
Abstract
Since Kraeplin's and Bleuler's descriptions of schizophrenia, the presence of depressive symptoms in the disorder has been widely reported [1–6]. The depressive syndrome in schizophrenia has received increasing attention because of its significance in diagnosis, treatment and outcome [2, 7–9]. Because there were different objects or methods in those studies, the rates of depression in the course of schizophrenia have been found to vary widely (25–80%) [1, 2, 4, 5, 10, 11]. Because the identification of depressive symptoms in schizophrenia patients is difficult, several methodological problems require discussion: (i) there are marked overlaps between the signs and symptoms of depression and negative or extrapyramidal symptoms [12]; and (ii) standard depression rating scales such as the Hamilton Depression Rating Scale (HDRS) and the Montgomery–Åsberg Depression Rating Scale (MADRS) have been designed and developed for non-psychotic patients and do not perform well with schizophrenia patients [13, 14].
To overcome this problem, the Calgary Depression Scale for Schizophrenia (CDSS) was developed by Drs D. Addington and J. Addington at the University of Calgary. The scale was specifically developed to assess the level of depression in schizophrenia. It has been extensively evaluated in both relapsed and remitted patients and appears sensitive to change. The scale is derived from the Present State Examination (PSE) and the HDRS, and assesses symptoms of depression at any stage of schizophrenia.
The scale has been validated in several studies and has shown high reliability and satisfactory validity as well as methodological superiority when compared to the HDRS and the MADRS [15–19]. The CDSS is now translated into 29 languages and has been adapted and validated for use in Mexico, Brazil, France, Germany, and Greece, among others [20–24].
The purpose of the present study was to test the reliability and validity of the Chinese version of the CDSS (CDSS-C) in identifying depressive episodes in patients with schizophrenia in China.
Method
Sample
Twenty-six schizophrenia patients were included in the reliability study, while 101 were included in the validity study. The subjects were inpatients from four mental health units in China between January and May 2007. They fulfilled the DSM-IV (American Psychiatry Association) diagnostic criteria for schizophrenia and had given their consent to take part in the study. The subjects in the four mental health units were enrolled randomly. Patients with a current history of alcohol or substance abuse, any decompensated organic disorder (especially neurological), mental retardation, significant clinical pathologies that could be associated with depression, and subjects whose native language was not Chinese were excluded from the study.
Procedure
The CDSS was translated from original English into Chinese by three psychiatrists who were bilingual in English and Chinese. A final consensus version was discussed in a panel with clinical experienced colleagues. The nine items of the scale were checked item by item and the modifications proposed were added. The final version was back-translated into English by another psychiatrist who was bilingual and fluent in English Chinese, working independently. The English back-translated version of the CDSS was sent to Prof. D. Addington, author of the original version of the CDSS, to examine whether the precise meaning of the English had been successfully conveyed.
Each patient was assessed on the same day by two independent psychiatrist-raters. The first rater evaluated patients eligible for the study and applied a questionnaire on sociodemographic data, clinical data, and psychiatric history. Diagnosis of schizophrenia according to DSM-IV criteria was confirmed. He also administered the following scales: the Positive and Negative Syndrome Scale (PANSS), the HDRS-24, the Simpson–Augus rating Scale (SAS), and the Barnes Acathisia Rating Scale (BARS). The second rater without any information from the previous interview applied the CDSS-C.
In order to assess the CDSS-C inter-rater reliability, 26 patients were simultaneously rated by two investigating psychiatrists who worked independently. As to test–retest validity of the CDSS-C, some of the assessments (in 26 patients) involved the same investigator making two ratings separated by an interval of no more than 3 days. All raters had sufficient clinical experience and had received formal and specific training on the use of the scales. Examiners acquired sufficient experience in the administration of the CDSS-C within 5–10 practice interviews, and an internal concordance of 0.80 was the minimum required.
Statistical analysis
SPSS software (version 13.0 for Windows; SPSS, Chicago, IL, USA) was used for statistical analysis. Internal consistency was tested with Cronbach's alpha coefficient. Inter-rater consistency was tested by means of the kappa coefficient. Intra-rater reliability was analysed using test–retest comparison. Construct validity was investigated using the Pearson product–moment correlation coefficient between the CDSS-C scores and the scores obtained with the HDRS-24, the G6 item (depression) of the PANSS, the positive and negative subscales of the PANSS, the general psychopathology subscale of the PANSS, the total score of the PANSS, the SAS and the BARS. To evaluate the diagnostic validity of the three depression scales (CDSS-C, HDRS-24, PANSS-G6), the area under the receiver operating characteristic (ROC) curve was obtained and compared with MedCalc (version 7.0; Medcalc Software, Mariakerke, Belgium). The significance level was set at 0.05.
Results
Sample characteristics
The study population consisted of 101 inpatients from four mental health units in two cities. All patients met the DSM-IV criteria for schizophrenia. Thirty-five were female (35%) and 66 were male (65%). Their mean age was 34.1±10.0 years old, and age of onset was 34.6±8.5 years. Mean duration of disease was 10.2±8.6 years, and duration of treatment with neuroleptics was 9.3±7.6 years. All patients were being treated with neuroleptics at the time of their inclusion in the study. The total scores on the PANSS, HDRS, CDSS-C, SAS and BARS were 75.5±16.3, 17.9±9.3, 6.1±4.3, 1.4±2.0 and 1.9±2.5, respectively (Table 1).
Subject data
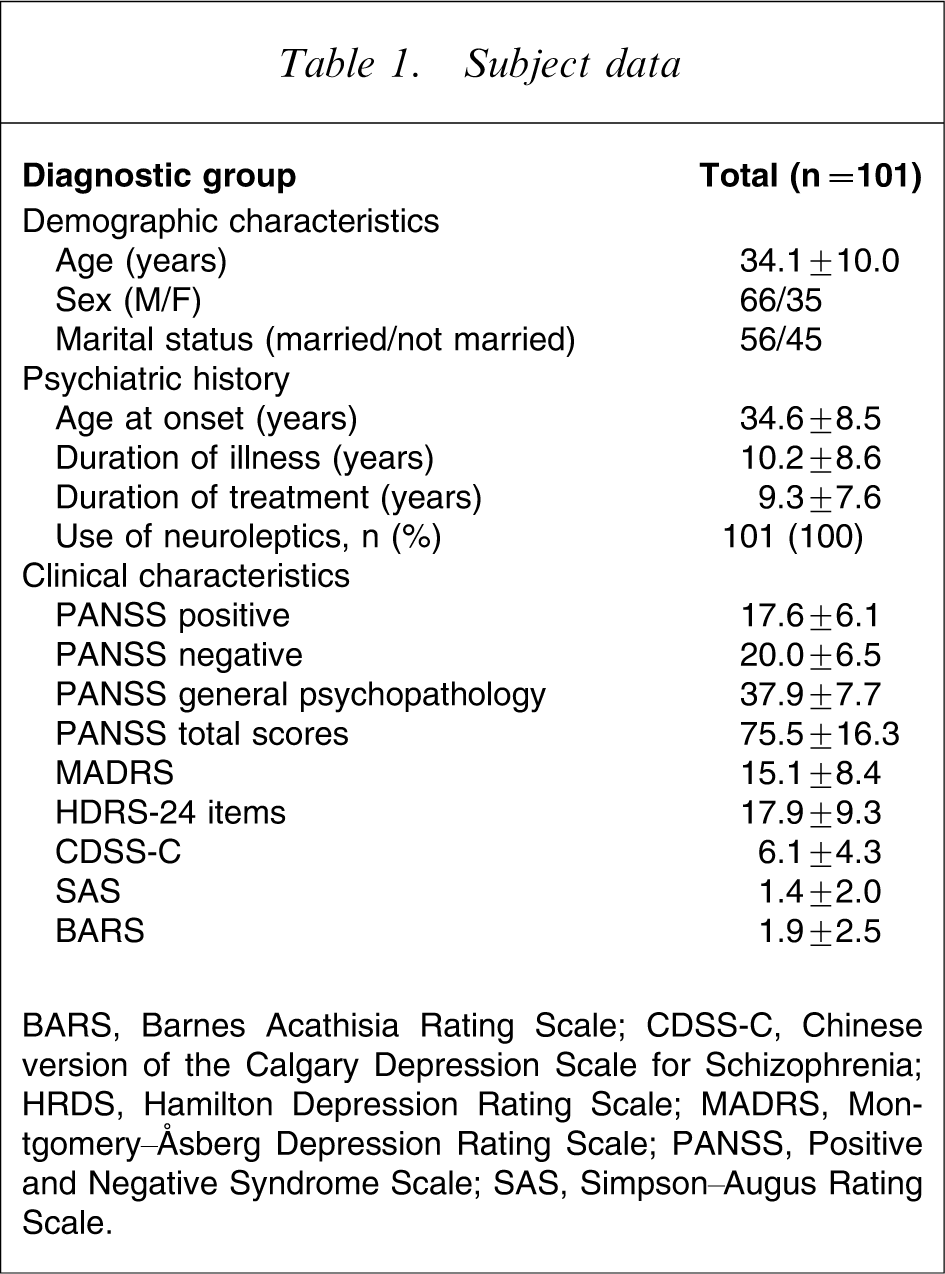
BARS, Barnes Acathisia Rating Scale; CDSS-C, Chinese version of the Calgary Depression Scale for Schizophrenia; HRDS, Hamilton Depression Rating Scale; MADRS, Montgomery–Åsberg Depression Rating Scale; PANSS, Positive and Negative Syndrome Scale; SAS, Simpson–Augus Rating Scale.
Reliability of the CDSS-C
Inter-rater reliability was tested on a sample of 26 patients who were typical of the population. As assessed for each of the items, the inter-rater reliability was found to be high (κ coefficient >0.79; Table 2). The test–retest reliability was also high, with r = 0.927 (p < 0.001) for the total score of the CDSS-C. The internal consistency of the CDSS-C using Cronbach's alpha was 0.804. All the items are necessary for the construction of the scale except for item 4 (Guilty ideas of reference), item 6 (Morning depression) and item 7 (Early morning waking; Table 3).
Inter-rater reliability of the CDSS-C
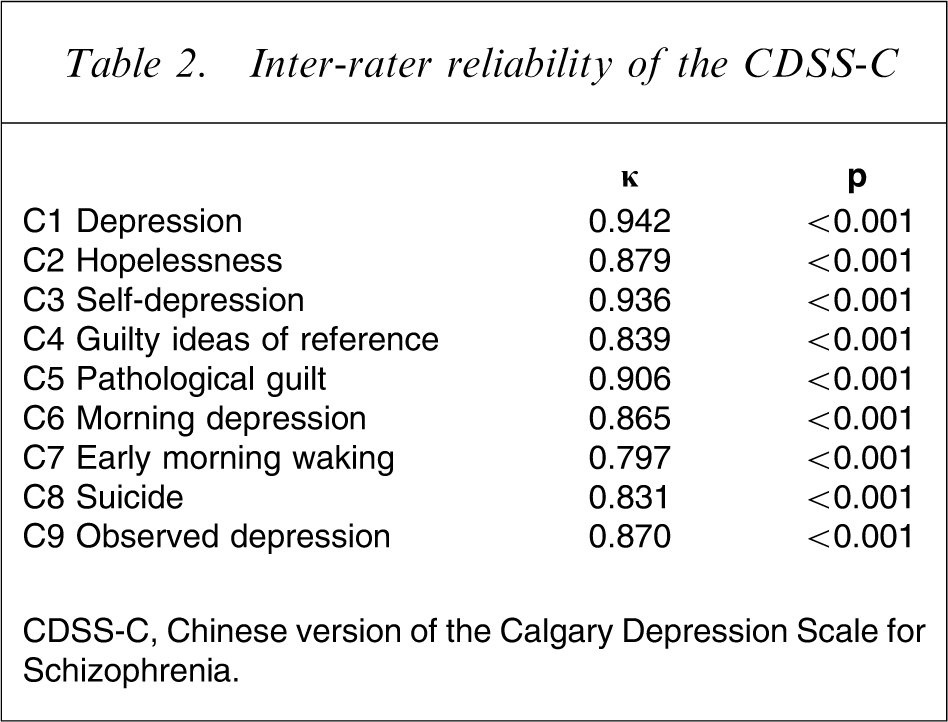
CDSS-C, Chinese version of the Calgary Depression Scale for Schizophrenia.
Internal reliability of the CDSS-C
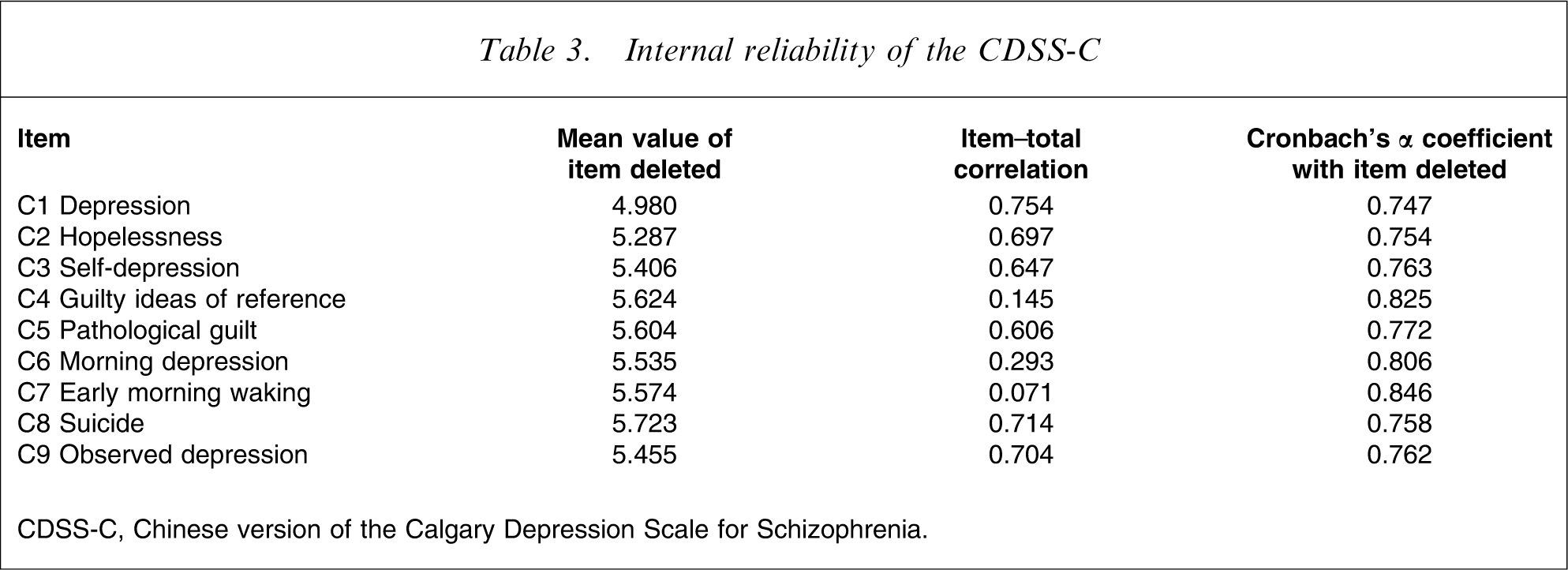
CDSS-C, Chinese version of the Calgary Depression Scale for Schizophrenia.
Validity of the CDSS-C
The CDSS-C showed a significant correlation with the HDRS-24 (r = 0.862, p<0.01), and the depression item (G6) of the PANSS (r = 0.830, p < 0.01). In contrast, the CDSS-C had significant weak correlations with the general psychopathology of the PANSS (r = 0.445, p < 0.01), but showed no correlation with the positive subscale of the PANSS (r = −0.018, p > 0.05), the negative subscale of the PANSS (r = 0.110, p > 0.05), the SAS (r = 0.077, p > 0.05) or the BARS (r = 0.182, p > 0.05; Table 4).
Validity of the CDSS-C
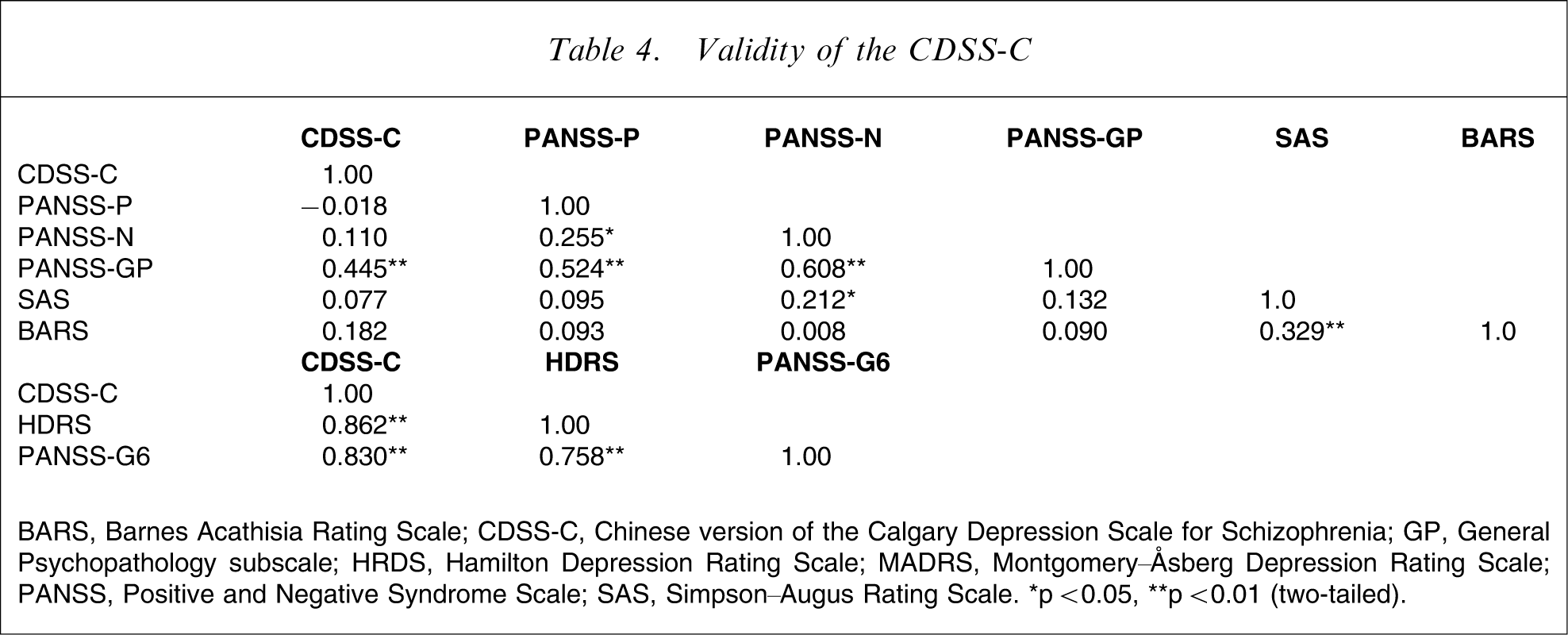
BARS, Barnes Acathisia Rating Scale; CDSS-C, Chinese version of the Calgary Depression Scale for Schizophrenia; GP, Genral Psychopathology subscale; HRDS, Hamilton Depression Rating Scale; MADRS, Montgomery–Åsberg Depression Rating Scale; PANSS, Positive and Negative Syndrome Scale; SAS, Simpson–Augus Rating Scale. ∗p < 0.05, ∗∗p < 0.01 (two-tailed).
As shown in Figure 1, the areas under the ROC curves of the CDSS, HDRS-24 and PANSS-G6 against the DSM-IV criteria for major depressive episode were 0.954, 0.870 and 0.932, respectively. The area under the ROC curve of the CDSS was significantly greater than that of the HDRS (p = 0.013, <0.05) and PANSS-G6 (p = 0.032, <0.05). The most suitable cut-off score to discriminate between depressed and non-depressed patients was 5, with a sensitivity of 84.3%, specificity of 96.8%.
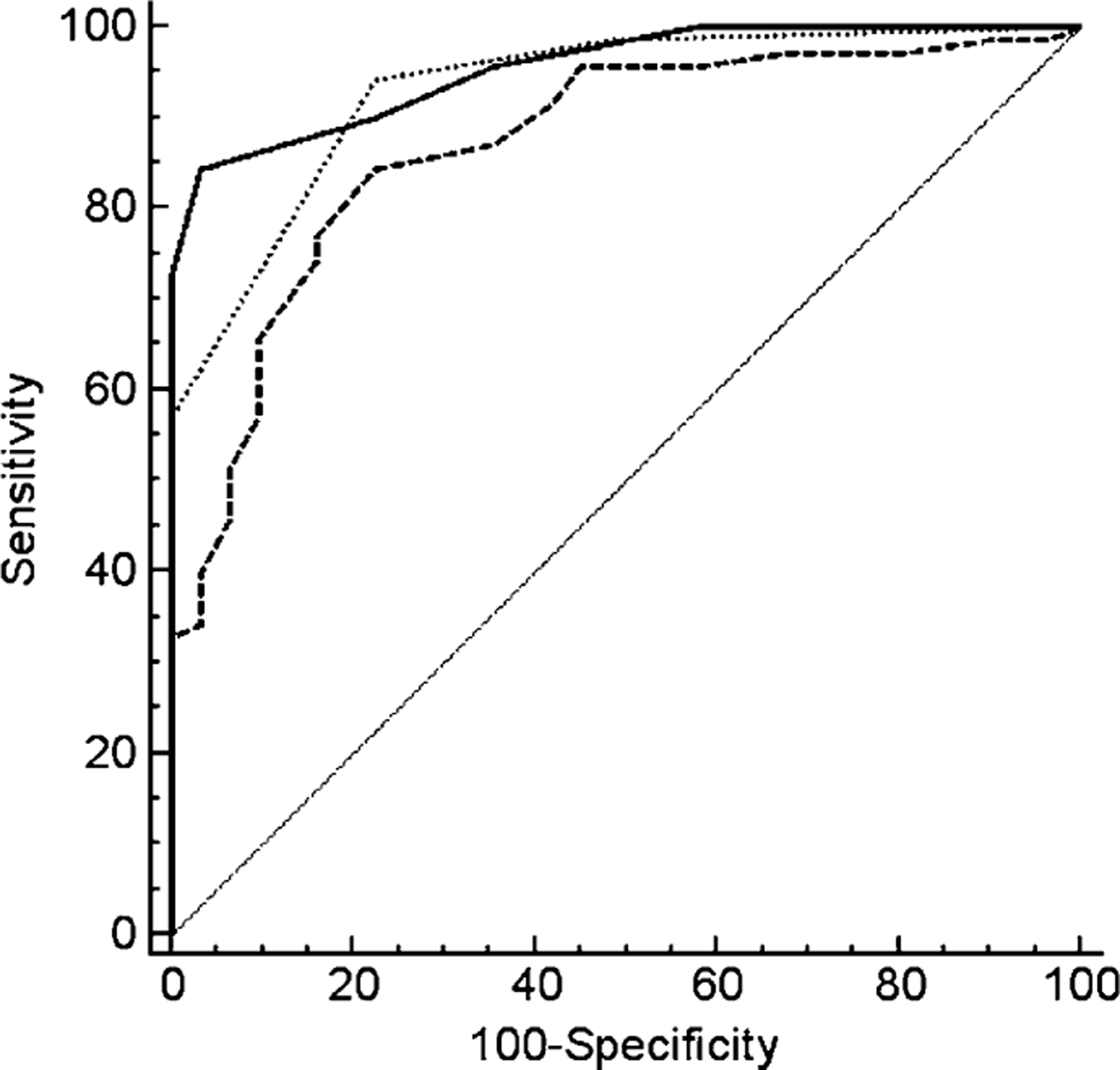
Receiver operating characteristics curve for (
Discussion
The purpose of the current study was to present the cross-cultural adaptation of the CDSS in a Chinese population as well as to assess the psychometric potential of the CDSS-C with regard to reliability and validity. A total of 101 inpatients in different stages of schizophrenia were evaluated for depression, and 71.3% of them fulfilled DSM-IV criteria for depressive disorder without other specification, while 16.8% fulfilled criteria for major depressive episode. These percentages are in agreement with results of other studies but are clearly higher than those expected for the prevalence of depression in the general population [25, 26]. These findings demonstrate that depressive episodes are frequent in the course of schizophrenia [7].
There was a high inter-rater reliability of the CDSS-C (κ > 0.797). These results are similar to those obtained for the French, Greek and Spanish versions of the CDSS [22, 24, 27]. None of the items was inconsistent between the raters. This is mainly due to the structured form of the interview and the presence of strict criteria for the definition of items.
Although there are a number of factors such as progression of the disease and therapeutic strategies that may affect the stability over time of psychopathological scales in clinical practice, test–retest reliability of the CDSS-C was very good (r = 0.927) and higher than that reported by Bernard et al. [22].
Internal consistency of the CDSS-C was good (α = 0.80). Other reliability and validity studies of the CDSS confirmed the high consistency of the instrument including a Brazilian version (α = 0.80), a French-language version (α = 0.82), a Japanese version (α = 0.82), a Greek version (α = 0.87), and a Spanish version (α = 0.83) [21, 24, 27–29]. All of the items are consistent with one another, except for items C4 (guilty ideas of reference) C6 (morning depression) and C7 (early wakening), that showed no correlation with the remaining items nor with total CDSS-C score. Internal consistency of the scale may be improved by excluding C4, C6 and C7 items. These results are similar to those studies for the French language version and the Spanish version [27, 29]. The low item/total correlation for items C4, C6 and C7 may be related in part to the sample of subjects selected, progression of disease and usage of hypnotics or antipsychotic drugs and so on.
The validity of the CDSS-C was also supported by the present results. There were positive correlations among the CDSS, the HDRS and the PANSS-G6. This finding indicates that all these scales have the ability to detect depressive symptoms in patients with schizophrenia. Other authors have also reported positive correlations between the CDSS and several instruments measuring depressive symptoms, such as the MADRS; PANSS-D, including the items of somatic concern (G1), anxiety (G2), guilty feelings, (G3) and depression (G6) [15, 17, 21, 22].
In the results reported by Bressan et al. and Kontaxakis et al., a positive correlation between CDSS-C and the subscale of PANSS in schizophrenia patients was observed [21, 24]. In the present study we did not find such a correlation; instead a negative but not significant correlation between the CDSS and the PANSS positive subscale was found, which was similar to the results of the Kontaxakis et al. study [24]. Bressan et al. reported no correlation between the CDSS score and the negative subscale of PANSS (PANSS-N) score, and a statistically significant correlation between the CDSS-C and the general psychopathology subscale of PANSS (PANSS-GP) score [21]. Kontaxakis et al. reported no correlation between the CDSS score and the PANSS-N score, and a weak correlation between the CDSS-C and the PANSS-GP score [24], while Sarro et al. reported a weak correlation between the CDSS-C and the PANSS-N score, and the PANSS-GP score [27]. In the present study we found no correlation between the CDSS score and the PANSS-GP score, which means that the CDSS-C is an effective tool to different the depressive symptoms from the negative symptoms of schizophrenia patients. In the present study we also found a significant weak correlation between the CDSS score and the PANSS-N score, which was attributed to a stronger correlation between CDSS and PANSS-GP ‘depressive cluster’ scores, including the items of depression, anxiety, guilt feelings and somatic concern (r = 0.256, p < 0.05) [24].
In the validity study of the Brazilian version of the CDSS, a weak correlation with Extrapyramidal Symptom Rating Scale was found [21]. In the present study a significant correlation between CDSS-C and extrapyramidal symptoms was not found, which is similar to results of the Addington et al. and Collins et al. studies [18, 30]. This means that the CDSS-C is an effective tool to different the depressive symptoms from motor side-effects of schizophrenia patients.
The area under the ROC curve showed that the CDSS-C was more effective than the HDRS-24 and PANSS-G6 for evaluating depressive symptoms in schizophrenia. The most suitable cut-off score in the present study was 5 because it offered the best sensitivity, specificity, and positive and negative predictive values.
The present study has several methodological limitations. First, the study subjects were inpatients, and the assessment of depressive symptoms in schizophrenia outpatients need further study; second, all subjects were treated with antidepressants; finally, subjects in acute episode and in restoration period were all included in the present study. Further studies that include a diverse patient population will be better able to evaluate depression in patients with schizophrenia.
In conclusion, the CDSS-C is a valid and reliable scale for the assessment of depression in schizophrenia patients.
Footnotes
Acknowledgements
We are indebted to Dr Donald Addington for his authorization and helpful suggestions during the validity study of the CDSS-C; to Professor Xu You-xin and Dr Sheng Li for their back-translation into English, and to Professor Zhang Dai for his work on the manuscript. This work was supported by Institute of Mental Health, Peking University.