
Abstract
Preventative approaches are important because anxiety disorders, if left untreated, represent a significant cost to individuals and the community [1, 2]. Recent community surveys have confirmed that anxiety and depressive disorders are among the most prevalent disorders across childhood and adolescence [3], and are associated with severe impairment in life and activities [4]. There is a strong case for preventing problems in the first place before they begin to cause disability, restriction of life choices and other damage [5].
The key study in the prevention of childhood anxiety, using an indicated approach, is the Queensland Early Intervention and Prevention of Anxiety Project [6, 7]. Children aged 7–14 years who were screened for symptoms of anxiety either attended a group-based cognitive behavioural programme (Coping koala: prevention manual) run by clinical psychologists in their schools, or were assigned to a monitoring (control) condition. At the 6 month follow up 16% of children in the treatment group met criteria for an anxiety disorder, compared to 54% in the control group. A similar pattern of results was found at the 2 year follow up, with 20% of the children in the treatment group and 39% of children in the control group meeting criteria for an anxiety disorder. The strongest effect was found for children who had an initial anxiety disorder, suggesting a salient treatment, as opposed to preventative, effect. The intervention, however, produced a significant decrease in the risk of maintaining or developing an anxiety disorder.
The aim of the present study was therefore to assess whether a school-based programme already shown to prevent anxiety disorders in children when delivered by clinical psychologists, could produce a similar outcome when conducted within the school by school counsellors and teachers.
In the present study students in their first year of high school identified as ‘at risk’ for developing an anxiety disorder participated in either a school-based intervention or a monitoring (control) condition, and were assessed for the presence of anxiety disorders and symptoms 4 years later.
Method
Participants
A total of 1120 children (482 girls, 43%) were recruited from 19 Catholic secondary schools in the metropolitan area of Sydney, Australia in 2001. All participants provided student and parental written consent and the project was conducted in compliance with the ethics protocols of the hospital and university ethics committees. The sample represented 47.1% of the larger sample (n = 2377) who were initially approached to participate in the research. All students were in grade 7 and aged between 11 and 13 years (M = 12.05 years, SD = 0.40).
Measures
Self-report questionnaires
The Revised Children's Manifest Anxiety Scale (RCMAS) identified those students with higher anxiety symptoms that might put them at risk for the development of future anxiety disorders [8]. The RCMAS was also used as an outcome measure along with the Spence Childhood Anxiety Scale (SCAS) [9] and the Child Depression Inventory (CDI) [10].
Diagnostic interviews
The Schedule for Affective Disorders and Schizophrenia for School-age Children (K-SADS-P/L) is a structured diagnostic interview that assesses other disorders, anxiety and mood disorders in school-age children [11]. This was used as a baseline diagnostic measure. At the 4 year follow up, 12 month DSM-IV diagnoses of anxiety and affective disorders were made using the Composite International Diagnostic Interview (CIDI, version 2.1).
Health-care use
All participants completed a questionnaire at both follow ups that asked them whether they had seen a mental health professional for problems with stress, anxiety or depression over the previous 2 years, and to nominate the type of health professional seen. The CIDI and these questions were taken from the Australian National Survey of Mental Health and Well-Being [1].
Intervention.
The FRIENDS intervention consists of 10 weekly group sessions and two booster sessions (conducted 1 and 3 months following the completion of treatment), as well as parent sessions that match the content of the child sessions. Each group session lasted for 50 min. Schools ran one to two parent sessions. Strategies taught within the programme included learning to be aware of symptoms of anxiety, to relax, to challenge unhelpful thoughts, to use graded exposure to overcome avoidance, and problem solving. The FRIENDS programme has been described in detail elsewhere, and has been found to be an effective treatment for childhood anxiety disorders [12].
Procedure
First-stage screening
The screening procedure described by Dadds et al. [6] was used to identify children at risk for the development of an anxiety disorder using a cut-off score of 11, 1 SD above the average score based on an age-related normative sample [8].
Second-stage sample selection
Teachers were asked to nominate up to three students who displayed prominent anxiety (i.e., shy, nervous, afraid, inhibited) and 24 students were further included in the study. Class teachers were provided with the list of students who had been nominated as anxious, or who had scored above the cut-off on the RCMAS. They were asked to identify students from this list who (i) did not speak English at home, (ii) had substantial learning problems, disability or developmental delay or (iii) clearly had no anxiety problems. Thus, 396 students were identified in the total at-risk sample.
Assignment of schools to intervention and control conditions
Students in the at-risk sample were randomly allocated to the intervention or monitoring condition on the basis of their school. Nine schools were allocated to the monitoring condition (n = 137, from a screened sample of 1046), and 10 to the intervention condition (n = 259, from a screened sample of 1331). A second-stage student and parental consent was obtained for students in the intervention condition, with 136 students commencing the intervention. In total, 260 students were included in the study.
Baseline diagnosis
All students were interviewed for the presence of DSM-IV mood and anxiety disorders using the K-SADS by four interviewers with a clinical psychology background who were blind to condition assignment. Four interviews provided unreliable data and were coded as missing.
Intervention and monitoring
The FRIENDS programme was implemented in each school by a school counsellor assisted by a support teacher, who all attended a 2 day training workshop. The programme was run within normal school hours. Regular supervision was not scheduled because we were interested in the implementation of the programme under normal school conditions. All contacts with the research team related to practical difficulties in the scheduling of sessions. The control schools received no intervention but were told that they would be contacted for monitoring in 2 and 4 years time.
School counsellors completed a measure after each group session of how well they believed that the aims of each session had been met, and were asked to audio-tape group sessions. The majority of aims were rated as having been met extremely well (49.0% of ratings) or moderately well (44.8% of ratings). Forty per cent of schools provided rateable audiotapes, which showed that 55% of session aims were rated as having being met either moderately or extremely well. In contrast to the core activities for each session, the setting and review of self-practice tasks were rated as being poorly implemented or were not conducted at all.
Follow-up assessments
Students in both conditions completed the RCMAS, SCAS, CDI and the health-care use questionnaire 2 and 4 years after the intervention (in 2003 and 2005, respectively). At the 4 year follow up the computerized CIDI was used to diagnose DSM-IV anxiety and affective disorders in the 12 months prior to the interview. The assessor was blind to condition allocation.
Results
No differences were found between the monitoring and intervention samples in the proportion meeting criteria for a definite K-SADS DSM-IV anxiety disorder at pre-intervention assessment (χ2(1,n = 256) = 1.85, NS); 30.8% met criteria in the intervention sample, and 22.0% in the control sample. A total of 111 students in the intervention sample (81.6% of the initial intervention sample) and 117 students in the monitoring sample (94.4% of the initial monitoring sample) completed the 2 year follow up. One hundred and three students in the intervention sample (75.7% of the initial intervention sample) and 86 students in the monitoring sample (69.4% of the initial sample) completed the 4 year follow up. No significant differences were found between the students who dropped out from the study and the final sample on any demographic or baseline symptom measure.
Effect of intervention on outcome measures over time
Because the study design involved randomization by clusters (or schools) random-effects regression analyses using MIXREG [13] were used to estimate the amount of intraclass correlation IICC) in the data. The additional variance parameters for school clusters were not statistically significant (α = 0.05; SCAS ICC = 0.079 NS, CDI ICC = 0.048 NS, RCMAS ICC = 0.083 NS) and it was appropriate to analyse the data at the individual level.
An intention-to-treat analysis was used, in which the most recent score was carried forward to subsequent missing data points. In order to predict anxiety and depression scores based on intervention condition status, analyses of covariance were conducted with the pre-intervention scores as covariates. Controlling for pre-intervention scores, there were no significant intervention effects at the 2 year follow up on the RCMAS (F(1,257) = 1.52, NS), SCAS (F(1,257) = 0.23, NS) or CDI (F(1,257) = 0.67, NS). At the 4 year follow up, controlling for pre-intervention scores, there was a significant main effect for RCMAS scores (F(1,257) = 4.53, p < 0.05), but no effect for SCAS (F(1,257) = 3.12, NS) or for CDI scores (F(1,257) = 1.80, NS). The results in students who met diagnostic criteria for an anxiety disorder prior to the intervention were identical, only the RCMAS at 4 years showed a significant difference.
Means and standard deviations on questionnaire measures for the intervention and monitoring conditions before intervention, after intervention and at the 2 year and 4 year follow ups are shown in Table 1. Effect size differences were calculated using the pooled sample pre-intervention standard deviation, and these are also presented in Table 1 with 95% confidence intervals. The average effect size change for the intervention condition was 0.82 units, and 0.46 units in the monitoring condition. The between-group effect size differences were, however, no different from 0 on most measures at both the 2 and 4 year follow up. In summary, both analyses of covariance and effect size data indicate that there was little significant improvement in the intervention condition relative to the monitoring condition over the 4 years of the follow up.
Outcome measures
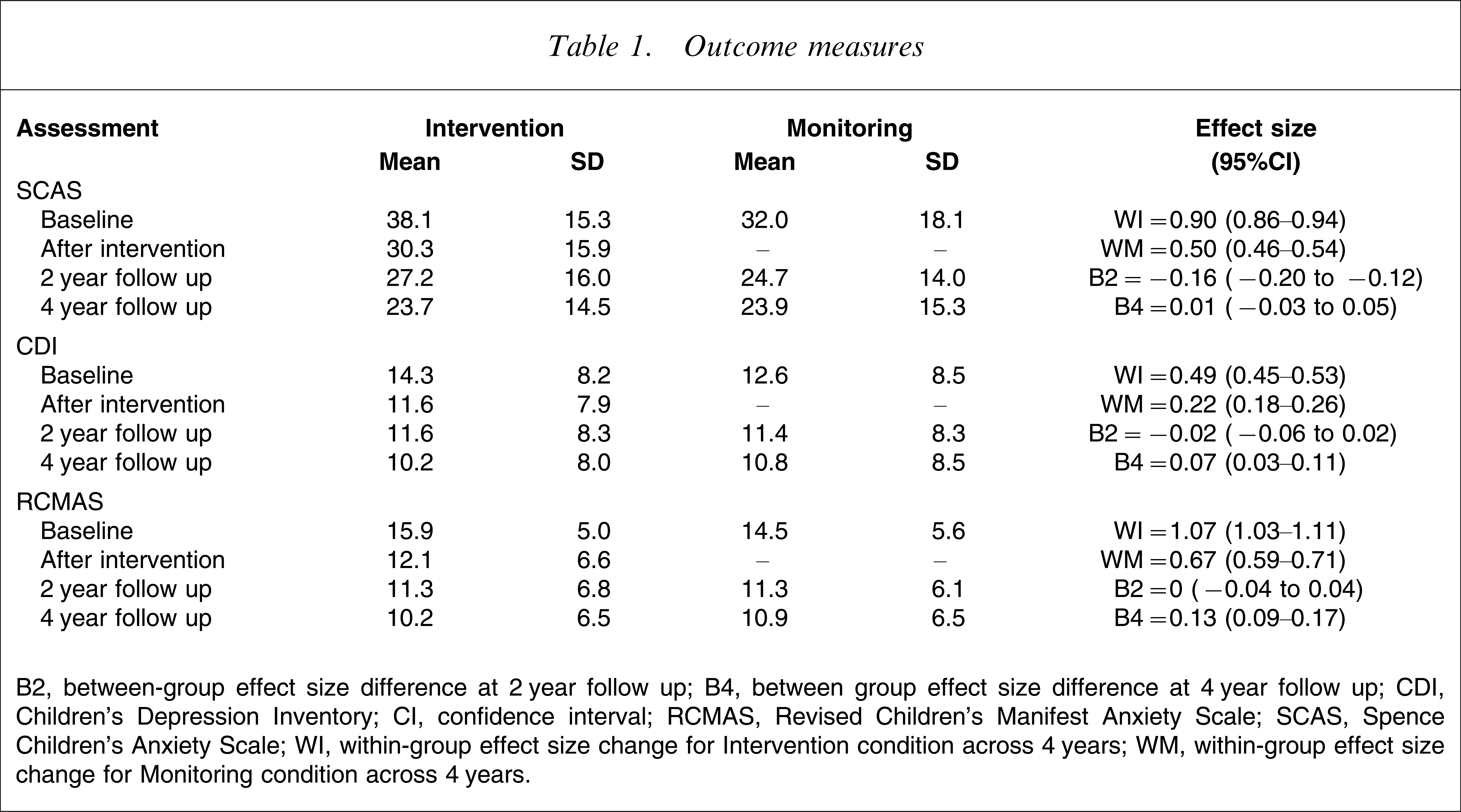
B2, between-group effect size difference at 2 year follow up; B4, between group effect size difference at 4 year follow up; CDI, Children's Depression Inventory; CI, confidence interval; RCMAS, Revised Children's Manifest Anxiety Scale; SCAS, Spence Children's Anxiety Scale; WI, within-group effect size change for Intervention condition across 4 years; WM, within-group effect size change for Monitoring condition across 4 years.
Thirty per cent of the sample met diagnostic criteria for an affective or anxiety disorder in the 12 months prior to the 4 year follow up. There was no difference in the rates of disorder between the intervention sample (33/103, 32.0%) and the monitoring sample (23/86, 26.7%; χ2(1,n = 189) = 0.63, NS). There were 40 new cases of an anxiety or mood disorder at the 4 year follow up with no difference between the intervention and monitoring samples (25/73, 34.2% vs 15/68, 22.1%; χ2(1,n = 141) = 2.57, NS). Over the 2 years to the 2 year follow up, or from that to the 4 year follow up there were no significant differences between the intervention and monitoring samples on the number of visits to a health professional for problems with stress, anxiety or depression.
Discussion
The study aimed to replicate the Queensland Early Intervention and Prevention Project [6] but added a long-term follow up in dimensional and categorical terms, assessment of treatment fidelity, and delivered the intervention by school counsellors and teachers not by clinical psychologists. This trial scored 38–40 of 42 possible points on the Cochrane Collaboration Depression and Anxiety Network Quality Rating System [14]. No differences in outcomes between intervention and control groups could be found when controlling for the pre-intervention assessments. A number of explanations can be considered for these findings. The improvement over time in both conditions may well be attributed to maturational effects. Despite evidence of reasonable treatment fidelity, the use of school counsellors and teachers is the principal difference to other programmes that have used clinicians with a cognitive behaviour therapy background. Minimal parental involvement may have diluted the intervention effect but Mifsud and Rapee produced strong intervention effects with minimal parental involvement [15]. Last, the older age of the current sample relative to the Dadds et al. sample [6] may be a factor; and weak intervention effects have since been found in other high school samples [16, 17].
The measures used were psychometrically sound; taking the clustering of data into effect, the power of the study was sufficient to detect meaningful differences between the conditions, and the follow up was 4 years in duration. Furthermore, the study addresses a gap in the prevention research literature by focusing on the implementation of an intervention that already has demonstrated efficacy in routine school practice when delivered by clinicians. An important outcome of preventative approaches is whether school staff can acquire adequate skills in the delivery of the intervention and whether schools will keep up the implementation of such programmes [18, 19]. Although the treatment integrity data for the current study were incomplete, the available information suggested that trained school staff were able to meet the key aims of each session plan. Of more concern was the lack of emphasis on between-session practice, which may have limited the generalization of skills from the programme into the adolescents’ daily lives. Closer ongoing supervision of the school staff may have overcome this problem, but also would have countered our aim for an evaluation under conditions of routine practice. The present results suggest that for an indicated intervention of this type to be effective specialist mental health staff are needed to run it. Although the programme was acceptable to teachers, the question of ongoing support by the institution is clear. Despite the initial enthusiasm, no school involved in the present study had continued to run the FRIENDS programme in the 4 years of follow up.
The study provides information about the gap between the efficacy of a cognitive behavioural school-based programme delivered by clinicians and the effectiveness of a similar programme delivered by school staff. There have been calls for the evaluation of the effectiveness, as opposed to efficacy, of early intervention approaches [20] and the importance of clarifying the conditions under which such approaches do and do not work [21]. The present results suggest that the routine implementation of early intervention programmes for early adolescents by school staff may not be effective. Future research needs to determine the conditions under which such interventions will have the largest impact on anxiety and depressive disorders relative to the cost of implementation.
Footnotes
Acknowledgements
This research was supported by a grant from the National Health and Medical Research Council of Australia. We thank the Catholic Education Office Sydney for their support of the project, and all the schools and students who agreed to participate in the research. This trial has been registered with the Australian Clinical Trials Registry (ACTR; ![]() . ACTRN012607000254493).
. ACTRN012607000254493).