
Abstract
The prevention of depressive disorders may be an important way to reduce the disease burden. All three types of prevention (universal, selective, and indicated) have potential but also have important limitations. Increasing evidence suggests that universal prevention, aimed at a population, may have no impact on the incidence of depression. Selective prevention, aimed at high-risk groups, is probably effective but may be mostly helpful for those who already have problems. Indicated prevention, aimed at people with depressive symptoms but no disorder, is also probably effective, but uptake is very low. Innovation in the field is very much needed, including well-powered and longitudinal trials aimed at important determinants, such as poor parenting, interparental conflict, and family instability, but also inequalities, social status, and migration.
Approximately 280 million people worldwide suffer from depressive disorders, and 6% of all “years lived with disability” can be attributed to depression (World Health Organization, 2022). Depression is also associated with enormous economic costs, mostly because of productivity losses (Greenberg et al., 2021). Although evidence-based treatments are available (Cipriani et al., 2018; Cuijpers, Quero, et al., 2021), modeling studies have shown that current treatments can only reduce the disease burden of depression in the population by one third (Andrews et al., 2004). Furthermore, despite a strong increase in the number of people seeking treatment for depression in the past decades, the prevalence of depression has not decreased (Ormel et al., 2022).
Preventing the onset of depressive disorders may be an alternative method for reducing the disease burden. There are three types of prevention: universal, selective, and indicated (Institute of Medicine, 2009; Mrazek & Haggerty, 1994; National Academies of Sciences, Engineering, and Medicine, 2019). Universal prevention is aimed at a population, regardless of the risk status of this population (e.g., prevention programs at schools or universities); selective prevention is aimed at high-risk groups (e.g., people who recently experienced a stressful or traumatic event, children of parents who are depressed, older people in nursing homes); and indicated prevention is aimed at people with some depressive symptoms but who do not meet the criteria for a depressive disorder. Interventions aimed at people who meet criteria for a depressive disorder are treatment, not prevention.
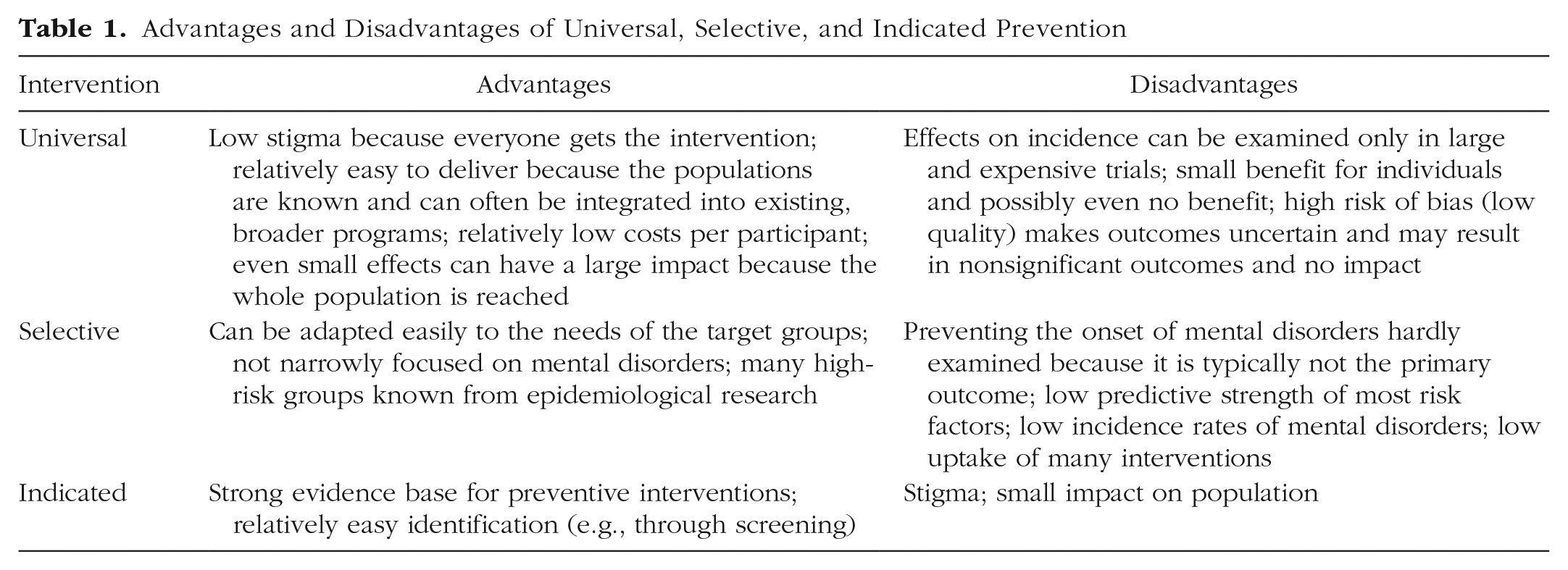
In this article I first give an overview of the state of the art of the three types of prevention and then give an overview of future directions for the field. The advantages and disadvantages of the three types of prevention are summarized in Table 1.
Advantages and Disadvantages of Universal, Selective, and Indicated Prevention
Universal Prevention
Universal-prevention programs are generally conducted in a specific setting, such as a “life-skills” training program at high schools or universities, a mental-health-awareness program in the work setting, or psychoeducational programs in perinatal care to prevent the onset of postpartum depression. These programs are attractive for several reasons. First, stigma is low because they are administered to all persons within the population rather than specific high-risk groups or people who already have a depressive disorder. It is also relatively easy to deliver the interventions because the populations are known and can often be integrated into existing, broader programs, such as health education at schools or well-being programs in the workplace. Because these interventions are delivered in larger populations, the costs per participant are also usually low, although the required resources may still be considerable because of the large number of participants in the interventions.
However, there are also important disadvantages to such programs, the most important of which is the difficulty in showing that prevention programs have prevented the onset of depressive disorders. In all preventive interventions it is important to establish that participants do not have a disorder at the start of the program (otherwise it would be treatment instead of prevention). Furthermore, it must be established that, for example, after 1 year the people who received the program developed a disorder less often than people who did not get the program. The presence of a depressive disorder at baseline and posttest can be established only with diagnostic interviews, which are expensive and require considerable resources.
Furthermore, the number of people developing a disorder within a year is small. It has been estimated that the incidence of major depression in the general population is 1.7% per year (De Graaf et al., 2002). Suppose we want to conduct a randomized trial showing that a universal preventive intervention can reduce this incidence from 1.7% to 1.4% (a reduction of 15%). Calculations of “statistical power” show that such a trial would need to include 60,422 participants (30,211 in the treatment and control group; Cuijpers, 2003). Conducting expensive clinical interviews in such large numbers is not feasible.
Most research has focused on prevention programs in high schools, including universal interventions in the classroom, but also indicated interventions aimed at students with subthreshold symptoms. Randomized trials examining the effects of these programs usually measure outcome in terms of the reduction of symptoms in students who received the program compared with students who did not. For example, a meta-analysis of psychological interventions for preventing depression in children and adolescents reported continuous outcomes for only 40 of 76 trials (Hetrick et al., 2016; Cuijpers, 2022a). These studies cannot really show whether the incidence of new cases of depression has been prevented, but they do show whether such programs have beneficial effects on symptoms of depression. Meta-analyses of these programs usually show small but significant effects on depression (Hetrick et al., 2016; Werner-Seidler et al., 2021), meaning that participants in these programs have lower levels of depressive symptoms after the intervention than those who did not participate. However, many of these studies are relatively small and underpowered, and the quality of most is suboptimal. If such an effect is small but is realized in large groups (all students of a high school), then the impact is large. The impact can be seen as the product of the effect and the number of people getting it. A large effect in a small group of people (e.g., individuals with a disorder) can have less impact than a small effect in a large group of people (e.g., in prevention programs).
The problem is that in universal prevention it is not clear whether the effects are small (and the impact large) or whether the effects are caused by the suboptimal quality and small sample sizes of the studies. Several recent large and well-designed randomized trials have suggested that the effects may be absent and that universal prevention is not effective in schools (Cuijpers, 2022b; Kuyken et al., 2022).
Selective Prevention
There are many high-risk groups that are known to have an increased risk of developing depressive disorders, ranging from children of depressed parents and those with childhood abuse or trauma to caregivers of chronically ill patients and those who experienced a stressful life event. Selective prevention, aimed at such high-risk groups, is often not stigmatizing because people participate in such interventions not because they are depressed but because they are part of the high-risk groups. Examples of selective interventions are support groups for patients and psychoeducational programs for caregivers of dementia patients.
One problem with risk factors in mental health is that the predictive value is typically not very high. This means that most people in such a high-risk group will not develop a depressive disorder in the coming year or 2 years, despite the increased risk (Cuijpers, Furukawa, & Smit, 2021). Although the incidence is higher than in universal prevention, the number of people that must be included in randomized trials to conclude that an intervention is indeed preventing the onset is still very high. So again, such trials are very expensive and logistically very challenging. Furthermore, most studies examining the effects of these interventions do not examine the effects on the incidence of depression but on the reduction of symptoms and improvement of well-being (which are much easier to examine than incidence because they do not need clinical interviews and require substantially smaller sample sizes). This is not a problem of selective interviews in themselves but more of current research practices.
Another problem is that many people who participate in selective interventions already have mental-health problems such as depression, and that is exactly the reason why they participate in these interventions. It is a way of coping with the problem they have. This means that many participants in selective interventions already have a disorder and prevention is no longer possible.
On the other hand, there is evidence that selective prevention can indeed reduce the incidence of depressive disorders. Cuijpers, Pineda, et al. (2021) conducted a meta-analysis of randomized controlled trials comparing preventive interventions in people who had no disorder at baseline (according to a clinical interview) and were randomized to the intervention or a control group, and then another interview was conducted at follow-up to examine how many of them developed a disorder. The authors included 16 randomized controlled trials comparing selective interventions to control conditions. These interventions focused, for example, on supporting children of depressed parents, caregivers of dementia patients, and people with general medical disorders. The authors found that the incidence rate ratio (IRR) was 0.79, 95% confidence interval (CI) = [0.64, 0.99]. This means that those who received the intervention had a 21% less chance to develop a depressive disorder than those who did not receive it. And this was a significant effect. Maybe the number of people who participate in selective prevention and have no disorder is relatively small, but preventing the onset in this subgroup is possible.
Indicated Prevention
Most research has examined the effects of indicated prevention, aimed at people who have some symptoms of depression but who do not meet the criteria for a disorder. Such interventions are often group interventions or digital interventions that can be described as “light” treatments. They are often based on cognitive behavior therapy or interpersonal psychotherapy but less intensive than full treatments. Cuijpers, Pineda, et al. (2021) identified 33 randomized trials of these interventions. The IRR was 0.81, 95% CI = [0.70, 0.94], indicating that those who received the intervention had a 19% less chance of developing a disorder than those who did not.
This means that a strong characteristic of indicated prevention is that the effects have been established relatively well. In some settings, it is also relatively easy to identify people with subthreshold depression, for example, in schools, in perinatal care, and in general medical care. However, a major problem for indicated prevention is that the uptake is low. For example, up to 2012 almost all people in the Netherlands with subthreshold depression could participate in preventive group interventions at no or very low costs. We estimated that only about 1% of those with subthreshold depression used this opportunity (Cuijpers et al., 2010). Potential participants did not consider themselves as being at risk, thought that such interventions were not effective, or were not willing to participate because of the stigma associated with depression. This is only one example from one country, and possibly digital solutions can help with increasing the uptake. However, considering the barriers to such interventions, increasing the uptake of indicated prevention will be a major challenge.
Next Steps
One could say that the prevention field is stuck. Universal prevention has great potential with even small effects having a huge impact, but there is accumulating evidence that it may not have an effect on the incidence of depressive disorders. It is also almost impossible to show that these interventions reduce the incidence because the required numbers of participants in these trials are enormous, and such trials are therefore extremely expensive. Selective prevention is probably effective, but most participants already have mental-health problems, and these interventions probably indirectly “treat” or support people with existing problems. Indicated prevention is probably effective, with a considerable number of trials supporting its effectiveness. However, the uptake of such interventions is low, meaning that the impact is small, even when it is offered to populations on a large scale. This means that none of the three types of prevention is very promising in terms of having an impact on the onset of disorders in populations. So how should we proceed?
One problem that limits the possibilities of making real progress is that little money is spent on research on the prevention of mental disorders. Woelbert et al. (2020) found that $3.7 billion is spent every year on mental-health research, which is 7% of all health research. At the same time, 16% of the total burden of disease in all disorders can be attributed to mental disorders (Arias et al., 2022). Furthermore, only 7% of this 7% spent on mental-health research is aimed at research on prevention. That is 0.5% of all health research. It is also known that much research that is called “prevention” is in fact treatment research, which was one of the reasons why the Institute of Medicine made this strict distinction between prevention and treatment in the 1990s to make sure that resources for depression research would not be spent on treatment research (Mrazek & Haggerty, 1994). If we really want to make progress in preventing depressive disorders, we need policymakers, funders, and researchers to take the problem seriously and make sufficient resources available for research.
These extensive resources are very much needed for large trials in multiple target populations. For example, school interventions should not just focus on single targets, such as training in life skills in classes, but also on training teachers and other school staff to recognize depression, as well as how to institute antibullying projects, develop good counseling services for those with existing problems, and implement general mental-health policies at schools.
There are also important determinants that have not been targeted in well-powered and long-term randomized trials, such as poor parenting, interparental conflict, family instability, children’s maladaptive personality traits, and poor social and problem-solving skills (Ormel et al., 2019). Effective interventions with a large impact should start early in life, focus on children and parents, and continue across the life course. Prevention programs can only be expected to have an impact when they are long term and structurally embedded in existing public (health) institutions, such as education, pregnancy and childcare, health and social work, and later in the work setting (Ormel et al., 2019). Some social determinants can have a negative effect on mental health and can be used to prevent depression at a more structural level, such as income inequality (Wilkinson & Pickett, 2011) but also low social status and migration. Potential preventive strategies include, for example, policies to reduce inequalities, improve housing, and provide social and material support to disadvantaged populations.
It is also important to conduct more research into individuals’ preferences for prevention services. This is especially important in indicated prevention, in which the uptake is low and people with subthreshold depression are not inclined to participate in preventive services at all. More research on preferences could help with developing indicated interventions that meet the needs of these populations better.
An interesting opportunity to develop effective prevention is to focus on “indirect” interventions (Cuijpers, 2021; Cuijpers & Reynolds, 2022). For example, one trial showed that an intervention aimed at insomnia in older adults with subthreshold depression (no disorder) reduced not only sleep problems but also the incidence of depressive disorders at follow-up (Irwin et al., 2022). This is important because insomnia is less stigmatizing than depression, and mentioning the word “depression” is not even needed to prevent it. The same idea can be used in other populations, for example, by focusing on procrastination and perfectionism in college students (Cuijpers, Smit, et al., 2021) or on stress in the work setting. Randomized trials examining these interventions still need large sample sizes, but once their effects have been shown, they may provide an excellent opportunity to increase the uptake of preventive interventions.
Conclusions
Because of the limited impact of treatments on the disease burden of depression, prevention is an important alternative. However, all three types of prevention not only have important possibilities but also important limitations. Although meta-analyses suggest that universal prevention may have small but significant effects on depression, increasing evidence from large-scale trials suggests that it may not have an impact on the incidence of depression. Selective prevention is probably effective but may be relevant only for a small part of those participating in such interventions. Indicated prevention is also probably effective, but uptake is very low. Innovation of the field is therefore very much needed, including well-powered and longitudinal trials aimed at important determinants, such as poor parenting, interparental conflict, and family instability, but also income inequalities, social status, and migration.
Recommended Reading
Cuijpers, P., Pineda, B. S., Quero, S., Karyotaki, E., Struijs, S. Y., Figueroa, C. A., Llamas, J. A. & Muñoz, R. F. (2021). (See References). Systematic review and meta-analysis of trials examining the effects of prevention programs on the incidence of major depression in people with no diagnosis of major depression at baseline.
Herrman, H., Patel, V., Kieling, C., Berk, M., Buchweitz, C., Cuijpers, P., Furukawa, T. A., Kessler, R. C., Kohrt, B. A., Maj, M., McGorry, P., Reynolds, C. F., III, Weissman, M. M., Chibanda, D., Dowrick, C., Howard, L. M., Hoven, C. W., Knapp, M., Mayberg, H. S., . . . Wolpert, M (2022). Time for united action on depression: a Lancet-World Psychiatric Association Commission. Lancet, 399, 957–1022. Overview of the current state of knowledge on depression.
National Academies of Sciences, Engineering, and Medicine (2019). (See References). Comprehensive overview of the field of prevention in young people.
Werner-Seidler, A., Spanos, S., Calear, A. L., Perry, Y., Torok, M., O’Dea, B., Christensen, H., & Newby, J. M. (2021). (See References). Systematic review and meta-analysis of randomized trials examining the effects of school-based prevention programs.
World Health Organization. (2022). (See References). Overview of the current state of mental-health problems across the world.