
Abstract
Dropout from child and adolescent mental health service is problematic for many reasons. Not only might individuals who would benefit from available treatment not receive that treatment, there may be long-term costs for the child, family and society because unresolved psychological difficulties may predispose the child to subsequently grow up to become a malfunctioning adult [1]. From an economic viewpoint, dropout represents a poor return on resources already invested in the individual in terms of intake procedures, assessments, treatment planning, and treatment delivered up to the point of dropout, which themselves may have denied or delayed access to services by other needy patients.
Clearly, the identification of any measures that could reduce dropout would be useful, and the first step may be to establish factors associated with dropout. Research on dropout to date, however, has produced findings that are far from definitive, partly because dropout is defined differently across studies [2], partly because studies across disorders may mask factors associated with any particular disorder, and partly because findings relating to one disorder may not be generalized to other disorders.
The need to examine dropout in relation to specific disorders is apparent in findings that there are different rates of dropout from child and adolescent services across diagnostic groups. For example, children experiencing family problems or conduct disorder and attention-deficit–hyperactivity disorder (ADHD) are more likely to drop out from treatment than those with other disorders, and those experiencing negative life events, anxiety disorders or those not having a diagnosis are less likely to drop out [3]. Because, for example, parent and family characteristics (e.g. socioeconomic status, parent marital status) can vary systematically by childhood problems [4], it may be that diagnosis-specific variables are associated with dropout. If they can be identified at the point of diagnosis, then preventative strategies could be implemented to reduce the risk of dropout.
Research to date has identified a wide variety of factors associated with dropout from child and adolescent mental health services [5–7]. For example, among children with conduct problems, perhaps the most studied disorder in relation to dropout, younger mothers and/or single parents, socioeconomic disadvantage, life stress, adverse life events, previous treatment, symptom duration, waiting time, referral source and parental pathology have been associated with dropout [6]. There has been little research, however, specifically to identify the factors associated with dropout from treatment for children with other disorders.
In the present study we set out to investigate whether the variables identified with dropout in previous studies may be differentially operative according to diagnosis. In light of the previous research on dropout, we expected that sociodemographic factors such as parental status would be associated with dropout. Although the literature identifies these as general factors with a special relevance to children with conduct problems, little is known about factors related to other disorders.
Method
The study reported here builds on a previous study on the different rates of dropout between diagnostic groups [3]. It utilized data retrieved from a file review of all cases referred to the community clinics of a public Child and Adolescent Mental Health Service (CAMHS) in Melbourne, Australia. This government-funded programme provides a tertiary-level service to children and young people up to the age of 18 years who are displaying psychiatric symptoms, severe emotional and/or behavioural disturbance. It is available to families who reside in the central and outer eastern region of Melbourne, reflecting patients who are largely of lower-middle class socioeconomic status.
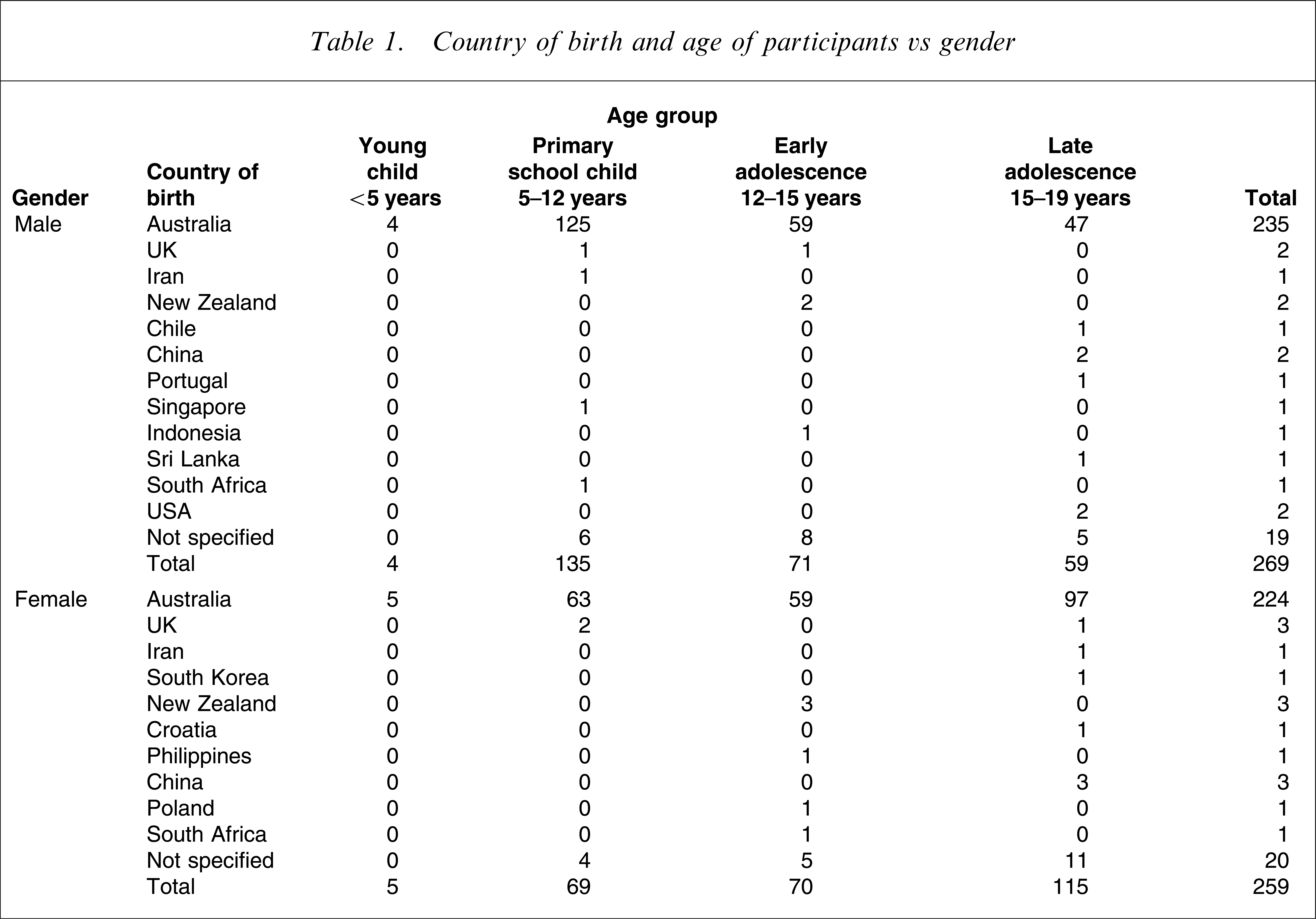
Following approval from the Deakin University Human Research Ethics Committee and the regional Health Service Research Ethics Committee, medical files of all children referred to the service over a 12 month period were examined approximately 1½–2½ years following intake. Files relating to 264 male and 256 female patients who had completed treatment or were no longer in treatment because they had ceased to attend were available for the study. Excluded from the study were 55 patients still receiving treatment and whose dropout/completion status was not yet established, eight patients for whom the diagnosis was missing, and five patients who had experienced two episodes of care in the relevant period. The average age at time of first appointment for the 520 patients (264 male, 256 female) included in the study was 12.6 years (range = 2.5–18.8 years). The majority of the patients were born in Australia and spoke English (Table 1). The Australian-born participants included five indigenous Australians (four male, one female).
Country of birth and age of participants vs gender
The medical records served as the source for each of the variables; data were obtained from intake information forms, reports, formal testing, clinical notes, and correspondence.
Intake information included referral source, intake status (e.g. normal, urgent or crisis) and time on waiting list. Parent information included data on mother's age, father's age, parent education (primary, secondary, tertiary) and the presence of parental psychopathology. Family information included postcode, country of birth, language, number of family members in total, number of family members in home, number of siblings in total, number of siblings in home, parents in the home (single mother, mother and stepfather etc.) and the presence of sibling psychopathology. Child information included gender, age at first appointment, birth order (first, second etc.), birth position (oldest, middle, youngest, only child), education dysfunction, intellectual dysfunction and language problems (these were recorded as either formally tested or noted in the report or file).
Details of previous treatment were recorded for each patient, including provider of previous treatment (paediatrician, general practitioner, school counsellor etc.), number of previous episodes and history of failed attendance at CAMHS (judged as repeated failed attendance in current or previous episodes). Treatment information collected for each patient included treatment team, where the patient was seen, case managers, case managers’ discipline and gender, use of medication, treatment modality (individual, group, both), type of treatment provided, number of sessions, length of treatment, set number of sessions (if specified in treatment plan), completion of set treatment programme.
Diagnoses as determined by clinical assessment were recorded according to the ICD-10 [8], as was the approximate duration of symptoms.
Dropout status was determined through examination of the discharge reports and clinical notes. Cases were coded as completed, dropped out, therapist cessation or referred on. Dropout was defined as the patient terminating treatment through explicitly stating their desire to discontinue, or implicitly by failing to attend sessions even when followed up. Completion of treatment was defined as mutually agreed discontinuation of treatment. Therapist cessation was defined as the therapist unilaterally terminating treatment.
Results
One hundred and sixty-three different diagnoses were recorded in the files of the 520 patients under review, almost half (255 of the 520) of whom dropped out of treatment. These diagnoses were incorporated into 25 super diagnostic categories based on the broad ICD-10 coding system, so that each patient could be assigned a primary diagnosis (Table 2).
System used to create a primary diagnosis from diagnostic groups
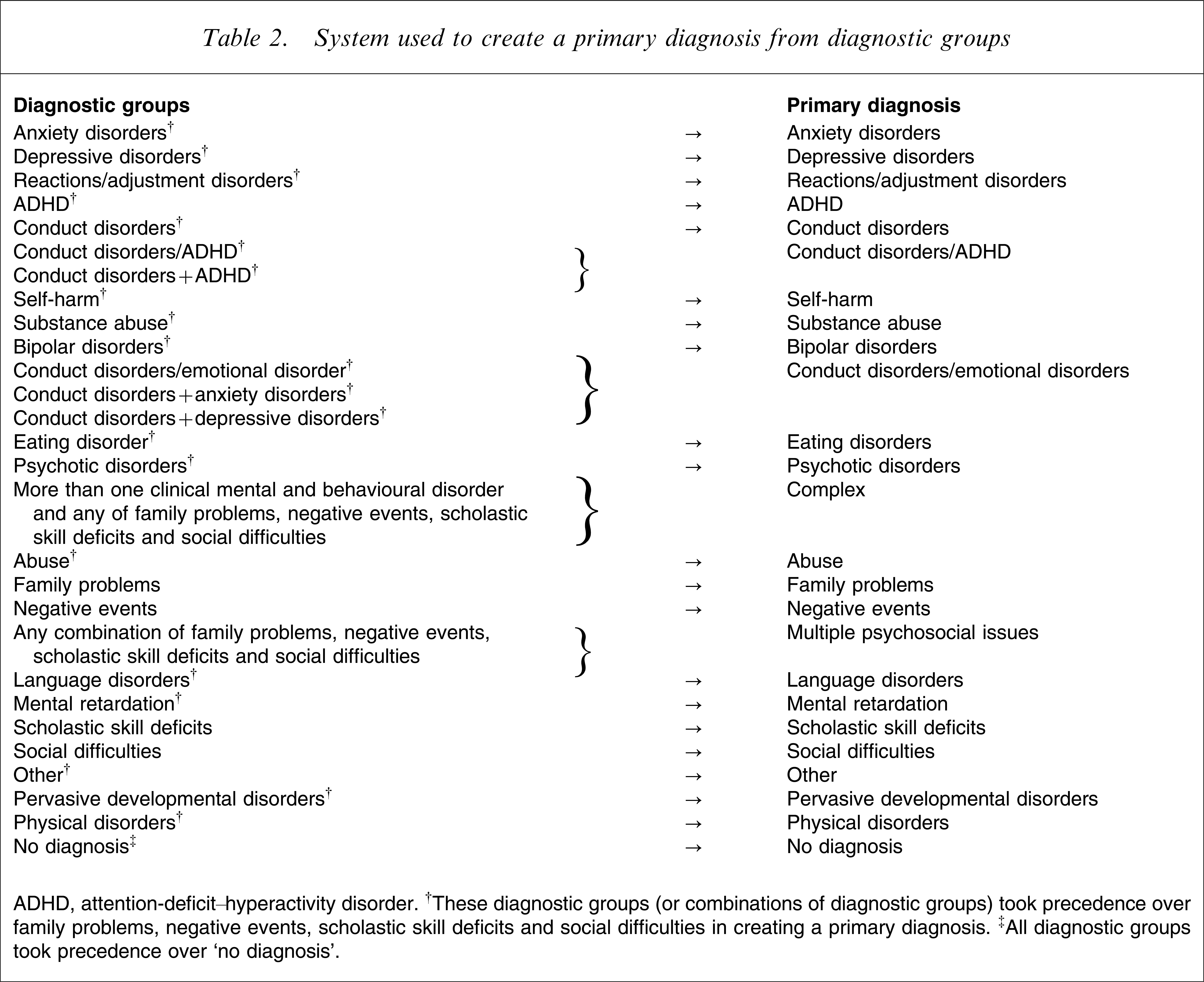
ADHD, attention-deficit–hyperactivity disorder. †These diagnostic groups (or combinations of diagnostic groups) took precedence over family problems, negative events, scholastic skill deficits and social difficulties in creating a primary diagnosis. ‡All diagnostic groups took precedence over ‘no diagnosis’.
Because many patients had multiple diagnoses, the following rules were used to establish a primary diagnosis.
If the diagnoses were conduct disorders and ADHD, the primary diagnosis became conduct disorders/ADHD. If the diagnoses were conduct disorders and anxiety or depressive disorders, the primary diagnosis became conduct disorders/emotional disorders. (These comorbid categories were retained because there was sufficient frequency of comorbidity between conduct disorder and the other disorders to warrant such differentiation.) The mental and behavioural disorders (ICD-10 F codes) were given precedence over non-clinical difficulties such as family problems, negative events, scholastic skill deficits and social difficulties, such that in general, F block codes, which are used to categorize mental and behavioural disorders, were given precedence over Z block codes, which are used to categorize factors influencing health status and contact with health services (such as problems related to negative life events in childhood). Patients with multiple mental and behavioural disorders, and non-clinical difficulties were given the primary diagnosis of complex because they could not be simply allocated into another primary diagnostic category. Patients with only multiple different non-clinical difficulties were given the primary diagnosis of multiple psychosocial issues.
Because insufficient data were available for multinominal or binominal logistic regression to be validly applied, the relationships between parent, family, child and treatment factors and dropout were explored using χ2 tests for relatedness within each primary diagnosis for which data on >20 patients were available. Table 3 summarizes these analyses and shows the factors significantly related to dropout for each diagnosis.
Factors with a significant relationship to dropout for primary diagnosis†
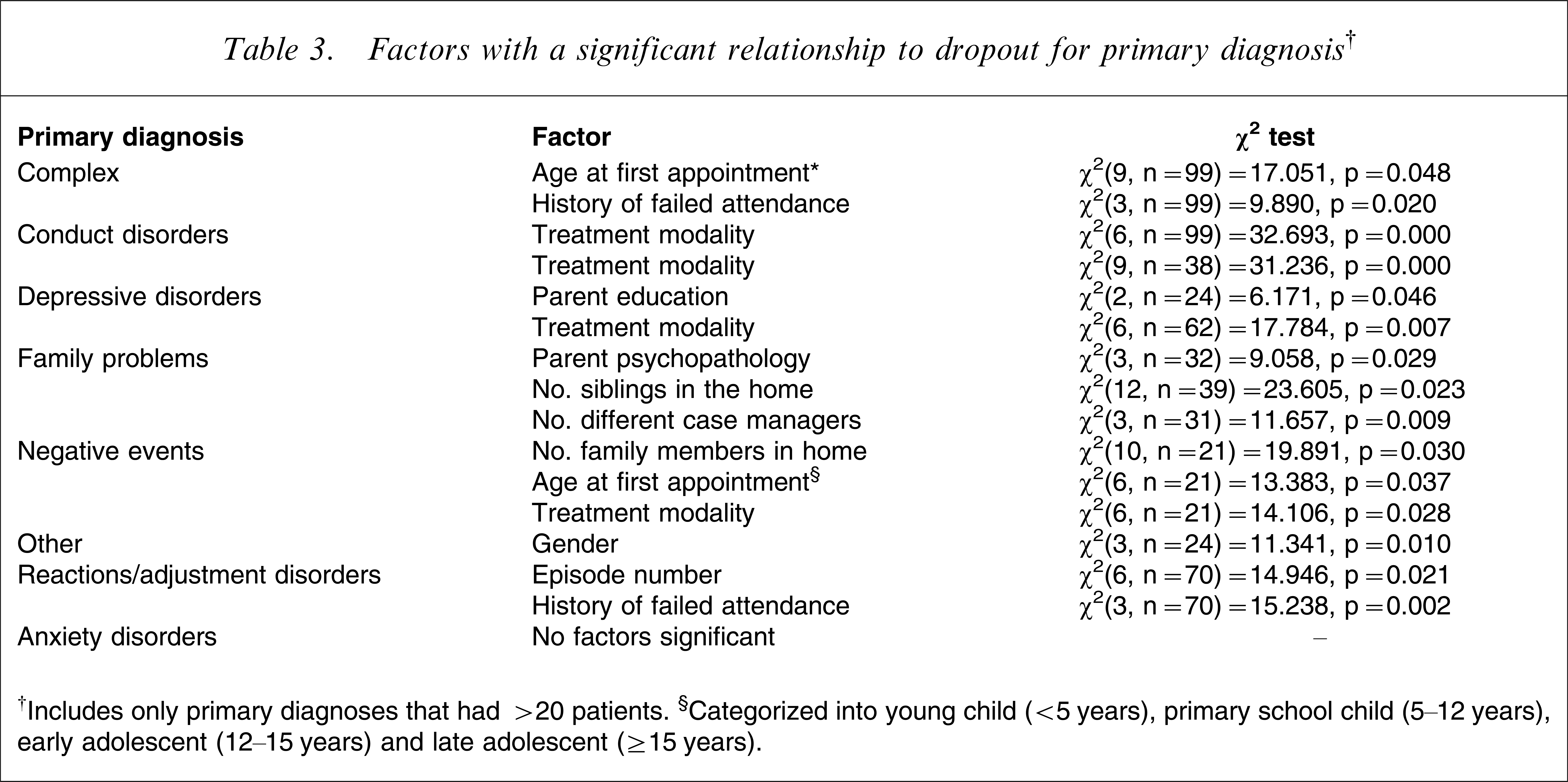
†Includes only primary diagnoses that had >20 patients. §Categorized into young child (<5 years), primary school child (5–12 years), early adolescent (12–15 years) and late adolescent (≥15 years).
As can be seen in Table 3, patients with conduct disorder participating in both individual and group treatment were more likely to complete treatment than those participating in only individual or group treatment. For depressive disorders, children with parents with a secondary level of education were more likely to dropout, and those with a tertiary level education were more likely to complete treatment. The patients receiving individual therapy were more likely to complete treatment than those who had group treatment. For complex cases, older patients and those with a history of missed appointments were more likely to drop out.
Table 3 also shows that family problems patients with an absence of parental psychopathology were more likely to complete treatment than patients in cases involving parental psychopathology. Higher numbers of siblings at home and higher number of case managers were also were associated with dropout. Similarly, for children who were receiving treatment after experiencing negative life events, the number of family members in the home, and age at which the negative event was experienced, were related to dropout, with higher number of family members and lower age of experiencing negative events being predictive. Individual therapy was also related to dropout.
For the ‘other’ diagnoses category, male patients were more likely than female patients to drop out. With regard to reactions/adjustment disorders, the first episode of care was related to completion, whereas having had previous presentations were associated with dropout. A history of failed attendance was also related to dropout.
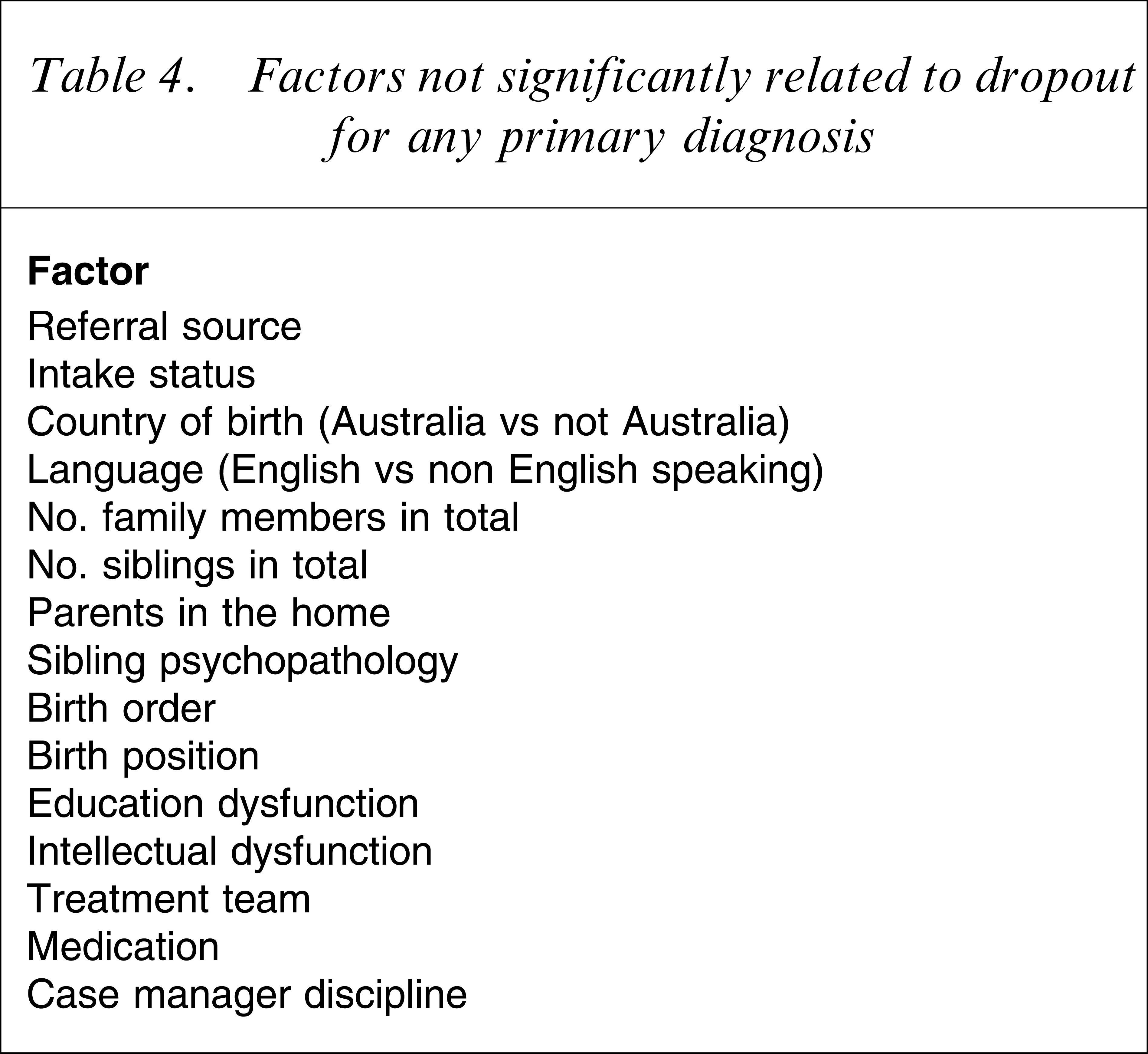
In summary there appear to be some factors that were related to dropout, but some were a result of small sample sizes within diagnoses and a number of factors were unrelated to dropout for all primary diagnoses. These are shown in Table 4. Overall, this suggests that there is a relationship between parent, family, child and treatment factors and dropout for different diagnoses. A clear pattern of factors, however, was not determined.
Factors not significantly related to dropout for any primary diagnosis
Discussion
The current study set out to determine which factors may be associated with dropout for the range of disorders referred to child and adolescent mental health services. Analyses demonstrated that there appear to be some factors that were related to dropout for particular diagnoses, that no factor was associated with dropout across all diagnoses, and many factors were not associated with dropout for any diagnosis.
In complex cases (those involving multiple psychological and behavioural disorders and non-clinical difficulties), age and a history of failed attendance was associated with dropout. For these cases, the finding that older patients tend to drop out is consistent with many studies examining all diagnoses [5, 9–12]. Age, however, has not been associated with dropout in many other studies [13–23]. Thus it may be that the previous findings regarding age have been confounded by diagnosis, such that studies with many complex cases in the sample find an association while those with few complex cases do not.
The finding that among complex cases a history of failed attendance was associated with dropout is perhaps unsurprising, because the reasons for failing to attend treatment would be similar to those that result in dropout. Interestingly, however, this factor was not associated with dropout for children with other diagnoses, even conduct disorder. It may be that the multiple psychological and behavioural disorders and other non-clinical difficulties experienced by children in this category make regular attendance difficult, and that this leads to dropout.
For patients with conduct disorder, those participating in only individual or group treatment were more likely to drop out than those participating in both. It is notable, however, that factors associated with dropout among conduct disordered patients identified in previous research [5, 6] were not found to be associated with dropout in the present study. Such factors include single parenthood, minority group membership, low socioeconomic status, low levels of family cohesion, and parental psychopathology. These findings may be specific to the service in which the file review was performed. This service operates empirically driven parent and child group treatment programmes for patients with conduct and oppositional disorders. The service also has an adolescent day programme that offers intensive treatment in a group setting. In both situations patients often continue with individual sessions. The findings suggest that these combined programmes may be beneficial in retaining these patients, and this may be an indicator for service delivery models in other settings.
For patients with family problems, a lack of parental psychopathology was associated with treatment completion. The absence of parental psychopathology may be an indication of lower levels of, or less severe stress in, the family, and this may have enabled patients to be more likely to complete treatment. In contrast, when parental psychopathology was a factor in this diagnostic group, the risk of dropping out increased. This was the only grouping for which parental psychopathology was related to dropout, and this information has direct implications for service providers. Primarily, ensuring that affected parents are accessing mental health services may decrease the likelihood that a child or adolescent will drop out of treatment.
The relationship between individual therapy and dropout for patients experiencing negative events may be because the events were seen as being uncontrollable, so treatment would not be beneficial. This may indicate that greater education is needed about the possible benefits of treatment for this subpopulation of child and adolescent mental health patients and their parents.
Within the reactions/adjustment disorders, it is unclear why the first episode of care was related to completion. A history of failed attendance being related to dropout is unsurprising because the reasons that a patient failed to attend treatment would be similar to those that result in dropout. It is difficult, however, to speculate on the exact nature of these reasons.
Patients with depressive disorders whose parents had a secondary level of education were more likely to drop out than those whose parents had a tertiary level education. Perhaps tertiary education is associated with greater awareness of, and expectations in relation to, treatment. It may be that public education campaigns about depression, such as the work of beyondblue as part of the National Depression Initiative in Australia has a greater impact among higher educated people than others. If this were the case then there are implications for health promotion campaigns, such as those of beyondblue.
It is difficult to interpret the relationships between previous treatment, gender and number of episodes for the ‘other’ group because this was a mixture of diagnoses. The type of previous treatment, however, has been associated with dropout and completion in the past [11].
Finally, it is interesting to examine the variables for which no relationship was found to dropout for any diagnosis. A number of these variables have been found to be related to dropout in the past. For example, the marital status of parents was not related to dropout, which is surprising because single parent status has been found to be associated with dropping out in a number of studies [6, 18]. Similarly, many studies have found a relationship between minority status and dropout [2, 5, 6, 9, 18, 24]. Such a relationship was not found in the present study. Previous studies, however, were not performed in Australia and the information about ethnic identity was not able to be obtained from the files (only country of birth and language, and very few patients were not Australian or English speaking). A relationship between education and intellectual dysfunction and dropout has been found previously [18] but it is unclear why this was not found in the present study. As in previous studies, however, the discipline of the therapist was found to be unrelated to dropout [21].
Overall, although the present findings provide some pointers for service providers, they need to be considered as preliminary and interpreted within the limitations of this study. There has been much discussion about what constitutes dropout and, even using the criteria described earlier, true dropout status can be ambiguous in some cases: for example when a child does not attend the last appointment at which discharge would have occurred. Further, in our analyses, 163 diagnoses were collapsed into 25 super categories, and then we analysed categories only into which ≥20 participants were allocated. While this was a necessary step in reducing the data for the purposes of analyses and ensuring sufficient cell sizes, the process may have masked more specific associations between particular diagnoses and factors associated with dropout. For example, it is somewhat surprising that single parenthood was not associated with dropout, even for conduct disorder. This may have been due to the small subsamples, or to an underrepresentation of this parental status in the sample overall.
Finally, although it is useful to identify the various factors associated with dropout for particular disorders or diagnostic groupings, this does not explain the underlying process of how these factors result in dropout or the best strategy to prevent dropout. Qualitative work with children, adolescents and their families who drop out from services may assist in providing a greater understanding of these mechanisms. Questions that might be addressed, for example, could be which aspects of various treatment modalities encourage attendance and completion of treatment. In addition, an examination of practical factors such as access to transport, parents’ ability to take time off work and so on in combination with disorder-specific factors would enhance our understanding of dropout from treatment. Analyses that showed how all these various factors may operate in combination to result in dropout for different disorders are desirable.
Conclusions
Although some factors have previously been related to dropout from child and adolescent mental health services generally, the present study identified the factors that may be associated with dropout for specific disorders. This is an important finding in the area of dropout research, and may assist clinicians and services in the development of targeted strategies prevent dropout. More research is needed, however, so that the impact of dropout can be diminished.