
Abstract
Neuropsychological, functional and structural imaging studies have supported the presence of dysfunction in the frontal–striatal brain areas in obsessive–compulsive disorder (OCD) [1–6], a highly heterogeneous condition in which individuals present with obsessions and/or compulsions [7]. Consistent with such suggestions, OCD patient groups have demonstrated deficits in executive functioning [2, 3], attention [8], visuospatial abilities [9], non-verbal memory [10] and response time [11]. But although several studies have supported these findings, particularly the presence of visuospatial and executive deficits in OCD [12–14], other studies have not [15, 16]. These inconsistencies could be due to heterogeneity within presentations of the disorder, and to differences between studies in the measures used [1]. Indeed, recent evidence from neuroimaging studies has suggested that the different symptom dimensions may be associated with specific neural correlates [17], and it is possible that different neurological deficits may underlie different clinical presentations.
In this paper we examined whether differences in underlying neuropsychological deficits are linked with particular OCD presentations. The examination of neuropsychological differences between OCD subtypes may have important implications for models of aetiology and management. Subtype differences on neuropsychological profiles may challenge current conceptualizations of OCD as a homogeneous neuropsychiatric disorder [18], and provide a basis for more fine-grained models of the disorder(s). Given current concerns about the ecological and syndromal validity of symptom subtypes [19], profiling of distinct neurocognitive capacities may have heuristic value in determining treatment methods and/or predicting the outcome, severity, course, psychiatric comorbidity and other clinical features of OCD.
Symptom-based schemes have been the most prominent approaches to subtyping OCD [19]. Symptom dimensions such as washing compulsions, checking compulsions, and obsessions without compulsions have consistently emerged in both clinical and non-clinical cohorts [20–23], with other dimensions being apparent depending on the measures used. Research investigating neuropsychological profiles across symptom-based OCD subtypes has focused largely on patients with checking rituals [24–26], although less common subtypes such as hoarding [27] and obsessional slowness [28] have also been examined. Generally, relative to non-checkers, checkers have been found to exhibit greater deficits in general memory, memory for actions, and decreased vividness of memory [24, 29–31].
The most common approach to examining neuropsychological differences across OCD subtypes has been to make direct comparisons of performance levels on standardized neuropsychological tests. This approach, however, has not yielded significant differences between subtypes on tasks of executive functioning or memory [32–34]. The relatively poor sensitivity of some neuropsychological measures used in a range of studies in detecting impairments relevant to OCD may account for the findings [32].
Studies using the Cambridge Neuropsychological Test Automated Battery (CANTAB) [35] have consistently reported findings of impaired neuropsychological performance in individuals with OCD [2, 3, 36]. For instance, Veale et al. found significantly poorer performance among participants with OCD relative to non-clinical controls (NCs) on tasks of set-shifting and planning [36]. Purcell et al. reported poorer spatial memory and spatial working memory (SWM) and slowed motor responses in an OCD cohort compared to NCs, and to cohorts with either panic disorder or major depression [2]. Thus, there is some support for mild impairments in cognitive functioning that are specific to OCD, particularly in the visuospatial and executive functioning domains. It is unclear whether such deficits are associated equally with symptom subtypes.
In the present study we explored the presence of differences between OCD subtypes on neuropsychological tasks of the CANTAB. We administered tasks that had previously indicated deficits in OCD, including tasks assessing executive functioning (spatial span, SWM, planning task), visual memory (pattern recognition, spatial recognition), and attentional set shifting (intradimensional–extradimensional set shift). Consistent with previous research, symptom subtypes were determined on the basis of overt symptoms.
Method
Subjects
Fifty-nine patients with OCD (36 female, mean age=37.8 years, SD=13.3) were recruited from patients referred to the University of Melbourne Psychology Clinic. Diagnosis was confirmed using a semi-structured diagnostic interview, the Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV) [37], administered by clinical psychologists or doctoral level students under supervision, who had received training in ADIS administration. Exclusion criteria included the presence of a head injury, a major medical or neurological illness, significant current or past alcohol or substance abuse, or another current Axis I disorder. At the time of testing 41 participants were medicated, mostly with a serotonergic medication.
Fifty-nine NCs were recruited from the community (36 female, mean age=37.5 years, SD=12.8). They reported no current psychological disorder on the ADIS-IV. The cohorts were matched according to age, gender, education and premorbid verbal IQ as estimated on the National Adult Reading Test (NART) [38].
OCD participants were categorized into subtypes on the basis of their current primary and secondary obsessions and compulsions as indicated on the Yale–Brown Obsessive Compulsive Scale (YBOCS) Symptom Checklist [39] by three clinical psychologists experienced in the assessment and treatment of OCD. All three psychologists had to agree on the classification of subjects into one of four groups. In 60% of cases the psychologists agreed independently on the placement of subjects into one of the four categories. In the remaining 40% of cases, consensus was reached with most of the remaining subjects being classified into the others or mixed symptom profile group.
Four OCD subtypes were identified: (i) washers, presenting predominantly with contamination obsessions, washing and cleaning compulsions; (ii) checkers, presenting with safety concerns, doubting obsessions and checking compulsions; (iii) obsessionals, presenting with few or no compulsions, and obsessional thoughts, images and/or impulses about harm to self or others; and (iv) others or mixed symptom profile (this cohort presented with either a mixture of symptoms such as washing and checking, or other less common obsessive–compulsive symptoms, including exactness, symmetry and order concerns, hoarding, and repeating compulsions).
Procedure
All clinical participants were approached to volunteer for the study when presenting for assessment or treatment. The NCs were recruited through community advertisements. Participants provided written, informed consent after receiving information about the study. Participants underwent the ADIS and clinician-rated measures of OCD severity, depression and anxiety. The clinical cohort also completed the YBOCS Symptom Checklist. In a separate session, computer-based neuropsychological testing was completed in the clinic. CANTAB subtests were presented in a random order on a high-resolution colour monitor with a touch-sensitive screen. Subjects were seated 0.5 m from the monitor and were instructed to respond to stimuli by touching the screen. Testing sessions lasted around 60 min. The tasks were administered according to standard protocols. Finally, all participants completed self-rated measures of anxiety, depression and OCD.
Measures
Anxiety Disorders Interview Schedule for DSM-IV
The ADIS-IV is a semistructured diagnostic interview developed to facilitate reliable diagnosis of mental disorders, particularly those relating to anxiety disorders [37].
National Adult Reading Scale
This test consists of 50 words presented visually in order of increasing difficulty, and requires subjects to read the words out aloud to the examiner while the number of errors is recorded [38]. The NART provides a valid and reliable estimate of premorbid verbal intelligence [40].
Hamilton Depression Rating Scale and Hamilton Anxiety Rating Scale
The Hamilton Depression Rating Scale (HDRS) and Hamilton Anxiety Rating Scale (HARS) are clinician-rated scales of depression and anxiety, respectively, with ratings based on information provided by the subject and observations made during clinical interview [41, 42]. Ratings account for participants’ general level of symptoms and the interference of symptoms in daily functioning over the past month. The 17-item HDRS and 14-item modified HARS [43] were used in the present study.
Yale–Brown Obsessive Compulsive Scale
The YBOCS is a 12-item clinician-rated scale assessing the severity of obsessions and compulsions with respect to time spent, interference, distress, resistance and control [39]. The YBOCS is the gold standard for treatment trials and exhibits adequate reliability [44]. It also provides a Symptom Checklist that allowed identification of primary and secondary obsessions and compulsions.
Beck Depression Inventory
This test contains 21 items that ask recipients to indicate the extent to which they exhibit cognitive, affective, somatic and vegetative symptoms of depression and dysphoria [45]. The psychometric properties of the Beck Depression Inventory (BDI) are well documented.
Beck Anxiety Inventory
The Beck Anxiety Inventory (BAI) is a 21-item self-report measure of clinical anxiety symptoms [46]. Items correspond closely to symptoms of generalized anxiety and panic disorder. It has been found to exhibit adequate psychometric properties across a range of populations.
Padua Inventory–Washington State University Revision
The Padua Inventory is a 39-item self-report inventory that consists of five subscales assessing distress associated with OCD symptoms: (i) thoughts of harm to self or others; (ii) impulses of harm to self or others; (iii) contamination and washing; (iv) checking; and (v) dressing rituals [20, 22]. The Padua Inventory has been shown to be acceptable on numerous indices of reliability and reliability [20].
Cambridge Neuropsychological Test Automated Battery
The CANTAB tasks administered in the present study included Executive Function Tasks (Spatial Span, SWM, Stockings of Cambridge (SOC) Planning Task), Visual Memory Tasks (Pattern Recognition, Spatial Recognition), and an Attentional Set Shifting Task (Intradimensional–Extradimensional Set Shift) [35]. Spatial Span is a computerized version of the Corsi Block Tapping Test and assesses participants’ spatial short-term memory capacity. Participants are shown white boxes that change colour in a specific sequence. The participant is required to repeat the sequence by touching the appropriate boxes. Span length was the outcome measure used in the current study. SWM requires subjects to locate tokens that are hidden in boxes. The task assesses the accuracy of working memory (between-search errors; i.e. returning to search in a box in which a token had already been found during a previous searching sequence). The task also provides a strategy score that indicates the ability to adopt a systematic searching approach. On the basis of findings from previous research [3] only between-search errors and strategy scores were used as outcome measures in the current study. The SOC planning task requires subjects to rearrange a set of balls in a specified minimum number of moves that increase in difficulty. The program records accuracy of planning, and estimates of cognitive speed. A control condition during the task also allows estimation of motor speed. In line with previous findings only cognitive and motor speed were used as outcome measures in the current study [3]. Pattern Recognition measures participants’ ability to recognize a previously presented coloured abstract pattern from two stimuli. Spatial Recognition measures participants’ ability to recognize the spatial location of white boxes previously presented at different positions on the screen. For both Pattern and Spatial Recognition tasks, the percentage of correct responses was recorded. Intradimensional–Extradimensional Set Shift assesses subjects’ ability to maintain attention to different examples within a reinforced stimulus dimension, and then to shift attention to a previously irrelevant stimulus dimension. The task involves nine stages, with subjects proceeding to the next stage when a criterion of six consecutive correct responses is attained. Performance is examined according to the number of trials to criterion at each stage of the task.
Results
Data analyses
The data were analysed using SPSS 16.0 (SPSS, Chicago, IL, USA). Logarithmic transformations were undertaken for the latency scores on the SOC task, to improve skewness. Due to the large number of comparisons, several measures were used to reduce the possibility of type two error. First, the overall OCD sample was compared to the non-clinical cohort on their performance of the selected neuropsychological test outcome measures. Then, a series of ANCOVAs, with depression and anxiety (i.e. HDRS and HARS scores) as covariates, were carried out to examine differences among the four OCD subtypes and NCs, on those tests on which overall group differences (OCD vs NC) were noted. These covariates were determined by previous analyses demonstrating significant correlations between depression and anxiety with neuropsychological performance. Finally, where overall differences were found, Bonferroni post-hoc comparisons were conducted to examine individual group differences. Conservative significance levels of 0.01 were used throughout, with the exception of the Bonferroni post-hoc analyses (p<0.05).
Comparisons on symptoms and background characteristics, and relationships of measures with mood
Baseline comparisons between OCD subtypes and NCs showed no differences on gender, age, years of education or verbal IQ (Table 1). OCD subtypes did not differ on medication status (c2(3)=4.19, p>0.05), age of onset (F(3,54)=0.87, p>0.05) or length of OCD (F(3,54)=0.84, p>0.05). Significant differences, however, were found between OCD subtypes on the YBOCS Total (F(3,53)=4.79, p=0.005) and YBOCS Compulsions (F(3,53)=9.54, p<0.001). As expected, Bonferroni post-hoc analyses indicated that obsessional subjects scored lower than other OCD subtypes.
Subject characteristics vs OCD subtype
BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; C, checkers; HARS, Hamilton Anxiety Rating Scale (14-item); HDRS, Hamilton Depression Rating Scale (17-item); M, mixed group; NART, National Adult Reading Test estimated Verbal IQ; NC, non-clinical control; O, obsessionals; OCD, obsessive–compulsive disorder; PI-R, Padua Inventory–Revised; W, washers; YBOCS, Yale–Brown Obsessive Compulsive Scale.
†χ2 test.
Analyses of covariance indicate a number of subscale differences between the OCD subtypes and NCs on the Padua Inventory of OCD symptoms (Table 1). The NCs generally scored lower across most Padua subscales. Expected differences on the Padua subscales were also found among the OCD subtypes, providing further validity for the classification of individuals into the different symptom subtypes. For instance, obsessionals scored higher on Impulses of Harm to Self or Others than washers; checkers scored higher on the Checking subscale than obsessionals and washers; washers scored higher than all other subtypes on the Contamination subscale. No subtype differences were found on the Dressing/Grooming subscale or on Thoughts of Harm to Self or Others.
For the total combined sample, low magnitude but significant correlations were found between depression and anxiety symptoms and all of the neuropsychological measures, except for initial thought latency on the SOC task, for which only non-significant correlations were observed (Table 2). Scores on HDRS and HARS were used as covariates in subsequent analyses.
Correlations between depressive and anxiety symptom measures and neuropsychological measures overall
BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; EDS, Extradimensional Set Shift Trial; HARS, Hamilton Anxiety Rating Scale (14-item); HDRS, Hamilton Depression Rating Scale (17-item); SOC, Stockings of Cambridge; SWM, spatial working memory.
∗p<0.05 (two-tailed); ∗∗p<0.01 level (two-tailed).
Comparisons on neuropsychological performance
Comparisons between OCD and NC groups indicated significantly poorer performance by the OCD cohort on all neuropsychological measures, with the exception of thinking latency response on the SOC (Table 3).
Comparisons between OCD and NC cohorts on neuropsychological measures
EDS, Extradimensional Set Shift Trial; NC, non-clinical control; OCD, obsessive–compulsive disorder; SOC, Stockings of Cambridge; SWM, spatial working memory.
Comparisons between the four OCD subtypes and NCs on the neuropsychological tasks (specifically, those yielding statistically significant results in the two cohort comparisons) were conducted using a series of ANCOVAs, with depression and anxiety as covariates. After adjustment, significant neuropsychological differences across subtypes and NCs were noted on SWM (between-search errors), Spatial Recognition (% correct), Pattern Recognition (% correct) and SOC tasks (Initial Movement Latency and Subsequent Movement Latency; Table 4). Although all tests exhibited adequate power despite small sample sizes (ranging from 0.78 to 0.96), the effect sizes for the relationships between the neuropsychological measures and symptom-based groups were generally small (Table 4, Appendix I). Bonferroni-adjusted post-hoc comparisons showed that both checkers and mixed groups, compared to NCs, recorded a lower percentage of correct responses on the Pattern Recognition task and longer initial movement latencies on the SOC task. Checkers also performed more poorly than NCs on SWM tasks and more poorly than washers on Pattern Recognition. The obsessionals were significantly less accurate than NCs on Spatial Recognition, while the mixed group compared to the NCs made more between-search errors on the SWM task and had longer subsequent movement latencies on the SOC task. Comparisons between the four OCD subtypes and NCs were restricted by power (0.11–0.65 for the individual comparisons). Significant differences were noted on SOC Initial Movement latency, with post-hoc comparisons indicating slower latencies in checkers compared to washers.
Differences in neuropsychological performance vs OCD subtype
C, checkers; EDS, Extradimensional Set Shift Trial; HARS, Hamilton Anxiety Rating Scale (14-item); HDRS, Hamilton Depression Rating Scale (17-item); M, mixed group; NC, non-clinical control; O, obsessionals; OCD, obsessive–compulsive disorder; SOC, Stockings of Cambridge; SWM, spatial working memory; W, washers.
Means estimated at HDRS=5.26 and HARS=7.74.
†ANCOVA, significance set at p<0.01.
Discussion
This study examined the performance of different OCD subtypes on neuropsychological tasks. Consistent with many previous studies [47–49], four OCD subtypes were identified: washers, checkers, obsessionals, and a mixed symptom group. The OCD subtypes and NCs differed as expected on measures of symptoms. We compared the performance of the groups on executive function tasks, visual memory tasks, and an attentional set-shifting task that have previously distinguished OCD cohorts from control groups [2, 3]. The study found that washers differed least from NCs in their neuropsychological performance. In contrast, checkers exhibited significantly poorer performance compared to NCs on a range of tasks, including SWM, pattern recognition, and initial movement latency on a planning task. The checkers also exhibited significantly poorer performance compared to washers on pattern recognition. The obsessional subtype performed significantly more poorly than NCs on a spatial recognition task.
Overall, the current findings offer some support for subtype differences in neuropsychological performance, with checkers showing greater deficits relative to other subtypes in SWM and initial movement latency. Various deficits have also previously been found in patients with checking symptoms [24, 29–31], but the low magnitude of these subtype differences provides less support to the hypothesis that OCD subtypes form separate disorders, and is more supportive of the influence of specific phenotypic characteristics on neuropsychological performance. Also, the current study may not have been sufficiently powerful to detect similar patterns of deficits across all subtypes. Future studies with larger samples are needed to confirm the observed effects. In addition, such studies need to also include tasks that are relatively insensitive to frontal deficits (e.g. test of general intelligence such as the Verbal and Full Scale Wechsler Adult Intelligence Scale–Revised) to examine whether the patterns of deficits observed in a particular subtype (e.g. checking) indeed are differential deficits [50].
Intuitively, a relative incapacity to remember and organize information may lead to doubting and excessive checking. Recent studies, however, also indicate that not only does checking exacerbate doubts about memory [51], but it is also associated with impaired trait confidence in memory [52]. Poorer performance in OCD, relative to other groups, is particularly evident when patients have to rely on internal representations to guide their selection during neuropsychological performance [2]. Covert checking and poor meta-memory are particularly likely to interfere most with the capacity to generate and be guided by realistic internal representations.
Meta-memory is increasingly seen to be important in checking. Individuals with lower memory confidence feel the need to repeatedly check so as to ensure that situations are safe [51–55]. Checkers may experience particular interference on tasks on which confidence is an important influence (e.g. initial movement latencies on the SOC). Lowered confidence in their internal representations of the world, particularly with respect to novel or ambiguous information (e.g. spatial), could lead to a greater reliance by checkers on external validation [2]. This could account for the relatively poor performance of checkers on the SWM task, in which external validation of ongoing performance is not possible. Checkers exhibited a compromised ability to organize and develop strategies for the online management of spatial information, whereas they may do as well as non-clinical and other clinical controls on tasks that can be verbally mediated or those in which the ongoing performance of subjects can be externally validated [2]. Future studies should examine how task-relevant factors interact with symptomatic phenomena and meta-memory factors in influencing the performance of OCD subtypes on specific neuropsychological tasks.
A limitation of the present study was that the OCD cohort consisted mainly of medicated participants. Previous examination, however, of differences between medicated and non-medicated cohorts on the CANTAB have suggested that medication is unlikely to account for the present results [3, 56–58], with research suggesting that any differences are, at most, mild [57]. Moreover, in the present study there were no significant differences between the three OCD subtypes on medication status.
The present study has strengths, in that it ascertained that the subtypes exhibited the expected subtype-specific symptoms at the time of neuropsychological assessment, and used multiple assessors to ascertain subtype status. We also matched OCD subtype and NC cohorts on important covariates (e.g. premorbid verbal IQ, handedness, age) and no subtype differences were noted in the course of disorder or in mood variables. Indeed, given the relatively small sample sizes for each subtype, the fact that significant results were found was particularly notable. Nonetheless, replication in larger samples is required to establish the reliability of the present results.
If replicated, the findings of neuropsychological differences between OCD subtypes may have implications for psychological treatment of the disorder, such as cognitive behaviour therapy. The poorer SWM in the checking subtype might favour an increased use of verbally mediated interventions, rather than strategies relying on internal representations, such as imaginal exposure. Indeed, one of the strengths of cognitive behavioural therapy is its ability to structure and organize the experience of affected individuals.
Also, although some previous studies have examined treatment effects on neuropsychological performance in OCD cohorts [59], two studies that used the CANTAB conflict in terms of whether performance improved over and above a test–retest control group (Nedeljkovic M et al.: unpublished data, 2007) [57]. Future research examining the relative effects of treatment in particular OCD subtypes would further clarify the role of neuropsychological factors in the aetiology and maintenance of specific OCD symptoms.
Overall, the present study found specific differences between OCD subtypes on neuropsychological performance, with checkers generally found to exhibit greater deficits from NCs than did washers and obsessionals. The knowledge of differences between subtypes in terms of neuropsychological profiles may have implications for treatment. Future research, such as investigations taking into account interaction between psychological and neuropsychological factors, will need to account for methodological limitations when replicating the current findings.
Partial η2 for subtype groups relative to non-clinical controls (n=59)
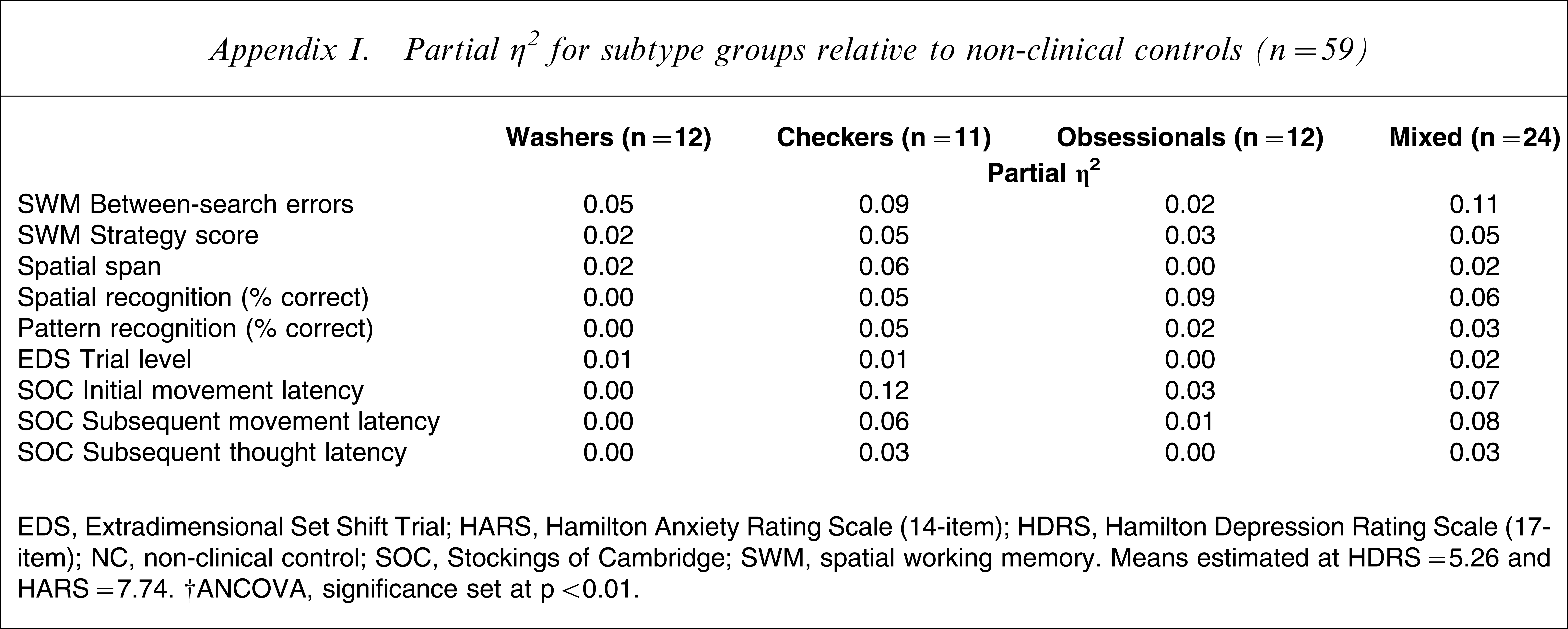
EDS, Extradimensional Set Shift Trial; HARS, Hamilton Anxiety Rating Scale (14-item); HDRS, Hamilton Depression Rating Scale (17-item); NC, non-clinical control; SOC, Stockings of Cambridge; SWM, spatial working memory.
Means estimated at HDRS=5.26 and HARS=7.74.
†ANCOVA, significance set at p<0.01.