
Abstract
In establishing rapport with any patient, it is the general maxim health that practitioners are caring [1]. We have long had the impression that female and male general practitioners (GPs) differ in the expression of care that they provide to depressed patients. This would not be unique to psychiatry because many previous studies have identified gender effects in GPs, with female GPs facilitating more open exchange with patients than their male counterparts and entering into more active physician–patient partnership behaviours [2, 3], as well as spending more time in consultations and being more likely to treat those with psychological problems [4].
In light of such general findings and our informal observations, we undertook two descriptive studies for which three research questions were formulated: (i) do female GPs write consistently longer referral letters (an ideal referral length to a psychiatrist as previously explicated is around 185 words) [5] than male GPs; (ii) are female GPs more likely to be viewed as more caring, and do they listen more than their male counterparts; and (iii) are male GPs more likely to prescribe or suggest medication as a first-line option for depression and, in turn, less likely to offer or suggest psychological strategies.
Methods
Study 1
The sample consisted of 100 consecutive referrals by GPs to the Black Dog Institute Depression Clinic: a Sydney-based, statewide tertiary service providing diagnostic and management advice for patients referred with a depressive mood disorder. Data included the actual number of words written by the GP in the referral letter, and the gender of the referring GP.
Study 2
A separate survey to the referral data was designed and posted on the Black Dog Institute website (http://www.blackdoginstitute.org.au). Data collection ceased when more than 500 fully completed questionnaires had been received. The questionnaire stated that we sought to learn about the individual's ‘experience of visiting a GP for the first time about depression within the past year’. It was noted that data collected would be anonymous and that we did not seek to identify respondents in any way. Questions (as noted below) directly and indirectly assessed components of care provided by the GP, as well as the gender of both the patient and the GP, while also addressing several management nuances. Our hypothesis – that there would be gender differences identified across the female and male GPs – was neither stated nor able to be inferred by participants. Once 517 complete questionnaires were generated, the survey was removed from the website.
Results
Study 1
The mean number of words used in the referral notes was 220.1 (SD = 207.1) from female, and 87.6 (SD = 81.8) from male GPs, a significant difference (t = 4.20, p < 0.001). On qualitative examination, male referrers were more likely to write brief ‘Please assess and manage’ referrals lacking background information.
Study 2
Of the 517 (167 male, 350 female) respondents, 309 (59.8%) nominated consulting a male and 208 a female GP. Table 1 reports responses to several survey questions. Question 1 (the extent to which the GP was judged to be caring when the patient spoke about depression) had five rating options. In the analysis we deleted the middle neutral option (generated for 20% of the male and 21% of the female GPs), and contrasted the consolidated responses of ‘not at all’ and ‘a bit’ (i.e. ‘uncaring’) with ‘quite a lot’ and ‘very much’ (i.e. ‘caring’).
GP attitude and treatment strategy vs gender
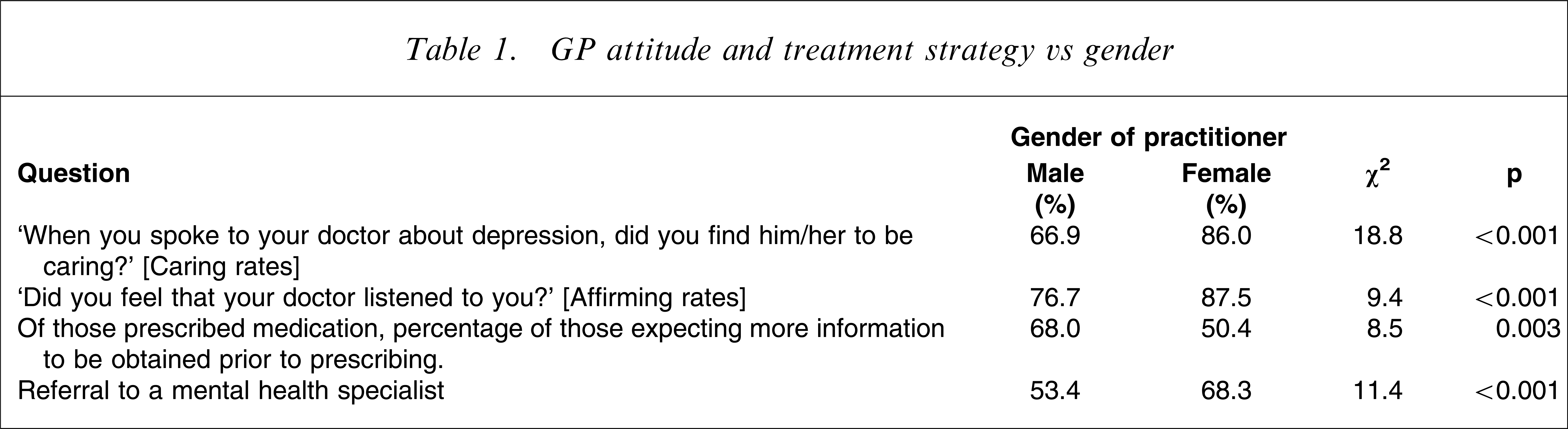
Table 1 data indicate that female GPs were rated as significantly more caring and, in response to the second question (‘yes’ vs ‘no’ answer), as significantly more likely to listen to the patient. A subsidiary analysis indicated that, although male patients returned comparable care levels from both male and female GPs, female patients rated female GPs as more caring than male GPs (χ2=21.61, p < 0.01).
Those scoring their GP as ‘not listening’ (male n = 71, female n = 25) were requested to judge the extent to which the GP expressed that response across one or more of five specific parameters. Although ratings across each parameter did not identify any significant differences, there were consistent GP gender differences, with male GPs more likely than female GPs to show ‘poor eye contact’ (74.1% vs 25.9%), ‘cut off’ the patient (72.7% vs 27.3%), be ‘verbally distant’ (80% vs 20%), to ‘suggest a solution before hearing you out’ (71.7% vs 28.3%) and be viewed as ‘too quick to prescribe medication’ (71.8% vs 28.2%). Additional analyses indicated that the gender of the patient did not influence those findings.
There was a non-significant trend for patients to be more likely to expect a male (61.2%) as against a female (38.8%) GP to prescribe medication. At that initial consultation for depression, two-thirds (66.5%) were actually prescribed medication (48.3% to female patients by female GPs and 20.9% to male patients by female GPs; 51.7% to female patients by male GPs and 79.1% to male patients by male GPs). Although there was a trend for prescriptions by male GPs to be higher, the overall gender of patient–GP analysis was not formally significant.
When asked if they had expected more diagnostic information to have been sought by the GP before prescribing any medication, 26% of the respondents answered ‘don't know’, while Table 1 data show that, of those who had such expectations, this was more likely in relation to a male GP. No impact of patient gender was observed in relation to such expectations.
Table 1 data also indicate that female GPs were more likely to refer patients of either gender to a mental health professional specialist (i.e. psychiatrist, psychologist), whereas male GPs were more likely to refer male rather than female patients (62.2% vs 37.8%, χ2=10.7, p < 0.01).
For those so referred, we sought to determine whether such specialist referral might merely reflect the GP seeking to avoid direct management, and asked two explicit questions. First, ‘Did your general GP just want to refer the problem to someone else?’. Of the 52 patients who affirmed the question, more had consulted a male than a female GP (75.0% vs 25.0%, χ2=12.0, p = 0.001). Both male (χ2=8.2, p < 0.01) and female (χ2=5.5, p < 0.05) patients nominated male GPs as more likely than female GPs to want to ‘refer the problem to someone else’. The second question: ‘Did you feel that your general practitioner referred you for ‘good’ or ‘bad’ reasons?’, generated only 19 patients nominating ‘bad’ reasons, and no difference emerging from GP or patient gender was identified.
Asked if they would return to the same GP for further depression management, rates of returning to a male GP were slightly lower than those for female GPs (72.5% vs 80.3%, χ2=4.1, p < 0.05). Gender-of-patient effects were demonstrated only for female patients, who were significantly less likely to return to their male GP (64.8% vs 35.2%, χ2=8.5, p < 0.05).
We next examined GP-recommended medication and/or counselling approaches. After deleting 43 patients (whose GP had not nominated any treatment), the rates of prescribing medication alone was 15% (70/474 GPs), with male GPs more likely to prescribe a drug as a monotherapy (20.2% vs 7.1%, χ2=15.7, p < 0.001). By contrast, of the 11% nominating counselling only, there was no GP gender difference (56% male, 44% female GPs). Combination management strategies (e.g. medication and counselling) were nominated by the majority of GPs and without any gender differences being identified.
For those patients whose GPs had prescribed a treatment, we examined whether having medication prescribed as the only treatment influenced the decision to return to see that GP, and established that a return visit was less likely to occur in such circumstances if the GP was male (20.0% vs 80.0%, χ2=6.2, p < 0.025).
We allowed survey respondents to provide open-ended information about the characteristics of medical consultations that would influence their decision to return for future assessment and management of their condition. Responses weighted the doctor being empathic, able to listen, experienced and not merely there to prescribe medication.
Finally, open-ended information was sought on what features distinguish a caring GP. Responses again weighted interpersonal issues such as listening, empathy and understanding, being non-judgmental, and two competence components (asking questions and ability).
Discussion
Because the survey (Study 2) was Web-based and limited to patients’ subjective experiences, we cannot draw any general conclusions about the extent to which patients had clinical depressive conditions (and their severity), and we cannot make any judgments about the extent to which GPs’ interpersonal and management styles are representative of GPs in general. But because our principal objective was to examine for gender differences among GPs in managing a new episode of depression, the overall representativeness of surveyed subjects is less of concern. It is also important to emphasize that we structured the survey in neutral terms (i.e. neither suggesting that we sought to identify strengths or limitations to GP management), and that we did not allude to our hypothesis (of gender differences). Thus, even if there were negative or positive response biases by subjects, we would again argue that these would be unlikely to have influenced our gender findings.
Survey findings can be briefly summarized. In managing depression, male (compared to female) GPs were less likely to be rated as caring and listening, showed poorer communication skills and, as expected by the respondents, were more likely to prescribe medication, more likely to prescribe medication alone, more likely to seek less information than expected by the patient, and less likely to refer to a specialist (but more likely to be viewed as wanting to refer on and not manage the patient).
The gender of the patient had some impact. Female patients were more likely to rate female rather than male GPs as caring, and less likely to receive medication from GPs of either gender.
If these findings are valid, such gender differences could reflect differing processes. It could be a ‘men from Mars, women from Venus’ scenario, in which the female doctors wish to spend more time in discussion versus male GPs ‘cutting to the chase’ and making rapid technical decisions, and the female GPs viewed as more caring in consequence. It would be of benefit to have information on the length of time of the average consultation, although Australian data (of some 70 000 consultations) have shown that female GPs do spend more time with patients generally [6]. It could also be that depressed patients (and especially women) expect more care from female GPs and that their expectations then influence the practice interaction [7].
Such findings could also reflect a gender difference in levels of conscientiousness and/or perhaps even defensive practice (i.e. the GP seeking to avoid a poor outcome), as supported by female GPs being more likely to refer their patients on to specialists. But communicated lack of care (e.g. poor eye contact, cutting the patient off, precipitous prescription of medication) – all of which appear to reflect an actual lack of care and empathy – were more likely to be effected by male GPs.
There are other studies that have identified gender differences in GP interpersonal skills and practice priorities that, while not being limited to the management of mood disorders, support our findings. For example, a Canadian study of GPs identified that female GPs were more likely to value psychosocial factors in patient care [8]. In an Australian study of 113 000 general practice encounters, female GPs were more likely to manage psychosocial problems [9]. In a Californian study the gender of the GP was shown to influence the communication pattern and to contribute to the female GPs being viewed as providing greater patient satisfaction [10].
The impact of any such differential level of care is clearly not trivial when open-ended survey responses identified empathy, care and listening as the priorities from a GP. Further, female patients were slightly less likely to return to a male GP – and particularly less likely if the GP favoured medication as the only option. Thus, the patients seem not only to have experienced less care from male GPs, but also that the differential level of care had real-world impact in influencing how they would seek to have their condition managed in the future.
We established that male GPs were more likely to refer-on the depressed patient. Such a finding may link with results from Study 1, in which male GPs wrote less detailed (and qualitatively more superficial) referral notes to our specialist clinic. This is a striking finding that may reflect differential care writ large. It is worthy of further study.
Thus, in managing a patient with a new episode of depression, female GPs were rated as more caring and empathic than male GPs. If female GPs are more caring in such circumstances and also write more detailed referral notes, does this impact positively (or even negatively) on the management of those with mood disorders? If a doctor is efficient and implements the correct management strategy, then the doctor's interpersonal characteristics are of little consequence at a utilitarian level. It would be a rare individual, however (and particularly one who has psychological problems), who would not wish to have a GP who is not only technically efficient but who shows interest and empathy, and who listens to their story. Our open-ended questions, which enquired into GP factors that would encourage the patient to return, found strong support for both technical competence (i.e. experience) and also for the expression of care that not only included empathy and listening, but the doctor going beyond the mere prescription of medication. Pollock and Grime have previously drawn attention to patients with depression feeling under acute time pressure in the usual time allocated for a medical appointment, and consequently feeling unable to fully disclose their problems, preventing them from obtaining best use of consultations [11].
Clinical depression is now recognized as a highly prevalent condition. It has attracted an extraordinary number of studies in recent decades examining the impact of differing treatments. Most such studies focus on specific treatments. Because there has been a move away from the psychotherapies of the past – accused of being redolent with ‘non-specific’ therapeutic ingredients (e.g. empathy, therapeutic congruence, non-possessive warmth) – there has been less consideration of the impact of such variables, despite their widely recognized capacity to activate remission in those with a depressive condition [12]. If the gender of the GP does influence the assessment and management of those with depressive conditions to any substantive degree, quantifying the therapeutic impact of such differences may enable the design of strategies and tools to improve early medical education, with the long-term effect being the more efficient management of conditions that are commonly chronic, difficult and disabling – and in which therapist care is a substantive management component.
Footnotes
Acknowledgements
The authors gratefully acknowledge Kerrie Eyers for assistance and grants from the National Health and Medical Research Council of Australia (510135) NSW Department of Health.