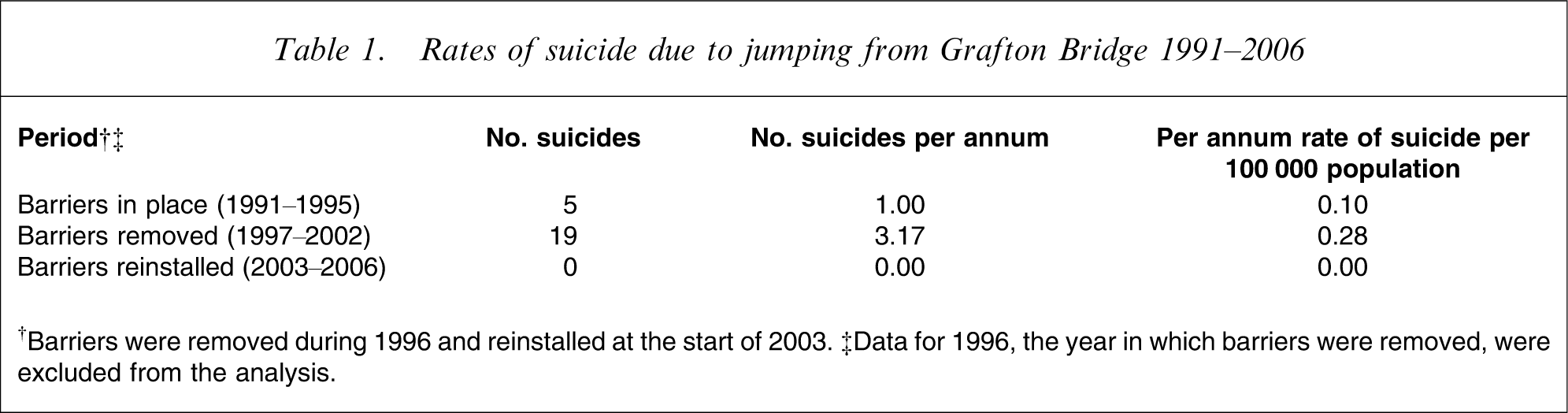
†Barriers were removed during 1996 and reinstalled at the start of 2003. ‡Data for 1996, the year in which barriers were removed, were excluded from the analysis.
All these findings are consistent with a process in which the presence of barriers was associated with a reduction in rates of suicide and the removal of barriers was associated with increased rates of suicide. It can be estimated that had the rate of mortality associated with the original barriers prevailed over the period 1997–2002, this would have led to a reduction in the number of deaths from the bridge during this period from 19 to 6.4. Had the rate of mortality for the new barriers prevailed then all deaths over the period from 1997 to 2002 would have been prevented. These results make it clear that the loss of life due to the removal of barriers from Grafton Bridge was not inconsequential.
Discussion
To our knowledge, nowhere else in the world have safety barriers been removed and reinstated at a known suicide jumping site, providing an opportunity to study the way in which barriers influence suicide rates. Indeed, it has been argued that the ideal epidemiological method for evaluating the effectiveness of safety barriers in reducing suicide by jumping from bridges would be to conduct exactly this experiment, but that, ethically, it could never be done: “Needless to say, this controlled study can never be done, in part because it would be intolerable to wait for a 5- to 7-year period of time to elapse if it was observed early on that there was even a slight increase in the number (let alone rate) of suicides occurring on the bridge once the barriers came down” [7]. In a naturalistic study, the Grafton Bridge ‘experiment’ has used, in effect, a powerful a-b-a (reversal) design: barriers were in place, removed, and then reinstated. The original barriers were old, did not extend across the full length of the Bridge and failed to prevent all suicides. The well-designed replacements extend the entire length of the Bridge and have eliminated suicides.
Few studies have formally evaluated the impact of installing safety barriers at sites that have become popular for suicide by jumping. Placement of barriers on the main span of the Clifton Suspension Bridge in Bristol halved suicides from eight to four per year [3], but barriers did not extend the full length of the bridge, so while suicides from the fenced main span decreased, suicides from the unfenced buttresses at either side of the bridge increased. In Washington DC the installation of barriers at the Ellington Bridge reduced suicides on that bridge (from four per year to one in 5 years), while the number of suicides at the neighbouring Taft Bridge, which remained unfenced, did not change [7].
The present study adds to evidence that the most effective form of prevention at bridge jumping sites is installation of safety barriers. This evidence justifies preventive interventions at sites that become identified for suicide, and suggests that these approaches are now moving towards becoming best practice in suicide prevention. In turn, the development of best practice guidelines for preventing suicide due to jumping raises important issues about the accountability and liability, both of authorities with responsibility for bridges, structures, buildings and other sites from which people jump, and of government agencies accountable for suicide prevention.
Footnotes
Acknowledgements
This study was funded by the Health Research Council of New Zealand.