
Abstract
The Mood Disorder Questionnaire (MDQ) was devised as an easy-to-administer, self-rated, screening tool for detecting bipolar I and II disorders in clinical populations. It has become a widely used tool that has been validated and used in both primary care [1–3] and other health settings [4, 5].
The MDQ was initially validated in a small sample of psychiatric outpatients (n = 198), yielding a sensitivity of 73% and a specificity of 90% for a screening score of ≥7, plus the diagnostic criteria relating to whether the symptoms happened at the same time and the level of functional impairment, relative to the telephone version of the Structured Clinical Interview for DSM-IV (SCID) [6]. A further study investigated the MDQ in a randomly selected group of the general population (n = 711). The MDQ was found to have a sensitivity of 28% and a specificity of 97% in comparison to the SCID [7]. Sensitivity was considerably less in the general population study than in the study of psychiatric patients. A version of the MDQ has also been validated in adolescent outpatients and has a sensitivity of 72% and specificity of 81% for a score of ≥5 when rated by parents [8].
Translations of the MDQ have recently been validated. A Spanish version was validated by comparing psychiatric outpatients with healthy controls and had a specificity of 95% and sensitivity of 81% [9]. A validation of a French version reported sensitivity of 90% for bipolar I disorder and 52% for bipolar II disorder and an overall specificity of 91% [10]. A sensitivity of 76% and specificity of 86% was reported for an Italian version of the MDQ when a cut-off score of ≥6 was used [11]. In a study utilizing a clinical population presenting with a current depressive episode, Kim et al. found that the MDQ had a sensitivity of 29% and a specificity of 77% for bipolar diagnosis using the standard scoring, and that the results of the MDQ were improved when scoring was modified by discarding items on functional impairment and symptom co-occurrence [12]. Carta et al. compared the Italian version of the MDQ and the Hypomania Checklist (HCL-32) with the SCID and found good sensitivity and specificity for both screening tools, but the HCL-32 was more sensitive for detecting bipolar II disorder [13]. The MDQ has also been validated in other languages including Finnish [14] and Turkish [15].
The validation studies demonstrate that although the MDQ has a high specificity, indicating that few people who screen positive on the MDQ do not have bipolar disorder, there are potential problems with the sensitivity of the MDQ, suggesting that many people with bipolar disorder may fail to screen positive. This is a general problem in retrospective recognition of disorders with a remittent/recurrent course. The widespread use of the MDQ in epidemiological studies may therefore result in potential inaccuracy in reported prevalence rates of bipolar disorder [16]. An explanation for the discordance of the SCID and MDQ suggests that people who experience only hypomania or mixed mania but never full manic episodes often fail to screen positive [13, 17]. It has also been suggested that the low sensitivity of the MDQ is due to a low test–retest reliability of the SCID, which has been used as a comparator in most studies conducted [7], although it has been argued that the kappas for test–retest reliability for the MDQ are satisfactory [10].
Nevertheless, the MDQ remains a widely used tool by researchers and clinicians in a variety of contexts. The aim of the present study was therefore to investigate the reliability of the MDQ relative to the Structured Clinical Interview for DSM-IV-TR Research Version, Non-patient edition (SCID) in a large community-based sample of adult women.
Methods
Participants
This study included data collected from women participating in the Geelong Osteoporosis Study (GOS), a large epidemiological study involving age-stratified community-based samples of women randomly recruited from the electoral roll for the region (Barwon Statistical Division, South-Eastern Australia). The initial sample was recruited between 1994 and 1997, with 1494 women (median age = 54 years, interquartile range (IQR) = 37–72) agreeing to participate [18]. Data on medical and lifestyle factors have been collected at baseline and biennial follow-up assessments. Invitations for participation in the 10 year follow up of the GOS were sent to each eligible subject. A further cohort of 200 women aged 20–29 years was also recruited at the time of the 10 year follow up. Exclusion criteria included an inability to provide informed consent; death; or inability to be contacted. Height, weight and other clinical assessments were taken, while a series of detailed questionnaires was administered. Following the clinical assessments and questionnaires, a different member of the research team conducted the psychiatric assessment.
From a potential pool of 1117 women, enrolled in the GOS at the time of the study, 23 women who did not participate in the clinical interview and a further 28 who had not completed the MDQ were excluded from the analyses, resulting in a sample of 1066 women (95%) aged 21–94 years eligible for inclusion. Barwon Health Research and Ethics Advisory Committee approved the study, and participants provided informed, written consent.
Clinical assessments
Psychiatric status was assessed using the SCID-I/NP [19]. The SCID-I/NP was used to identify those who had ever experienced a depressive disorder, including bipolar disorder (I, II and not otherwise specified or NOS), major depressive disorder, minor depression, dysthymia, mood disorder due to a general medical condition and substance-induced mood disorder and/or any anxiety disorder. All psychiatric interviews were conducted by trained personnel who were blind to the results from the MDQ screen.
The MDQ is a self-report screening instrument for detecting previous mania and hypomania, characteristic of bipolar I and II disorders, respectively [6]. The MDQ includes 13 questions relating to manic or hypomanic symptoms derived from DSM-IV criteria plus a further two items assessing the temporal clustering of symptoms and functional impairment. This questionnaire has been used and validated in both primary care and community settings [1, 7]. Trained researchers also gathered data regarding demographic, lifestyle, medical, and other parameters during the assessment. Socioeconomic status was measured using Socio-Economic Index For Areas (SEIFA) scores. Individuals were assigned a SEIFA index score based on their address. Scores ranged from low (1) to high (5), corresponding to quintiles in the Barwon Statistical Division. Education (highest level completed) was self-reported, as was medication use, current smoking and country of birth.
Statistical analysis
Descriptive statistics for the sample population were completed using Minitab (Version 15; Minitab, State College, PA, USA). Other statistical analyses were completed manually using a 2×2 table of association as described by Zimmerman et al. [20]. Calculations for the MDQ relative to the SCID-I/NP included sensitivity, which measures the proportion of persons with a confirmed diagnosis of bipolar disorder (I, II or NOS) using the SCID who also screen positive using the MDQ; specificity, which measures the proportion of persons without bipolar disorder who also screen negative using the MDQ; positive predictive value, which measures the proportion of persons who screen positive using the MDQ who have bipolar disorder; negative predictive value, which measures the proportion of persons who screen negative using the MDQ who do not have a SCID diagnosis of bipolar disorder; and the overall level of agreement (kappa), which measures the proportion of persons correctly classified on the MDQ.
Results
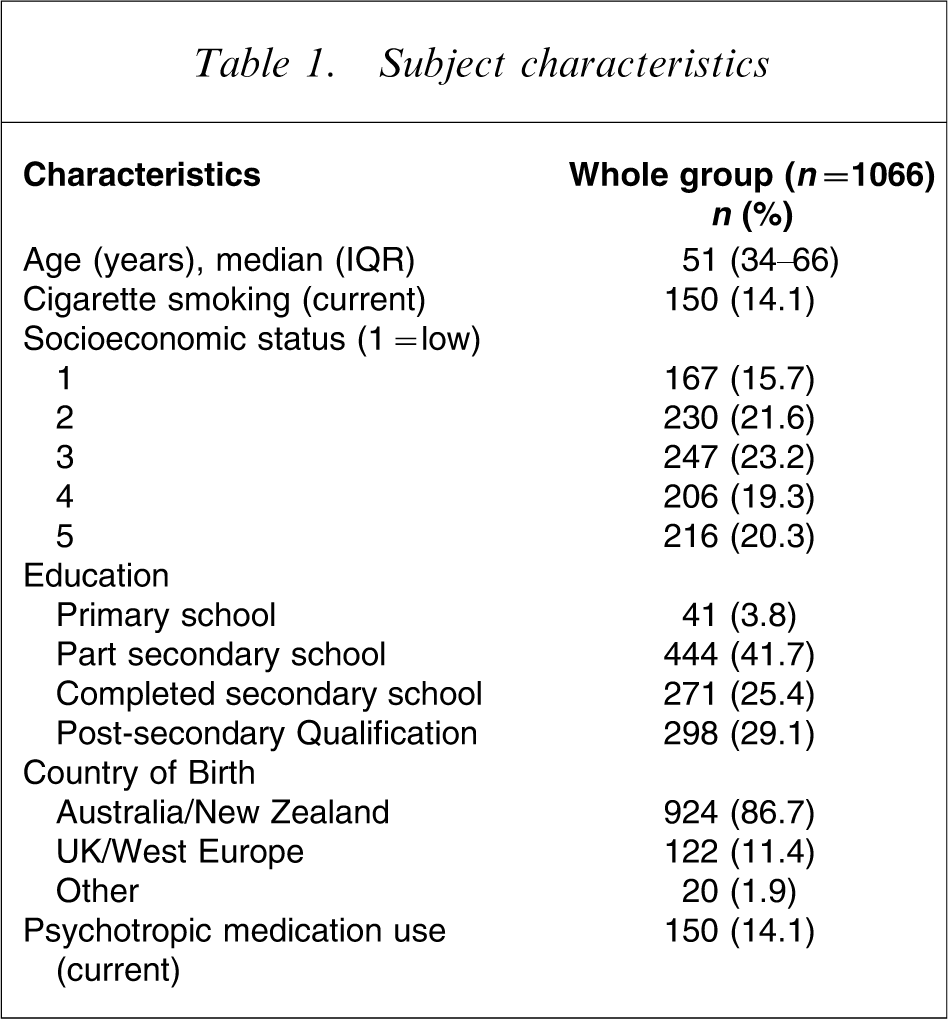
Data were collected from 1066 women using both the MDQ and the SCID. The median age of the sample was 51 years (IQR = 34–66 years) and 362 (34%) met lifetime criteria for any psychiatric disorder. Characteristics of the group are reported in Table 1.
Subject characteristics
For those diagnosed via SCID with bipolar disorder, the median age was 42 years (IQR = 30–52 years). Ten (42%) were identified with bipolar I, 11 (46%) bipolar II and three (13%) with bipolar NOS. The median age of onset was 20 years (IQR = 16–37 years) and the median duration since onset at the time of the SCID was 11 years (IQR = 5–21 years). Fourteen (58.3%) were suffering from a current depressive or manic/hypomanic episode and nine (38%) were medically untreated at time of interview.
From the full sample of 1066 women there were 21 women (2%) who scored positive for bipolar disorder using the MDQ, and 24 women (2%) were identified as having a diagnosis of bipolar disorder using the SCID. Six of the 24 women (25%) identified as having bipolar disorder using the SCID also scored positive using the MDQ. Of these six women, five (83%) were diagnosed with bipolar I disorder and one (17%) was diagnosed with bipolar disorder NOS. Of the 15 (71%) remaining women who scored positive using the MDQ, seven were identified having a SCID diagnosis of major depressive disorder, of which two had current major depressive disorder, four were identified with minor depression, two had social phobia and two had no current or past history of psychopathology.
Compared to the SCID, the sensitivity for the MDQ was 25%, specificity 99%, positive predictive value 28%, negative predictive value 98% and the overall level of agreement (kappa) was 0.25.
Discussion
The overall level of agreement between the MDQ and the SCID was low; the MDQ could identified only 25% of women in the study population with a confirmed diagnosis of bipolar disorder. Values of sensitivity for the MDQ vary widely between studies conducted by different research groups, ranging from >70% when used in some patient populations [5, 6, 21, 22], with lower sensitivity between 40% and 70% in other studies of patient populations [9, 23], and a low sensitivity of 23% in the general population [7]. In the present study the sensitivity was 25%, which is concordant with the previous general population study. In several studies the MDQ demonstrated a higher sensitivity for bipolar I disorder than for bipolar II disorder or bipolar disorder NOS. This observation was also found in the present study, with the MDQ failing to detect any of the women confirmed with bipolar II disorder (n = 11) and the two women identified with bipolar disorder NOS using the SCID. It is the case that, although symptom severity and construct validity of bipolar I disorder is high and both relatives and clinicians quickly become aware of the symptoms, this is not the case for bipolar II disorder. A low prevalence and subthreshold manic symptoms combined with low symptom awareness complicate the detection of bipolar II disorders. The fact that mild or moderate hypomania is often perceived as positive and healthy episodes (symptom attribution) in persons who have experienced depressive episodes earlier, is a well-known challenge for clinicians. Equally, some individuals appear to endorse symptoms of mood elevation that are not clinically salient.
Limitations of the study include the sample size; only the expected percentage of the community sample of 1066 women was diagnosed on the SCID as being positive for a diagnosis of bipolar disorder. The present study may not be extrapolated to clinical populations, because clinical populations may well have different experiences of mood symptoms that may lead to them responding in a different manner to this questionnaire. A further limitation is that the present study was conducted in women, and these results may not be generalized to male subjects. Das et al. screened 1157 patients in a primary care setting using the MDQ and found significant differences in positive screening rates for bipolar disorder by gender [2].
The present study suggests that the MDQ may not be a useful screening tool in a non-clinical population to detect bipolar disorder, because it would miss as many as 75% of cases. Reliable screening tools to detect bipolar disorder in clinical and community populations are of overt value, and the development of novel tools and refinement of existing instruments is warranted.
Sources of support
The present study was funded by the National Health and Medical Research Council of Australia and supported by an unrestricted educational grant from Eli Lilly. Postgraduate scholarships were provided by the University of Melbourne, Faculty of Medicine, Dentistry and Health Sciences and the Australian Rotary Health Research Fund. The sponsors played no role in the design or conduct of the study; collection, management, analysis, and interpretation of the data; or in preparation, review, or approval of the manuscript.