
Abstract
Emotion perception abnormalities have long been suggested to be core features of schizophrenia [1–4]. In recent years, considerable evidence has emerged from a variety of experimental paradigms to support the notion that context processing may be necessary for the acquisition and maintenance of social skills among schizophrenia patients [5]. Accurate emotion perception requires people to consider the target emotion in a given context and to generate a proper response. Various studies have tried to clarify emotion perception in context processing [6, 7], which is helpful for understanding cue utilization in different social contexts in schizophrenia [6].
Most emotion perception studies on schizophrenia have focused on facial expressions [8, 9], based on the notion that facial expressions provide the most salient social information [10]. These studies, however, merely examined emotion identification or recognition through categorized photographs of facial expressions. In a real-life scenario it is more difficult for people to correctly perceive facial expressions during social interaction than in a constrained laboratory environment. Previous preliminary studies of emotion processing in schizophrenia may thus be limited in that they fail to examine the corresponding responses of patients to ambiguous or subtle facial expressions. Other studies of schizophrenia have shown that the ability of schizophrenia patients to recognize the eye expressions resulting from a complex mental state may be reduced [11]. The performance of schizophrenia patients in categorizing ambiguous or subtle facial expressions was further explored in the present study by using a continuum of morphing facial expressions. Morphed images have been applied in cognitive psychological research [12] and schizophrenia research [13–15]. For instance, Kircher et al. used the morphed blending of combinations of one's own face and a relative's face, one's own face and an unknown person's face, and a relative's face and an unknown person's face to investigate the self-recognition ability of schizophrenia patients, and found a specific self-face processing dysfunction in schizophrenia [14]. De Gelder et al. focused on emotion identification in multisensory integration using an emotion continuum between a sad and a happy facial expression, along with a semantically neutral sentence that was pronounced in a happy tone or a sad tone [15]. They found that compared with healthy controls, patients with schizophrenia were less affected by the voice in their processing of emotion categorization perception. But although morphed facial images have been widely used to investigate perception characteristics in schizophrenia, no study has specifically examined the impact of social context upon the emotion categorization perception of schizophrenia patients.
Given the increasing evidence that context plays an important role in the cognitive activities of schizophrenia patients [16] and that their context processing is impaired [17, 18], leaving them unable to integrate social contextual information into real-world situations [18], it is necessary to further examine the impact of social dyadic interaction on emotion perception. Social dyadic interaction can take the form of eye gazing [19] or conversation [20]. Successful communication requires the accurate perception of the emotion of the other individual in the conversation, and can enhance a person's daily social functioning. Previous studies have indicated that emotion categorization representation in a facial expression continuum may be impaired in schizophrenia patients [13]. Whether this impairment is promoted or impeded, however, by the context of the conversation remains unanswered. Recent studies have attempted to study affective prosody perception in schizophrenia [21–23], but it would appear that dynamic auditory and visual emotion cues mimic real-world social cues more accurately [24]. Therefore, in the current study we presented questions both aurally and visually to construct the social context using morphed facial expressions. The purpose of the study was to investigate the response patterns of patients with schizophrenia to a continuum of facial expressions in different social contexts.
There is considerable evidence that social threat is a significant factor in schizophrenia [25]. Studies using visual scanpath techniques have provided evidence for early increased sensitivity to and later avoidance of threat-related facial expressions (anger, fear) in delusion-prone individuals [26] and deluded schizophrenia patients [27]. Emotion categorization perception of a morphed facial expression also provides a paradigm to replicate the characteristic perception of angry facial expressions by schizophrenia patients and to further investigate whether their emotion perception is affected by the social context of conversation. Morphed facial expressions in emotion continua should range from pleasant to unpleasant to represent the basic emotion dimensions. Therefore, we morphed facial expressions that ranged from happy to angry to create different social conversation contexts. We asked schizophrenia inpatients and healthy controls to complete an emotion continuum task in a dyadic conversation scenario to elucidate two issues. First, we sought to determine whether different social contexts influence individuals’ categorical perception of facial expressions. Second, we wanted to test whether schizophrenia patients would demonstrate different emotion categorization perception in conversations in different social contexts.
Method
Participants
Eighteen right-handed inpatients with a DSM-IV diagnosis of schizophrenia were recruited from Fangcun Hospital in Guangzhou, China. Two experienced psychiatrists established the diagnosis after an independent assessment. All of the inpatients were undergoing stabilizing antipsychotic treatment at the time of the study. Psychopathological assessment was based on the Positive and Negative Syndrome Scale (PANSS) [28]. Sixteen healthy controls were also recruited from the community through advertisement, and were screened by the first author using a semi-structured interview to confirm the absence of psychiatric history or related illness. Table 1 describes the demographic and clinical characteristics of the sample.
Subject characteristics
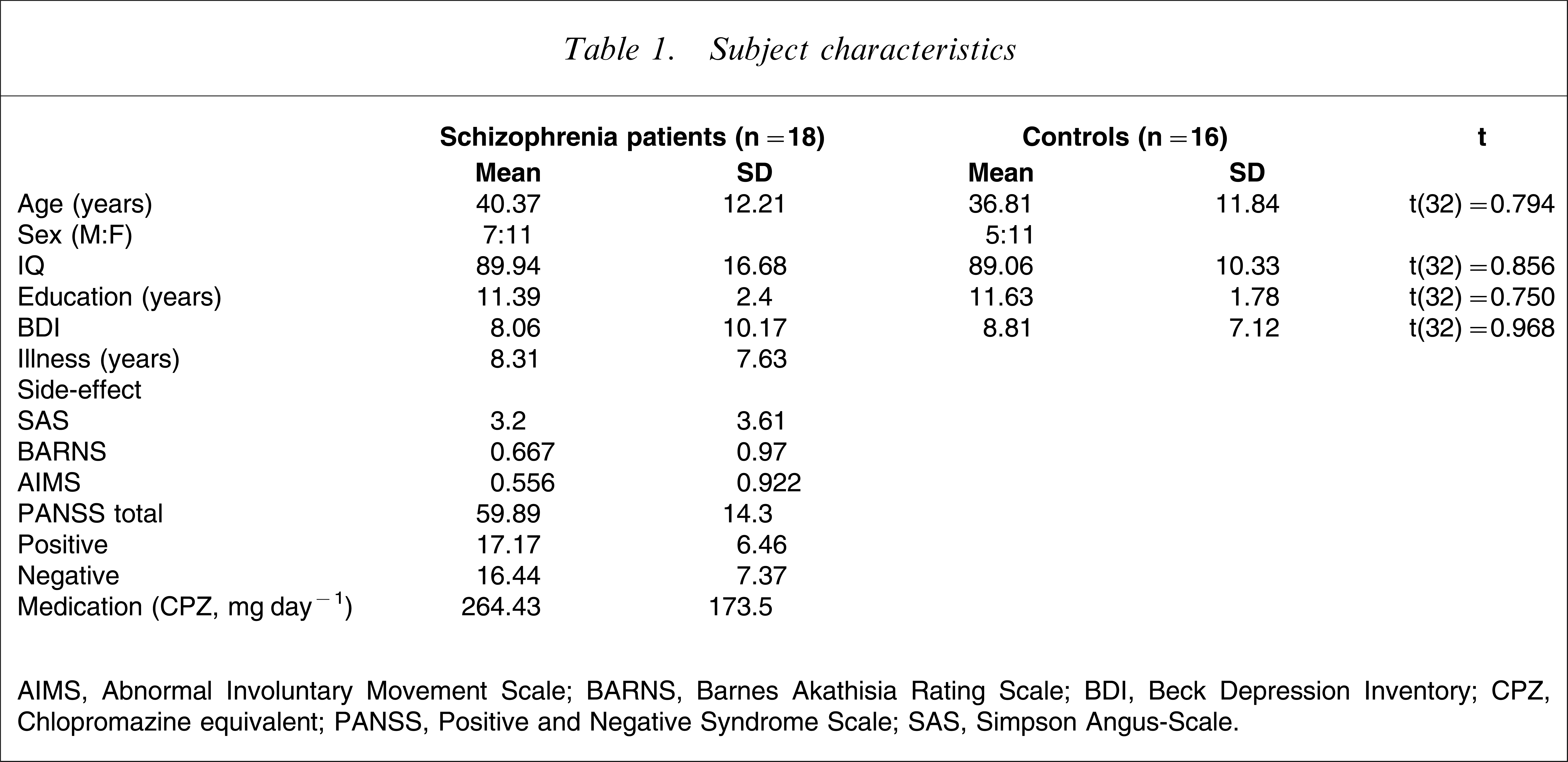
AIMS, Abnormal Involuntary Movement Scale; BARNS, Barnes Akathisia Rating Scale; BDI, Beck Depression Inventory; CPZ, Chlopromazine equivalent; PANSS, Positive and Negative Syndrome Scale; SAS, Simpson Angus-Scale.
Materials
Question development
The source for the questions used in the study was the database of the Centre for Chinese Linguistics of Peking University, which consists of sentences from newspapers, books, magazines, and the media. A total of 61 questions capturing the emotions of negative blame, positive praise, and neutral enquiry were composed according to search results from the database. These questions were then randomly presented to 20 undergraduate students from the Beijing Forest University who were asked to rate their emotion valence and intensity on a 5 point rating scale that ranged from the angry blame (1) and neutral enquiry (3) to the happy praise (5) dimensions. The 12 questions that received the highest agreement for the blame, praise, and enquiry conditions were retained for the main study.
Morphed emotion stimuli
The facial emotion images were created from a set of black and white photographs of Asian people developed by Ekman and Friesen that depict differing expressions, including happy and angry [29]. Using a computer algorithm, the prototype photographs were morphed to create a linear continuum of nine facial images between two end-points (100% angry and 100% happy). Each intermediate image was transformed by a 10% increment (Figure 1). Details of the morphing technique are provided in Pollak and Kistler [30].

Facial expressions ranging from 100% happy to 100% angry. The expressions located in the middle are ambiguous expressions with morphed features of happy (50%) and angry (50%).
Experimental paradigm
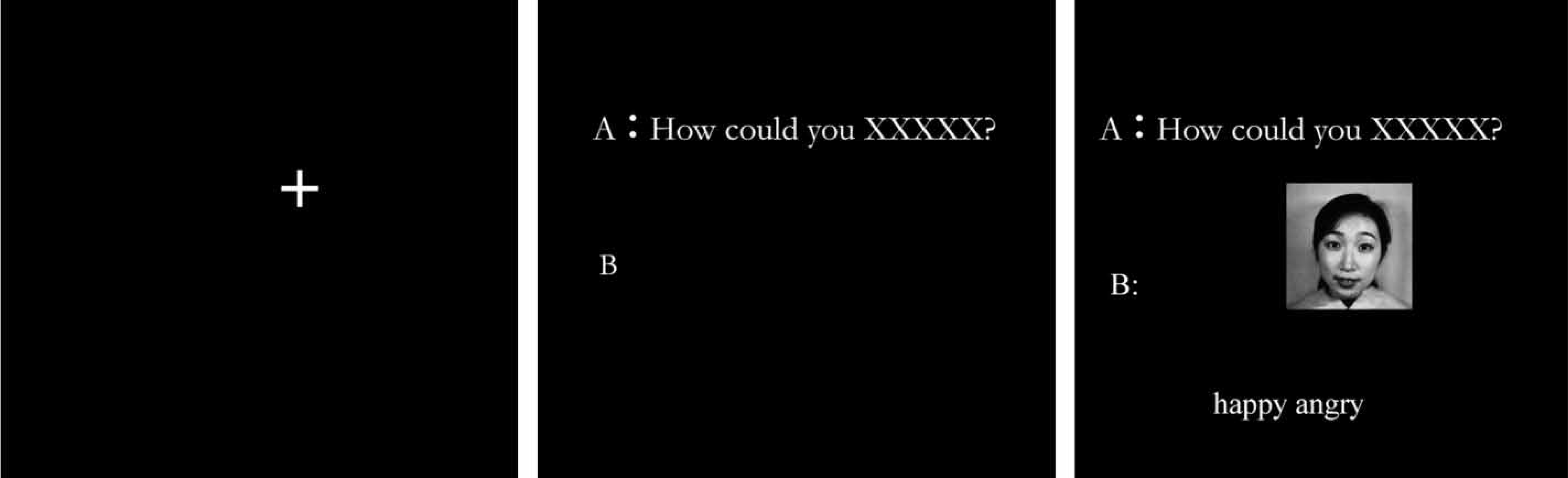
Figure 2 illustrates the flow of the experiment. The subjects were presented with a fixed image at the centre of the screen for a random duration of either 1000 ms or 2000 ms. They were then asked to respond to the dyadic conversation between two persons (questioner A and replier B). The question posted by questioner A was presented at the top of the fixed image with the centre point 157 pixels away from the fixed image for a duration of 2 s. After the visual presentation of the question, the 11 facial expression images of replier B appeared at the centre of the screen in a random order. At the same time, two labels of emotion, ‘happy’ and ‘angry’, appeared below the facial expression. The subjects were instructed to pay attention both to the content of the question being asked by questioner A and the facial expression of the replier B in each conversation. The subjects were asked to select one emotion that best described the facial expression by pressing the corresponding button on a computer keyboard.
The task included four experimental conditions: blame, enquiry, control mask, and praise, distinguished by different categories of questions.
Sixteen questions were asked, each of which was presented with a continuum of 11 morphed facial expressions. One hundred and seventy-six trials were run, with each trial being divided into four blocks of 44 trials separated by a rest period. Four categories of questions were manipulated randomly: blame (How could you be so rude?), control mask (How could you XXX), enquiry (What do you call this man?), and praise (How did you do so well?). Each category contained four questions that had first been evaluated to ensure their equal emotion intensity. Each question was spoken and recorded in four tones: an angry tone for the blame category, a neutral tone for the control mask and enquiry categories, and a happy tone for the praise category. Each question was presented in both visual and auditory modules. The control mask question, ‘How could you XXX,’ was simply said ‘How could you…’ with no emphasis on the XXX part. The enquiry (neutral) questions were complete question sentences pronounced in a neutral tone. The control mask questions were designed to be compared with the enquiry (neutral) questions to exclude the influence of semantics on the subjects’ performance. Each block contained four questions in different categories, each with 11 morphed facial expressions. Before the actual experiment, four practice trials were run, each using only one question type.
Data analysis
Both linear and logistic curves fit the data well, as shown in Table 2, which compares the two functions with an ΔR2 t distribution, but because previous studies that have adopted the emotion identification paradigm have suggested that the logistic function is theoretically more appropriate for this task and is much less sensitive to outlying data points and the trajectories of individual subjects [30], we adopted this emotion continuum data analysis procedure, as described by Kee et al. [13]. We estimated the logistic parameters by parsimoniously characterizing the emotion identification task performance with the same logistic function model as in [13], as follows.

where y is the probability of identification, x is the signal strength, a is the lower asymptote, b is the difference between the upper and lower asymptotes, c is the signal threshold at the midpoint, d is the slope, and e is the exponential function. The shift point, or signal threshold at midpoint (c), and the slope (d) were the two parameters that we estimated to characterize emotion perception performance in the data analysis, according to the definitions in Kee et al. [13]. The signal strength increased steadily from the angry face with each morphed facial expression. We regarded the signal strength of the happy facial expression as 1 and that of the angry facial expression as 11, with the signal strength of the other morphed facial expression between these two ends taking the integer values between 1 and 11. The shift point is the point on the signal strength continuum most likely to be identified as the point at which the emotion shifted from happy to angry, and the slope indicates how abruptly this change occurred. A high value for the slope indicates a clear and relatively abrupt shift from classifying the photos as happy to classifying them as angry, with a flatter slope indicating more ambiguity in the shift from one emotion pole to the other, that is, from happy to angry.
Fitness of linear and logistic functions
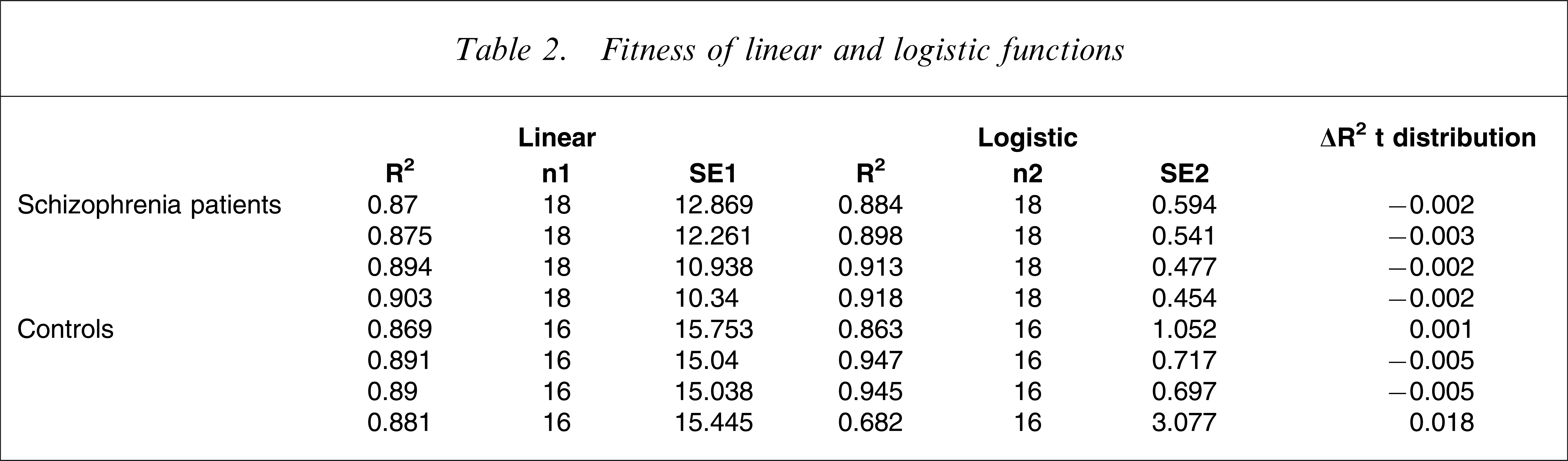
We used the asymptotic method to generate the standard error of the two parameters based on the 11 data points of signal strength for each question category. The asymptotic method generates the same mean slope and signal threshold as the bootstrapping method, but with a usually larger standard deviation.
Results
Performance of the two groups in the emotion identification task in the four conversation conditions
There was a significant difference between the two groups (inpatients and controls) in the proportion of angry identifications for the blame question category (χ2(1) = 6.443, p = 0.011) and for the control mask (χ2(1) = 4.44, p = 0.035), but not for the enquiry question (χ2(1) = 0.62, p = 0.431) or the praise question (χ2(1) = 0.309, p = 0.579; Figure 3). In the blame question context, the subjects with schizophrenia categorized 36.1% of the ambiguous facial expressions as angry when the signal strength was 6, whereas the healthy controls categorized 60.9% as angry. Similarly, in the control mask context, the subjects with schizophrenia categorized 34.7% of the facial expressions as angry, whereas the healthy controls categorized 54.7% as such.
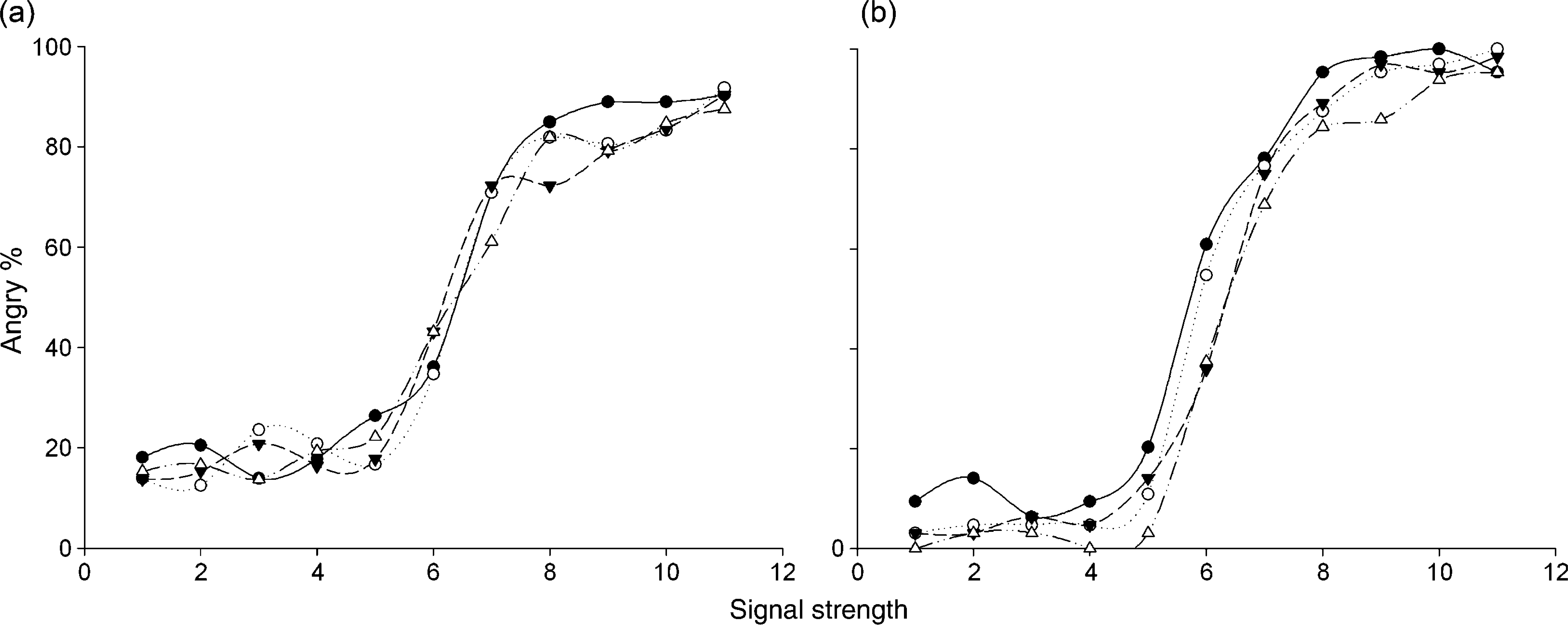
Emotion identification task performance in (a) patients with schizophrenia and (b) healthy controls across the four conditions. When the signal strength was 6 (an ambiguous facial expression), there was no difference among the four question categories in the percentage of angry identifications (χ2(3) = 1.146, p = 0.695). There was a significant difference among the four question categories in the healthy control group (χ2(3) = 9.705, p = 0.021). (–•–) Blame; (
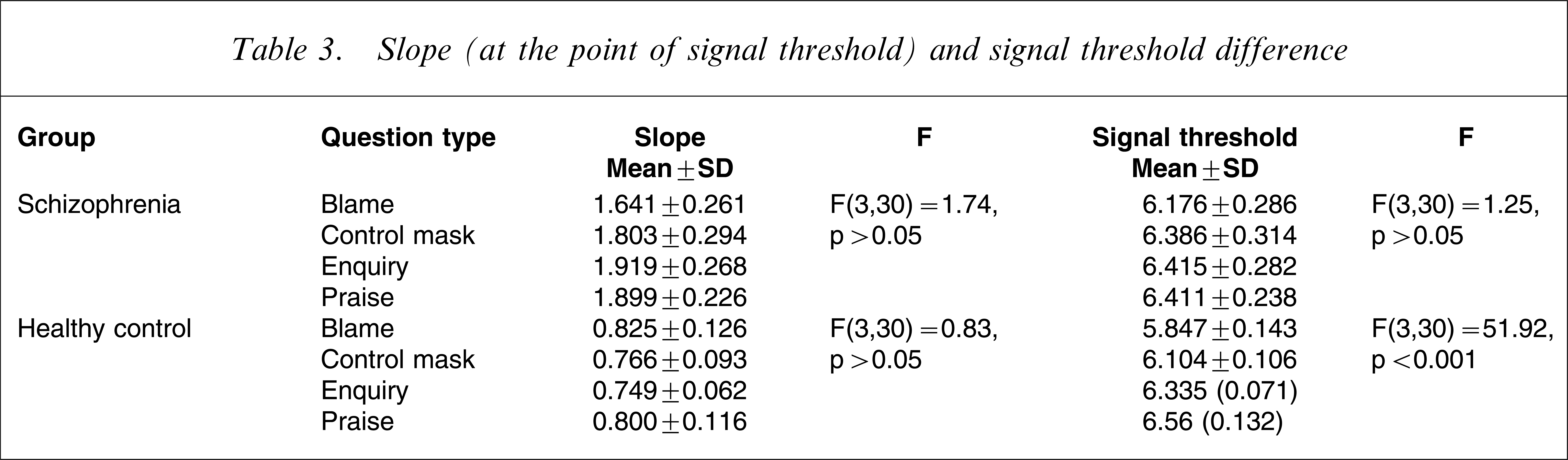
To evaluate whether the conversation atmosphere influenced individuals’ emotion perception categorization, a series of independent ANOVAs was conducted on the shift points and slopes on the happy–angry continua of the two groups. The descriptive data and results of these statistical tests are presented in Table 3. There were significant differences among the healthy controls in the mean signal threshold but not the slope for the four question categories. There were no significant effects, however, among the patients with schizophrenia in the mean slope or signal threshold for the four question categories.
Slope (at the point of signal threshold) and signal threshold difference
Group differences in slope and signal threshold for the four question categories
To evaluate whether there was any difference between the patients with schizophrenia and the healthy controls in terms of when and how rapidly they began to categorize facial expressions as angry, we compared the mean slope and signal threshold of the two groups. Table 4 shows that the patients with schizophrenia demonstrated a steeper turning from the left pole of the happy emotion to the right pole of the angry emotion than the healthy controls, which indicates that the patients with schizophrenia perceived the angry emotion more rapidly than the healthy controls. The two groups, however, did not significantly differ in shift point for any of the question categories, suggesting that the subjects in the two groups began to categorize facial expressions as angry at almost the same time.
Slope (at the point of signal threshold) and mean signal threshold difference
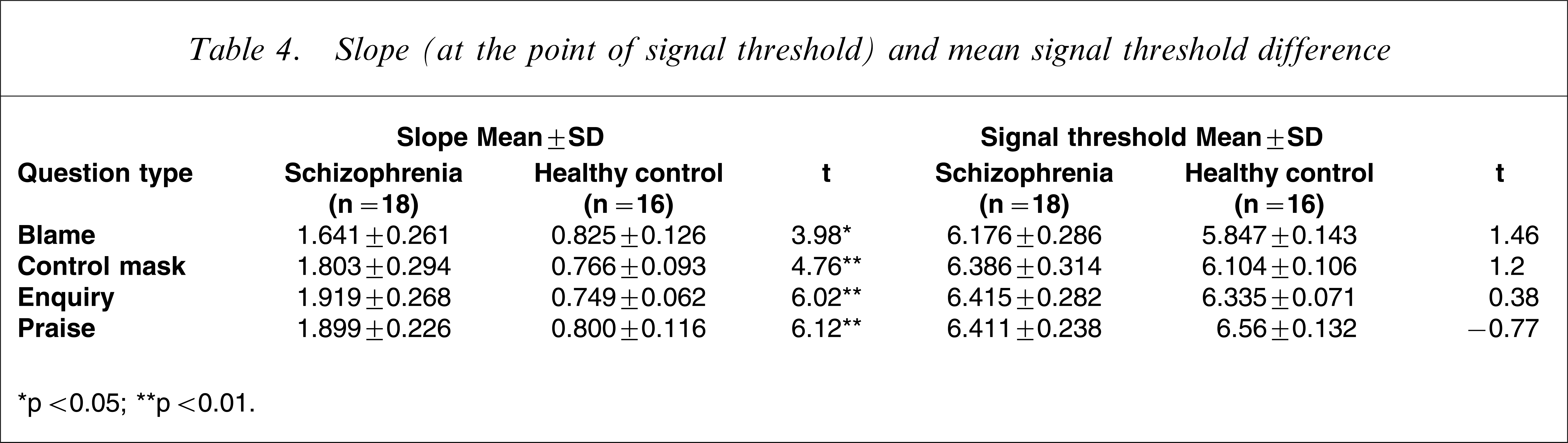
∗p < 0.05; ∗∗p < 0.01.
Supplemental analysis
In light of the steeper slope for the schizophrenia group, we further examined whether it was related to delusion symptoms in schizophrenia. Using a cut-off for the delusion item from PANSS of at least moderate or above, five patients were identified as having delusion and five were identified as being without delusion symptoms. The mean slope for the deluded schizophrenia patients was steeper than that of the non-deluded schizophrenia patients for the blame question category (t(9) = 3.95, p < 0.05) and enquiry question category (t(9) = 3.21, p < 0.05).
Discussion
The findings showed that patients with schizophrenia were less affected by different social contexts in identifying emotion categories in conversations compared with the healthy controls. Moreover, there was a propensity for the inpatients to change more rapidly from the happy emotion pole to the angry emotion pole at the shift point than the healthy controls, regardless of the social context, a result that was particularly manifested in the deluded schizophrenia patients.
The shift point indicates the point on the emotion continuum at which the subjects’ categorization shifted from one pole to the other. The shift point results suggest that the inpatients may have been less adaptive to categorizing emotions in conversations in changing social contexts than the healthy controls. Impairment in social cognition in schizophrenia and its relationship with social function has been extensively examined in previous studies [31, 32]. These studies, however, have not specifically examined the direct influence of the context of social interaction on social cognition. The similar slope and shift points for the four conditions with different social information indicate that patients with schizophrenia may not be able to make appropriate social judgments when the context and content of a conversation changes only slightly. These findings are in accordance with previous studies that have found that patients with schizophrenia may have impaired emotion context processing [17], but extend this impairment to cover interaction context. Taken together, the findings indicate that emotion perception impairment among schizophrenia patients may lead to a deficit in social interaction.
The mean slope of the schizophrenia group was steeper than that of the control group, and supplementary analysis suggested that deluded schizophrenia patients had an even steeper slope than non-deluded schizophrenia patients. This indicates that the patients with schizophrenia, and particularly those with deluded schizophrenia, seemed to be more sensitive to the change in question category from happy to angry compared with the healthy controls. The steeper curve for schizophrenia is inconsistent with the results of previous studies [13, 15]. There are three possible reasons for this. First, we used different methods to analyse the categorization of emotion perception data. In the Kee et al. study the authors used the bootstrapping method to generate the empirical standard deviation [13], but this was considered to be less well suited to our small sample: bootstrapping based on 30 samples in SPSS gives a standard deviation that is so small that the referring statistic is exaggerated. Therefore, we used the more conservative asymptotic method to generate the standard error for the two parameters based on the 11 data points for each question category condition.
Second, previous studies on emotion continua have mainly been based on angry–sad, angry–fearful, fearful–happy, and happy–sad continua, which may not be comparable to the happy–angry continuum in its meaning to schizophrenia. It may also be that schizophrenia patients are less able to discriminate the facial expressions of negative emotions, such as angry and sad. The rapid change, however, from the happy pole to the angry pole at the shift point in the schizophrenia group suggests that these patients were sensitive to social threat information when the anger signal increased. Furthermore, when the facial expression was ambiguous at a signal strength of 6, the schizophrenia patients categorized the emotion as angry significantly less often than the healthy controls. An interpretation is that when the anger signal was ambiguous, they avoided perceiving it as a threatening emotion, whereas when the angry signal increased, they became more vigilant, resulting in a rapid change in the curve.
Third, a supplemental analysis of deluded and non-deluded patients showed that the deluded patients demonstrated a steeper slope at the shift point than the non-deluded patients, which implies that the rapid change from the happy pole to the angry pole is somehow related to the presence of delusion. This finding provides another piece of evidence to support further exploration of the relationship between social cognitive bias and the formation of delusion previously suggested by visual scan-path research [33]. Other preliminary studies have also suggested that deluded or delusion-prone individuals are biased in their processing of social threat information [34]. The steeper slope but similar shift point of emotion categorization performance in the schizophrenia group in the present study further indicates that patients with schizophrenia, and especially those with delusion, make a rapid but not an early acknowledgement of social threat information such as anger [35–37].
The present study provides only preliminary findings on emotion perception based on the social context of conversation. It is limited by the small sample size, in that the function curve is not sufficiently smooth to give a good picture of the parameters. Furthermore, we adopted only the happy–angry emotion continuum, which makes it difficult to infer that the bias found in the current categorization of emotion perception is specific to schizophrenia. Further studies that adopt a more rigorous methodology with a larger sample should be launched to further validate the current findings.
Footnotes
Acknowledgements
This study was supported partially by the Research Initiation Fund of the 100-Scholar Programme (16000-3253182) from the Sun Yat-Sen University, the Research Initiation Fund (O7CX031003) and the Research Fund (KSCX2-YW-R-131) from the Institute of Psychology, Chinese Academy of Sciences, and grants from the National Natural Science Foundation of China (30770723) and National Basic Research Program of China (973 Program) (2007CB512302) to Raymond Chan.