
Abstract
Anorexia nervosa (AN) has been distinguished from other Axis 1 disorders in that it is pervasively associated with ambivalence and variable motivation for recovery [1]. This phenomenon has been partly attributed to the ego-syntonic quality of the illness, referring to the ‘sense of pleasure, accomplishment, and moral virtue anorexics derive from their pursuit of thinness’ [2] and it has been proposed that AN may serve a functional purpose by providing identity and a sense of self-worth, despite serious health risks [3]. Treatment is therefore often undertaken reluctantly in response to pleas and demands by family, friends, or medical practitioners and other practitioners, and is characterized by high levels of dropout and poor outcome [4].
Poorer outcome in AN has been variously associated with a wide range of variables, including younger age of onset, longer duration of symptoms, a lower body mass index (BMI), longer time spent as an inpatient, use of purging, and obsessive––compulsive personality [4]. Baseline motivation, however, has been shown to be a powerful and consistent predictor of outcome. Patients in an AN specialist residential treatment programme categorized as having high readiness to change were more than five times likely to have a favourable short-term outcome than patients who were categorized as having low readiness to change [5], and higher levels of motivation account for almost 19% of the variance of weight gain in the first 4 weeks of hospitalization [6].
The transtheoretical model provides a framework for conceptualizing motivation for change in which the process of change is divided into five stages [7]. The first stage, pre-contemplation, refers to being unaware or unwilling to change while the second stage, contemplation, refers to thinking about change. These two stages can be seen to represent low readiness to change [5]. High readiness to change is associated with the last three stages: preparation (having the intention of changing soon), action (actively working to bring about change) and maintenance (working towards relapse prevention). Higher levels of readiness for change have been shown to correlate with positive behavioural change across a variety of problems [8], and the model predicts that treatment failure occurs because the treatment approach does not match the patients’ stage of change [7]. The relevance of this model for AN has received growing attention as evidenced by the development of an assessment tool specific to AN, namely the AN Stages of Change Questionnaire (ANSOCQ) [6].
It has been suggested that motivational interviewing (MI) may be beneficial for engaging individuals with AN in treatment [9], a therapeutic approach derived from the transtheoretical model as a means to help people work through ambivalence and commit to change. A meta-analysis of 72 clinical trials spanning a range of target problems (including alcohol, smoking, HIV, drugs, gambling, diet and exercise) found that the average short-term between-group effect size of MI was 0.77, decreasing to 0.30 at 1 year follow up [8]. Results of the meta-analysis suggested that the effects of MI appeared to persist or increase over time when added to an active treatment, which has been attributable to its effects on treatment retention and adherence.
To date there is little evidence in an AN population to suggest that increasing motivation improves outcome or that we can increase motivation to recover. Of only five studies that have evaluated MI for the treatment of eating disorders, two were involved women with binge eating disorder or bulimia nervosa [10, 11] and three involved AN. Of these three latter studies, none adopted a randomized controlled design. The first of these included 12 women with AN in a group of 19 eating disorder patients and evaluated a pre-treatment motivational enhancement group intervention [9]. Results of that study suggested that motivation to change increased following the intervention. At the 6 week follow up, 90% of participants had entered specialized treatment for the eating disorder. The second was a case series examining the impact of a motivational assessment interview on adolescents with AN [12]. Motivation was assessed to have improved significantly and 80% of the group engaged in an outpatient treatment for AN.
The third study, by Dean et al., was a non-randomized controlled sequential trial comparing motivational enhancement therapy (MET) to a treatment-as-usual (TAU) comparison group with 42 consecutive admissions to an inpatient eating disorder unit, in which 50% of the participants met DSM-IV criteria for AN [13]. In addition to taking part in the standard hospital programme, patients in the MET group commenced therapy within the initial 2 weeks of admission, attending four sessions over 4 weeks. The MET sessions were designed to encourage participants to engage in the standard cognitive behavioural hospital programme. Dean et al. found no significant differences between the two treatment groups on any of the formal measures. At 6 week follow up, however, 94% of MET completers compared to 45% of TAU completers were engaged in appropriate levels of treatment. It was concluded that, in the context of a small sample size and short follow-up period, results of the study suggested that MET could potentially be useful in improving the outcome of brief inpatient hospitalization for patients with eating disorders.
In order to increase our understanding of the role of motivation in the process of recovery in AN, there were three aims of the current study with respect to an inpatient AN population, assessed over three waves, at admission to hospital (baseline), and at 2 and 6 week follow up. The first aim was to examine whether baseline motivation predicted improvement in eating pathology. The second was to examine whether improved motivation between the baseline and 2 week follow up predicted improvement in eating pathology between the baseline and 6 week follow up. Finally, within the design of a randomized controlled trial that conformed to CONSORT guidelines [14], we investigated whether four sessions of MI conducted by novice therapists added to TAU compared to TAU alone could significantly improve motivation to recover and eating pathology.
Method
Participants
Eligible participants were inpatients at a specialist weight disorder unit in Adelaide who: (i) were on either a 2 week (n=34) or 6 week (n=13) inpatient programme, (ii) were ≥16 years, and (iii) met the criteria for AN (excluding loss of menses and BMI <19 kg m−2). The incorporation of women who met both full- and subthreshold criteria for AN was considered vital in order to increase recruitment rates in a population notorious for treatment resistance and high dropout rates, and justified on the basis of previous research showing this group to exhibit no differences with respect to psychopathology to women with AN who met full criteria [15, 16].
Over a 19 month recruitment period 84 inpatients met the selection criteria; 21 (25%) declined to participate; 47 (56%) consented; 16 (19%) were not recruited for various reasons (e.g. participating in another study, self-discharged prior to assessment). Of the 47 people who participated, there were two male and 45 female subjects aged between 16 years and 37 years (mean=21.85 years, SD=5.37); 11 patients (23%) were ≤18 years of age. The mean BMI of this group at Wave 1 was 16.38 kg m−2 (SD=1.5) and increased significantly at Wave 3 to 16.89 kg m−2 (SD=1.6, t(41)=−2.39, p=0.02). The study was approved by the Flinders Clinical Research Ethics Committee and written informed consent was given by participants.
Procedure
Inpatients were visited within 3 days of their admission and introduced to the study. Following written informed consent, the self-report questionnaire was completed and participants were informed of their randomization to the MI (n=22) or TAU (n=25) condition (one male subject was randomly allocated to each condition), and the Eating Disorder Examination (EDE) [17] was conducted by one of four MI therapists (three female and one male), all of whom were postgraduate clinical psychology students. Randomization was stratified by treatment programme: 2 or 6 weeks. The aim of the 2 week inpatient programme was to support patients in contemplating change and to assist them to determine whether they are ready to engage in the longer 6 week weight gain inpatient programme. The random allocation sequence was generated by block randomization, a computer-generated random number sequence that takes into account the distribution of previous allocations so that groups will be approximately the same size. Primary responsibility for generation of the random allocation sequence was taken by one of the research team not involved in providing MI.
Participants randomized to the MI condition were invited to attend four individual 60 min sessions of MI (average attendance was 3.5 sessions, ranging from two to four sessions) over the initial 2 weeks of their admission. The TAU condition consisted of input from a multi-disciplinary team. The content of the four sessions of MI are summarized in Table 1. Therapists were instructed to conduct sessions in a manner consistent with MI style (collaborative, calm and caring, showing genuine concern, avoidance of arguments and taking guidance from patients’ reactions as to the direction of the session), and structured the sessions around worksheets developed by Treasure and Schmidt [18]. MI sessions were taped so that supervision could be provided by a clinical psychologist experienced in the treatment of eating disorders (TDW). It was difficult to formally assess MI compliance of each session given that these were structured around the information that the patient had provided in the worksheets, but informal assessment of a random selection of one session from each therapist by TDW suggested that adherence to the MI style was considerable to extensive [19].
Content of motivational interviewing sessions
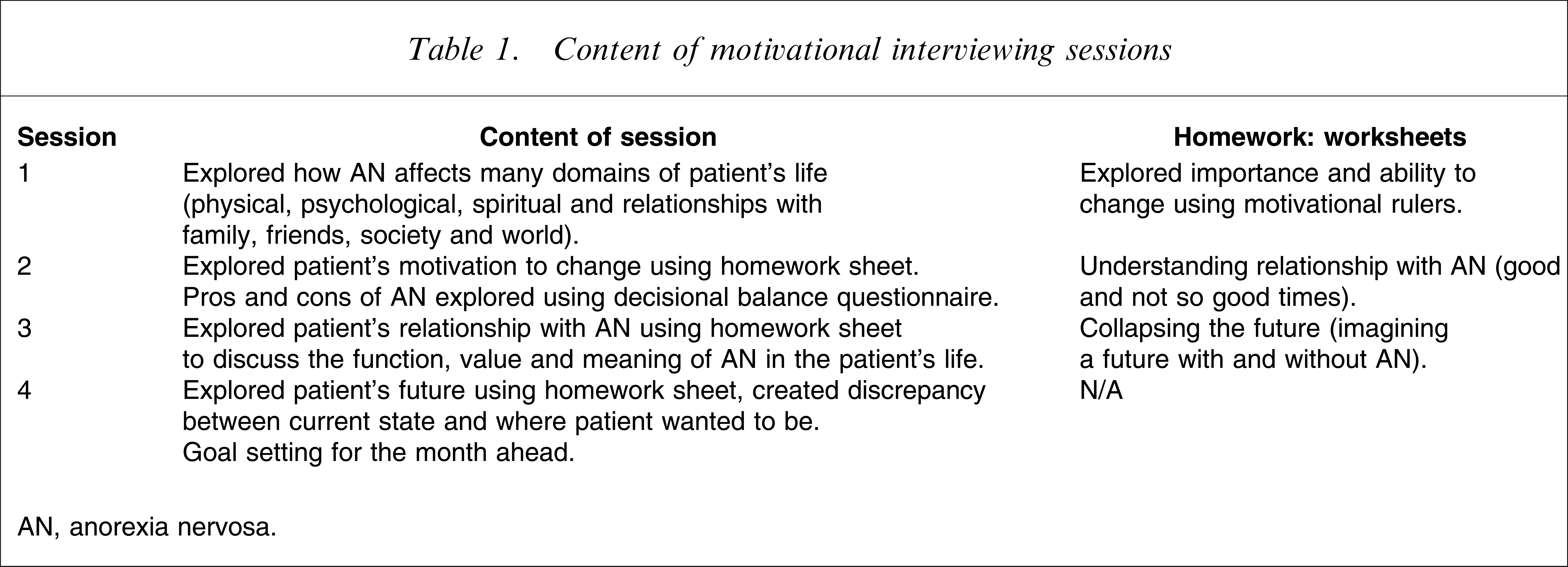
AN, anorexia nervosa.
Assessments were conducted at baseline (Wave 1), 2 week (Wave 2) and 6 week (Wave 3) follow up. Assessments were conducted face to face for participants in hospital and via the telephone for those who had been discharged. In the latter case, questionnaires were posted to participants and answers were collected over the telephone. Two trainee psychologists who were blind to participant condition conducted the follow-up interviews.
Measures
Demographics
At baseline patients were asked to self-report various demographic variables that have been previously shown to influence outcome, including the duration of AN symptoms, age of onset of AN symptoms, and number of prior hospitalizations for disordered eating behaviour. BMI was obtained from the case notes, and presence of purging or objective binge episodes was assessed as part of the eating pathology interview, described below.
Eating pathology
The EDE [17], a semi-structured interview that is accepted as the gold standard for assessing eating disorders [20] was used to assess eating pathology. Although the whole instrument was administered, only the total EDE score is reported in the current study, because any behaviours would be expected to decrease due to force of circumstance (i.e. hospitalization). The total EDE score is made up of four subscales: weight concern, shape concern, eating concern and dietary restraint, and assesses mainly attitudes associated with disordered eating. The internal consistency in the present study was high, with Cronbach's alpha of 0.92, 0.94, and 0.96 at baseline and 2 and 6 week follow up, respectively.
Motivation
The ANSOCQ is a 20-item self-report questionnaire used to assess readiness to recover from AN by assessing the stage of change that participants were in with regard to each symptom of AN, where scores ranged from 1 (pre-contemplation) to 5 (maintenance), with higher scores indicating higher levels of readiness to change [6]. Mean item scores were calculated to derive a total readiness to change score. Rieger et al. demonstrated the ANSOCQ's internal consistency, test–retest reliability and its convergent, discriminant, concurrent and predictive validity [6, 21]. Internal reliability in the present study was high at 0.92, 0.95, and 0.96, at baseline, 2 and 6 week assessment, respectively. In addition to examining the total mean item score, we followed the convention of McHugh [5] and dichotomized the ANSOCQ such that patients with scores <2.5 were categorized as having low readiness to change, and those with scores ≥2.5 were categorized as having high readiness to change.
We also used six self-report questions to assess motivation and self-efficacy to change AN behaviours, in particular, how important, confident and ready participants felt about recovering from their eating disorder and eating normally and gaining weight [22]. Participants responded to each item of a 10-point scale ranging from 1=not at all to 10=very. Each item was analysed independently with higher scores indicating greater levels of importance, confidence and readiness.
Statistical analyses
Analyses were conducted using version 14.0 of SPSS (SPSS, Chicago, IL, USA). In order to address our first aim, namely to investigate whether baseline motivation predicted a change in eating pathology, linear regressions were used to examine the Wave 3 total EDE score as the outcome variable, with the Wave 1 EDE score as the covariate and baseline motivation as the independent variable across the whole sample.
The second aim, which was to investigate whether improved motivation between the baseline and 2 week follow up predicted improvement in eating pathology between baseline and 6 week follow up, was also explored with linear regressions across the whole sample using the 6 week follow-up EDE score as the dependent variable and the baseline EDE as the covariate. The independent variable was the change in motivation between baseline and 2 week follow up.
The third aim, which investigated whether we could change motivation and eating pathology using MI compared to TAU, was examined using linear mixed model analyses [23]. These analyses have the advantage over ANOVAs because all participants (despite missing data from one or move waves) are included in the analyses and accurate parameter estimates can be attained, based on participants’ obtained data [24]. The model calculates a regression line for each individual while controlling for explanatory variables (fixed main effects). In the present study the fixed main effects were treatment (MI, TAU), time (2 weeks, 6 weeks), and the covariate, which was the baseline value of each dependent variable. This approach allows for direct comparisons between the groups at 2 and 6 week follow up despite any baseline differences between the groups because it equalizes the baseline scores between the two groups.
Post-hoc analyses were used to examine any significant main effects and interactions, and the formula MT1 – MT2/SDpooled was used to calculate within-group effect sizes (ES), which assessed the degree of change for each group's mean scores from baseline to follow up. MT1 refers to the raw mean score at baseline, MT2 refers to the raw mean score at 2 week (or 6 week) follow up, and SDpooled refers to the mean SD for both groups combined at baseline. It has been proposed that 0.20 is considered to be a small effect, 0.50 moderate, and 0.80 a large effect [24].
Results
Descriptives of group membership
As shown in Table 2, despite random allocation to treatment condition, some significant differences between the two groups existed at baseline. Independent samples t-tests found statistically significant differences in age of patients, in that patients in the MI group were significantly older than patients in the TAU group. Duration of AN symptoms at baseline was also significantly different between participants, in that those with longer duration were in the MI group. Therefore, age and duration of AN symptoms were entered as covariates in all analyses that compared these two groups. With respect to the motivation and eating pathology variables, no significant differences were found between the groups, with the exception of the stage of change of the participants. At baseline, significantly more participants in the TAU condition were categorized as high readiness to change than those in the MI condition. At the 6 week follow up there was no difference in days in hospital between the two groups, with participants in both the MI and TAU group spending an average of 21 days in hospital, with respective SDs of 11.86 and 11.83.
Baseline subject characteristics
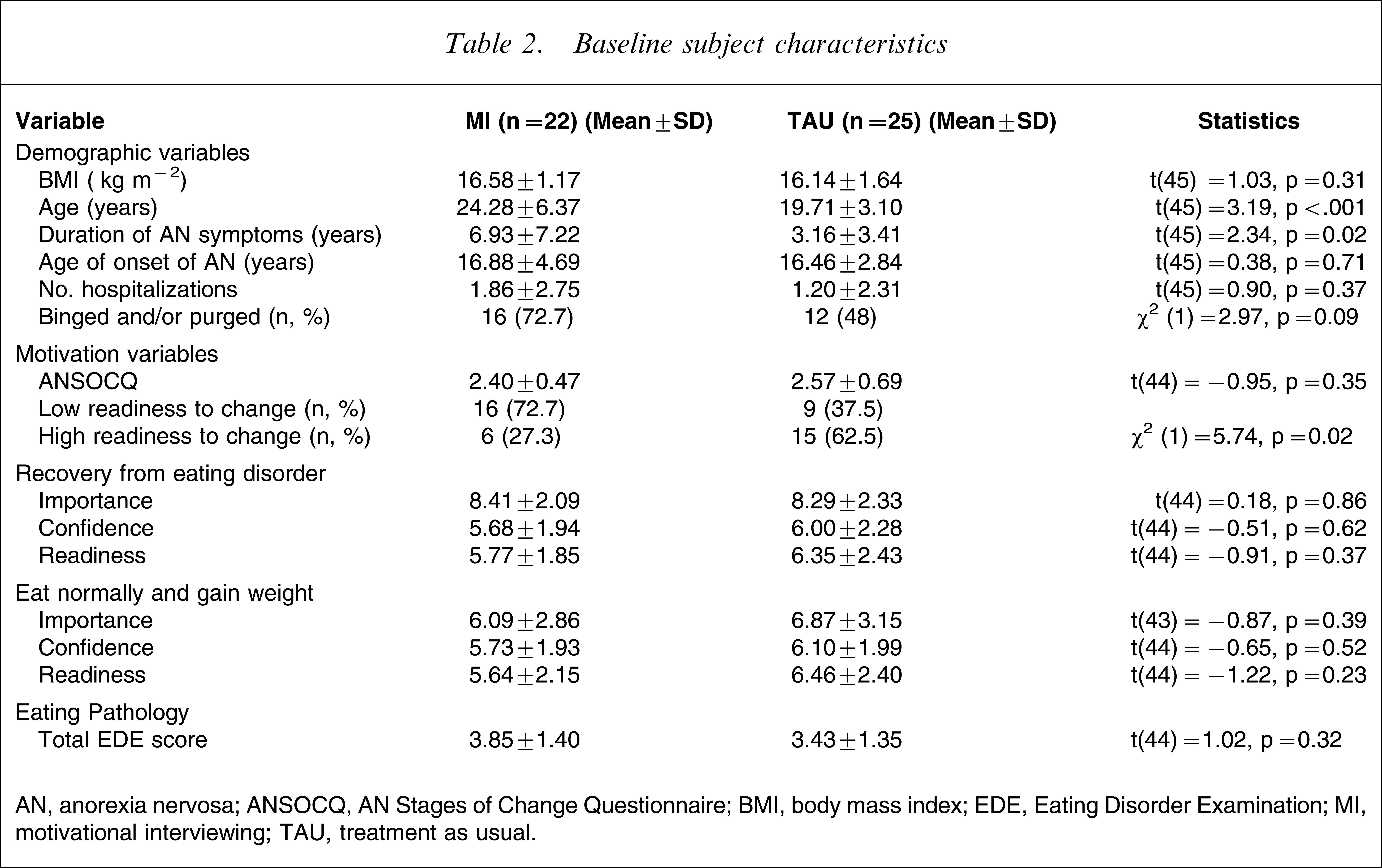
AN, anorexia nervosa; ANSOCQ, AN Stages of Change Questionnaire; BMI, body mass index; EDE, Eating Disorder Examination; MI, motivational interviewing; TAU, treatment as usual.
Attrition rates
As can be seen in Figure 1, the overall attrition rate at 6 week follow up was 17.0%, and 78.7% of those recruited completed both the self-report questionnaire and the clinical interview and 4.3% completed only the questionnaire or the interview. Of the eight participants who withdrew, significantly more came from the TAU (n=7, 87.5%) than the MI group (Fisher's exact test (one-sided)=0.03). In other words, participants from the TAU group were 1.33 times (95% confidence interval=1.03–1.72) more likely to withdraw from the study than the MI participants.
Flow of participants through treatment. MI, motivational interviewing; TAU, treatment as usual.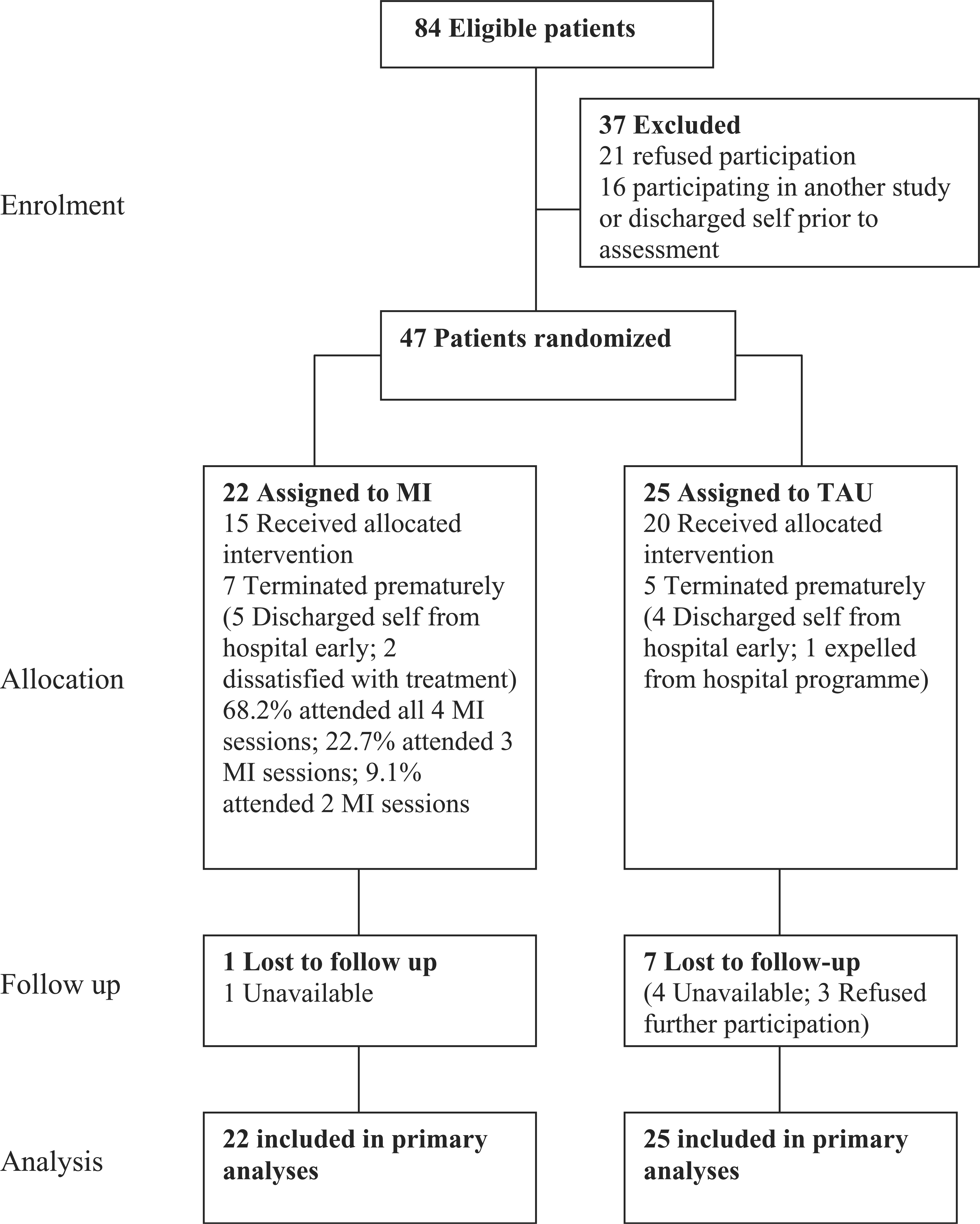
Baseline motivation and change in eating pathology
In order to examine whether any covariates should be included in the following analyses, the relationship between five baseline demographic variables and the change in the total EDE score over the 6 week period was examined. There were no significant relationships between the demographic variables and changes in psychopathology, including duration of the AN (β=−0.10, p=0.39), age of onset of AN (β=−0.02, p=0.88), baseline BMI (β=−0.02, p=0.84), purge/binge behaviour (β=−0.08, p=0.50), and number of previous hospitalizations for disordered eating (β=−0.04, p=0.75). Therefore, no covariates were included in the regressions examining motivational variables, with the exception of the total EDE score at baseline, the results of which are shown in Table 3. It can be seen that across the whole sample, five of the six single Likert scale motivational variables predicted change in the total EDE score, in that higher levels of baseline motivation predicted a decrease or improvement in the total EDE score between baseline and 6 week follow up. Confidence in ability to eat normally and gain weight and the total ANSOCQ score did not predict a change in the EDE score.
Predictors of total EDE score at 6 week follow up
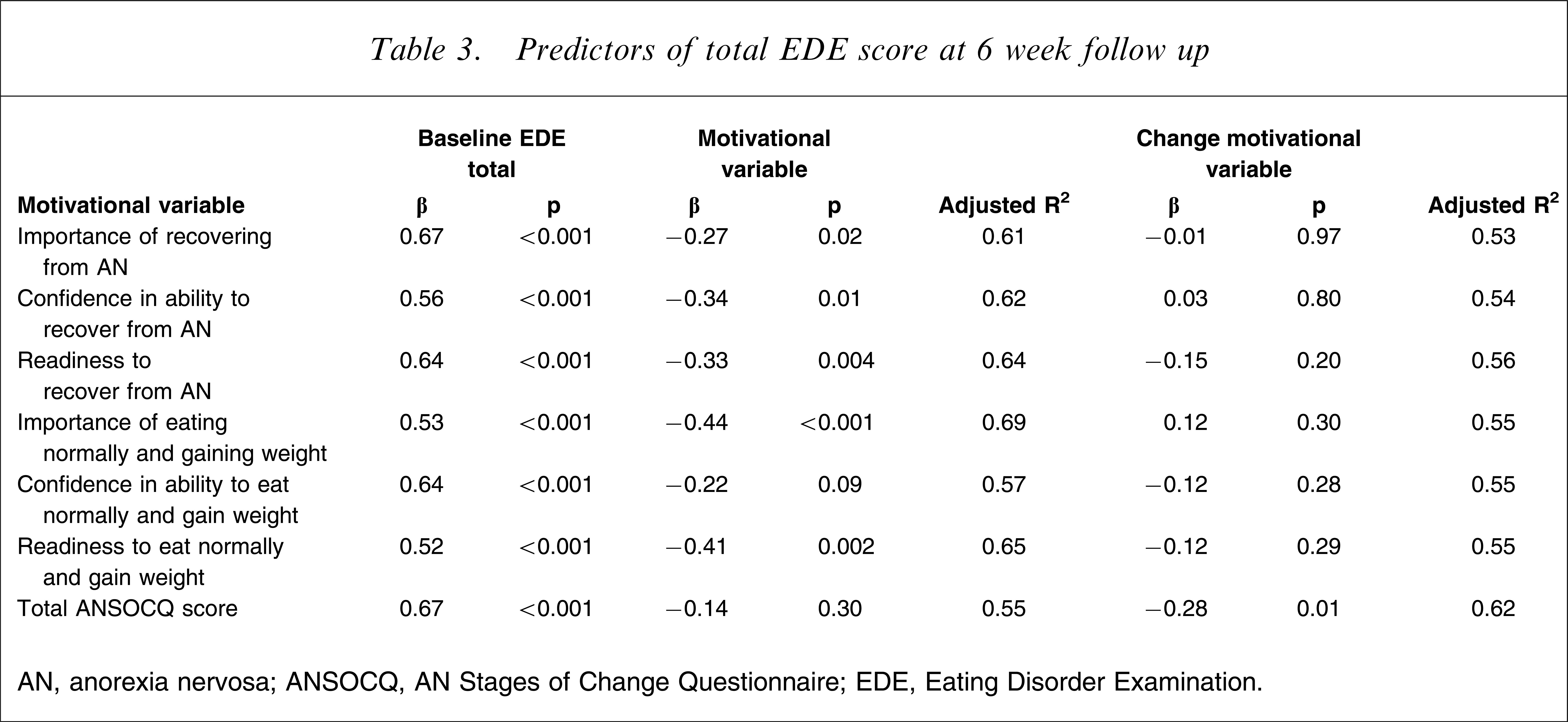
AN, anorexia nervosa; ANSOCQ, AN Stages of Change Questionnaire; EDE, Eating Disorder Examination.
Changes in motivation and changes in eating pathology
The relationship between changes in motivation between baseline and 2 week follow up and the changes in the total EDE score between baseline and 6 week follow up is also shown in Table 3. Across the whole sample, only changes in the total ANSOCQ score over a 2 week period predicted change in eating pathology over a 6 week period, where increases in motivation predicted decreased eating pathology.
Impact of MI versus TAU on motivation
Table 4 lists the estimated marginal means and standard errors over time for both programmes. No significant time × programme interactions or main effects of group were found. A significant main effect of time, however, for the Motivation to Change Scale items ‘Importance of recovering from the eating disorder’ (F=5.04, p=0.03) and ‘Importance to eat normally and gain weight’ (F=4.79, p=0.04) was indicated. In the first instance, across both groups, there was a small increase in motivation over the 2 week follow up but a significant drop in motivation below baseline at 6 week follow up. With respect to importance of eating normally and gaining weight, the MI group increased in motivation at the 2 week follow up and then significantly decreased at 6 week follow up, but did remain above baseline. In contrast, the TAU group had a small increase followed by a significant decrease and ending below baseline. We also examined whether the total EDE changed over time differently between the groups and, although no significant effects were found, it can be seen after a initial decrease in both groups between baseline and 2 week follow up: the total EDE score for the MI group continued to decrease between 2 and 6 week follow up, whereas it increased for the TAU group.
Means and within-group effect sizes
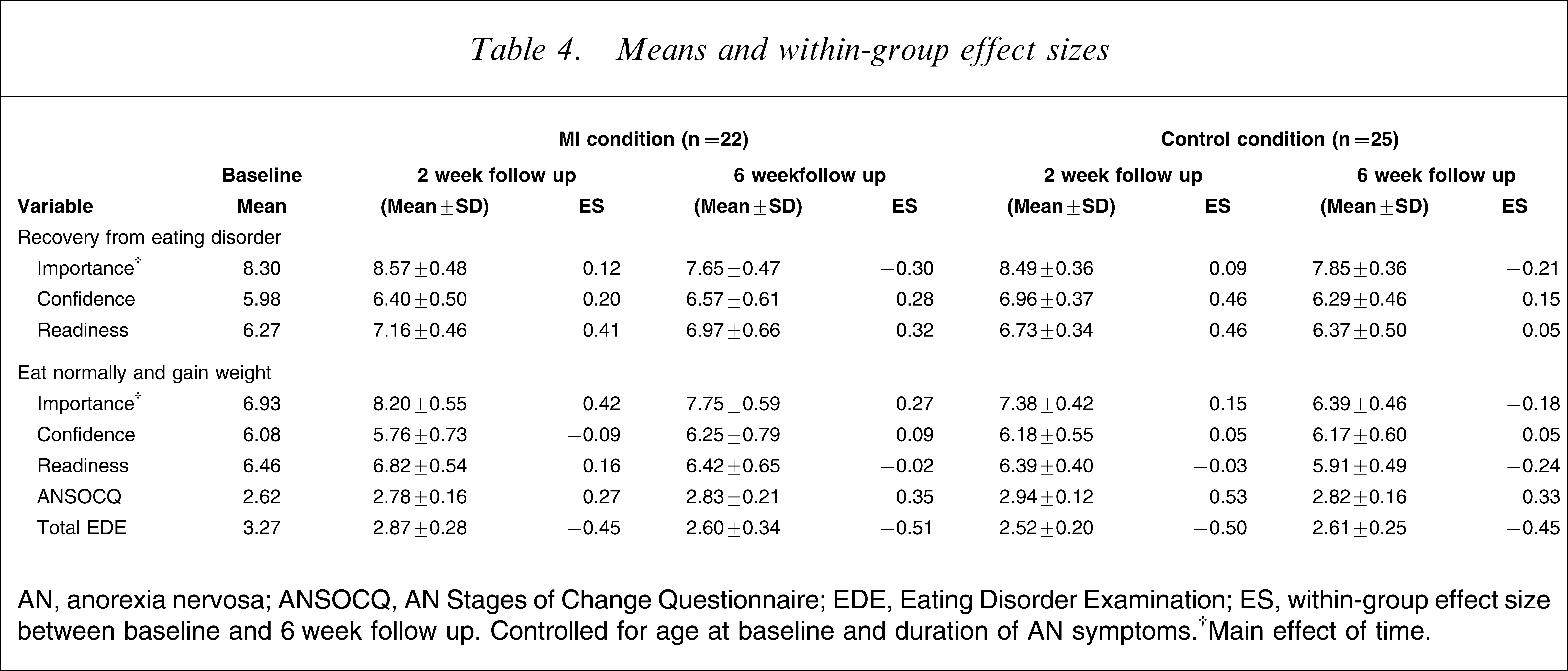
AN, anorexia nervosa; ANSOCQ, AN Stages of Change Questionnaire; EDE, Eating Disorder Examination; ES, within-group effect size between baseline and 6 week follow up. Controlled for age at baseline and duration of AN symptoms.†Main effect of time.
When looking at the dichotomous categorization of the ANSOCQ, of the 15 patients in the MI condition who were categorized as having low readiness to change at baseline (and who completed the ANSOCQ at both time points), nine (60%) had moved to high readiness to change at 2 week follow up and six stayed at low readiness to change. In contrast, of the seven patients in the TAU condition who were categorized as having low readiness to change at baseline (and who completed the ANSOCQ at both time points), only one patient (14.3%) moved to high readiness to change at 2 week follow up and six (85.7%) stayed at low readiness to change (Fisher's exact test (one-sided)=0.059). The effect size was moderate to strong (Cohen's w=0.43), where an effect size of 0.3 is considered moderate and 0.5 strong [25]. This pattern of results was identical at 6 week follow up, indicating that the move from low readiness to change to high readiness to change was maintained at 6 week follow up.
Conclusions
The current study investigated the role of motivation and its ability to predict change in disordered eating pathology and the efficacy of MI in enhancing readiness for change in inpatients with AN. With respect to our first aim, we found baseline motivation to be a significant predictor of change in eating pathology. Four of our six motivational variables accounted for between 61% and 69% of the variance of change in the total EDE score when taking into account the initial EDE score. In contrast, demographic variables that have been previously but inconsistently found to predict change in AN [26, 27] were not significantly associated with change, including duration or age of onset of the AN, baseline BMI, purge/binge behaviour and number of previous hospitalizations for eating problems. The baseline single Likert Motivation to Change Scales accounted better for change than the ANSOCQ, indicating that these simple scales may be of value in predicting the degree of change that can be expected in inpatient settings. The differences between the motivational measures highlight the need to continue to investigate and develop valid, reliable tools in the area of motivation for change in eating disorders. Overall, this finding adds to the growing body of clinical literature [5, 6] suggesting that it is important to focus on motivation in the treatment of AN, a variable that literature from other clinical areas shows can be manipulated, and improve the effectiveness of treatment [8].
To date, in the clinical area of AN it has not been convincingly shown that changes in motivation are associated with change in treatment. Investigation of our second question, namely whether improved motivation between the baseline and 2 week follow up predicted improvement in eating pathology between the baseline and 6 week follow up, showed that it was only change in the total ANSOCQ score that predicted change in the total EDE score. In contrast to the results of the investigation of our first aim, it appears that the single Likert scales do not have enough variance to adequately assess change in motivation. The ANSOCQ, a tool mapped on the transtheoretical stages of change model, and adapted specifically for AN, is more sensitive for this purpose, accounting for 62% of the change in eating pathology along with the baseline eating pathology score. It would therefore appear important to increase motivation as measured by the ANSOCQ in order to maximize opportunities for change in eating pathology.
With respect to our third aim we investigated whether four sessions of MI [18], offered by a novice therapist, would be sufficient to increase motivation and/or eating pathology in contrast to a TAU group. Overall, we did not find that MI significantly enhanced motivation or decreased eating pathology, but there are two aspects of our results that do support the suggestion that the utility of MI for enhancing treatment outcome in AN should be further investigated. First, there was a significantly lower dropout in the MI group as compared to the TAU group in terms of follow-up assessment. In the face of high dropout of therapy for both outpatient and inpatient AN ranging from 31% to 63% [27–29], retention of patients in therapy is considered essential in order to offer potentially useful treatments. Second, approaching significance at the p=0.06 level was our finding that more people in the MI group crossed over from the stage of low readiness to change to high readiness to change, as measured by the ANSOCQ. In the context of relatively small sample, the effect size, which is independent of sample size, is informative, and suggests an impact that is moderate. Coupled with the previous finding that change on the ANSOCQ predicted change in eating pathology as measured by the total EDE score, change on this motivational instrument is an important therapeutic goal.
Given that only four sessions of MI were offered by novice therapists, two improvements to our MI protocol are immediately apparent. First, given the difficulties of working with an AN population [1], it may be that use of therapists experienced in working with AN and who have training in MI is required in order to maximize the impact of MI. Second, while two to four sessions of MI is commonly used across other types of problems [8], it may be that this number of sessions is an insufficient dosage with such an intractable disorder as AN. It would not be unreasonable to suggest that double this number of sessions might be considered to be a more adequate preparation for enhancing response to consequent treatment. A third improvement to the current protocol is suggested by the nature of our TAU condition, which for the majority of patients in the present study was a 2 week inpatient assessment programme designed to assist patients to contemplate their motivation to recover from their eating disorder and to determine their readiness for the 6 week programme, which is aimed at behaviour change. It may be possible that we did not see changes in disordered eating behaviour in response to increases in motivation because the treatment programme to which the MI intervention was linked was not specifically aimed at equipping patients with tools for behaviour change. This is in contrast to the study conducted by Dean et al. [13], who aimed MI techniques at fostering engagement within the cognitive behavioural therapy approach of the inpatient unit.
A number of limitations of the current study should be noted. First, it is not possible to attribute changes in the MI group to the MI sessions per se, rather than to the additional attention received from the therapist and the quality of that relationship. As recognized by Fairburn [30], however, until preliminary data are available to support new treatments, it would be premature to implement costly, time-consuming randomized controlled trials. Second, the use of self-report motivational measures may not be as reliable as ascertaining motivation through interview. Third, the 6 week follow up was short and some participants remained in hospital, hence, future research would be improved by the addition of longer follow up.
In summary, results of this research support the importance of motivation in predicting change in eating pathology in AN inpatients. In the current study we report the results of the first randomized controlled trial for MI in the treatment of AN, and on balance we suggest that it is worth further investigating the addition of MI to treatment approaches for AN. Future research should endeavour to increase the power of motivational interventions by adding MI as a prelude to an active treatment aimed at behaviour change, using expert therapists and having more sessions than is typically incorporated in a MI approach.