
Abstract
For many years bipolar disorder was thought to be of low prevalence and invariably adequately treated by lithium. The past 15 years has seen a substantial shift in the view taken of this illness. Large-scale epidemiological surveys have indicated a lifetime prevalence of up to 4% [1]. Furthermore, it has become increasingly apparent that relapse rates and levels of inter-episodic symptoms are high, resulting in profound functional impairment and disruption in family, social and vocational aspects of individuals’ lives [2, 3].
The last decade has seen the establishment of large multi-centre clinical studies such as the Stanley Foundation Bipolar Network (SFBN) [4] and the Systematic Treatment Enhancement Program for Bipolar Disorder (STEP-BD) [5] in the USA. The SFBN operated in three US and one Dutch site [4], while STEP-BD collected information from an extensive network of US centres [5]. In addition to their focus on therapeutics in large and/or treatment-refractory bipolar disorder populations, these specialized clinical programmes, by virtue of their structure, generated an excellent opportunity to collect detailed data on large and heterogeneous samples, offering substantial statistical power for subgroup analysis and the flexibility to focus on issues of specific interest to the field. This contrasts with community survey methodologies through which limited numbers of bipolar disorder cases are ascertained, making detailed analysis difficult; and with traditional randomized clinical trials methodology that seeks sample homogeneity to maximize statistical power.
In studying clinical samples, especially those involving attendance at a clinic or programme, it is important to recognize that the population accessed is limited to those seeking treatment and, as with all methodologies, inherent referral biases exist. Unlike community surveys, the portion of the population with bipolar disorder is non-randomly selected in such samples. The clinical context, especially the means of access to the clinic or programme, plays an important role in the final sample composition.
This paper describes the first clinical cohort of an Australian specialist outpatient clinic – the Black Dog Institute Bipolar Disorders Clinic (BDI-BDC) – and compares this Australian dataset with (i) the predominantly outpatient SFBN and STEP-BD samples; (ii) findings from epidemiological studies; and (iii) the general Australian population. This report highlights the commonalities and distinctions between these samples. Because there have been few such large outpatient bipolar disorder samples described internationally, this comparison provides a rich source of definition of the characteristics of this condition in the (predominantly) outpatient setting. In this paper we focus on the sociodemographic and clinical features reported from all three samples.
Method
Background
The BDI-BDC was established in 2000. The data presented in this paper detail the first cohort of this clinical and research service. The clinic is ongoing. In addition to its research mission, the clinic provides comprehensive reviews and second opinions to the primary treating clinicians of patients who attend. Advice on diagnosis and management is informed by detailed assessment with multidisciplinary input. Initial appointment requests are made by patients, their relatives, general practitioners or psychiatrists, and a referral letter from a treating health professional is required prior to appointment. The clinic costs are fully covered by the Australian and New South Wales State public health systems, to which all residents are entitled.
The study has been approved by the Human Research Ethics Committee of the University of New South Wales. Patients who attend the clinic are invited to provide written consent to allow the data collected to be used for research purposes. All clinic attendees receive the same quality of clinical assessment and advice, irrespective of whether they agree to their details being used for research purposes. Patients are also invited to provide consent for blood samples and genotyping for research purposes.
Data collection
DSM-IV current and lifetime diagnoses of bipolar disorder were established employing the best estimate methodology of Leckman et al. [6] utilizing data obtained from the Diagnostic Interview for Genetic Studies (DIGS) [7], the Structured Clinical Interview for DSM-IV (SCID) [8], information gathered through a detailed structured interview developed for the clinic, and medical reports received from the referring medical practitioner. Both the SCID and DIGS are well-validated structured diagnostic interview schedules. The DIGS was used to enable data sharing and combined analyses with the large Sydney-based bipolar disorder molecular genetics study [9, 10], which consists of >1000 affected and non-affected family members. The DIGS also has the advantage of being able to derive Research Diagnostic Criteria, DSM-III and DSM-IIIR diagnoses.
Current symptom severity was assessed using the following standardized measures: the Bipolar Depression Rating Scale [11, 12]; the Montgomery and Åsberg Depression Rating Scale [13]; the Hamilton Depression Scale [14]; the Young Mania Rating Scale [15]; and the Mania Rating Scale from the Schedule for Affective Disorders and Schizophrenia [16].
The structured interview developed for the clinic consisted of >100 items, and was administered by the clinic research psychiatrists (PM and GM). This interview was devised to assess aspects of the patient's experience of bipolar illness not adequately captured in the other (standardized) instruments. It included a detailed section regarding the onset and course of illness. Patients were questioned regarding aspects of their illness profile such as the pattern of episodes and changes in frequency, duration and severity of elevated and depressive episodes. A treatment section detailed past and current pharmacotherapy, hospitalizations, the use of electroconvulsive therapy and psychological treatments. Further sections addressed interepisodic symptoms, early warning signs, clinical domains of functioning, family history of affective disorder, and comorbid disorders.
An objective rating of current functioning was made by the clinic research psychiatrists using the Global Assessment Scale [17]. Sociodemographic and physical health information was collected through a self-report questionnaire.
Inclusion criteria
Dataset inclusion criteria were limited to a DSM-IV diagnosis of bipolar disorder I, II or not otherwise specified (NOS) determined in an earlier section; the provision of informed written consent; and a current age of at least 18 years.
Statistical analysis
Analyses were conducted using SPSS, version 12 (SPSS, Chicago, IL, USA). Distributions of the sociodemographic and key clinical features were analysed. Measures of central tendency (mean, median) and of dispersion (SD) were run for continuous data. Categorical data was summarized by percentages. Comparisons were made with other clinical datasets, epidemiological surveys and the Australian general population (2001 Census [18]). These latter comparisons were purely observational and not quantitatively analysed.
Results
Of the 264 patients who attended the BDI-BDC in this cohort, 217 met the inclusion criteria. Seventeen per cent of patients who attended the clinic did not meet the diagnostic criteria and <1% declined consent for data to be used for research purposes. Of those who did not meet the diagnostic criteria, major depressive disorder was the most common diagnosis, accounting for 43% of non-bipolar disorder cases. Further non-bipolar disorder diagnoses of note were schizoaffective disorder (17.3%), schizophrenia (6.5%) and an anxiety disorder (10.8%). Of those included in the final dataset, 90% (196/217) met the DSM-IV diagnostic criteria for bipolar I disorder and 10% met criteria for bipolar II disorder.
Sociodemographic characteristics
Seventy-nine per cent of the BDI-BDC sample resided in Sydney and 96% within the State of New South Wales. Ninety-two per cent resided in metropolitan areas as classified by the Rural, Remote and Metropolitan Areas classification [19].
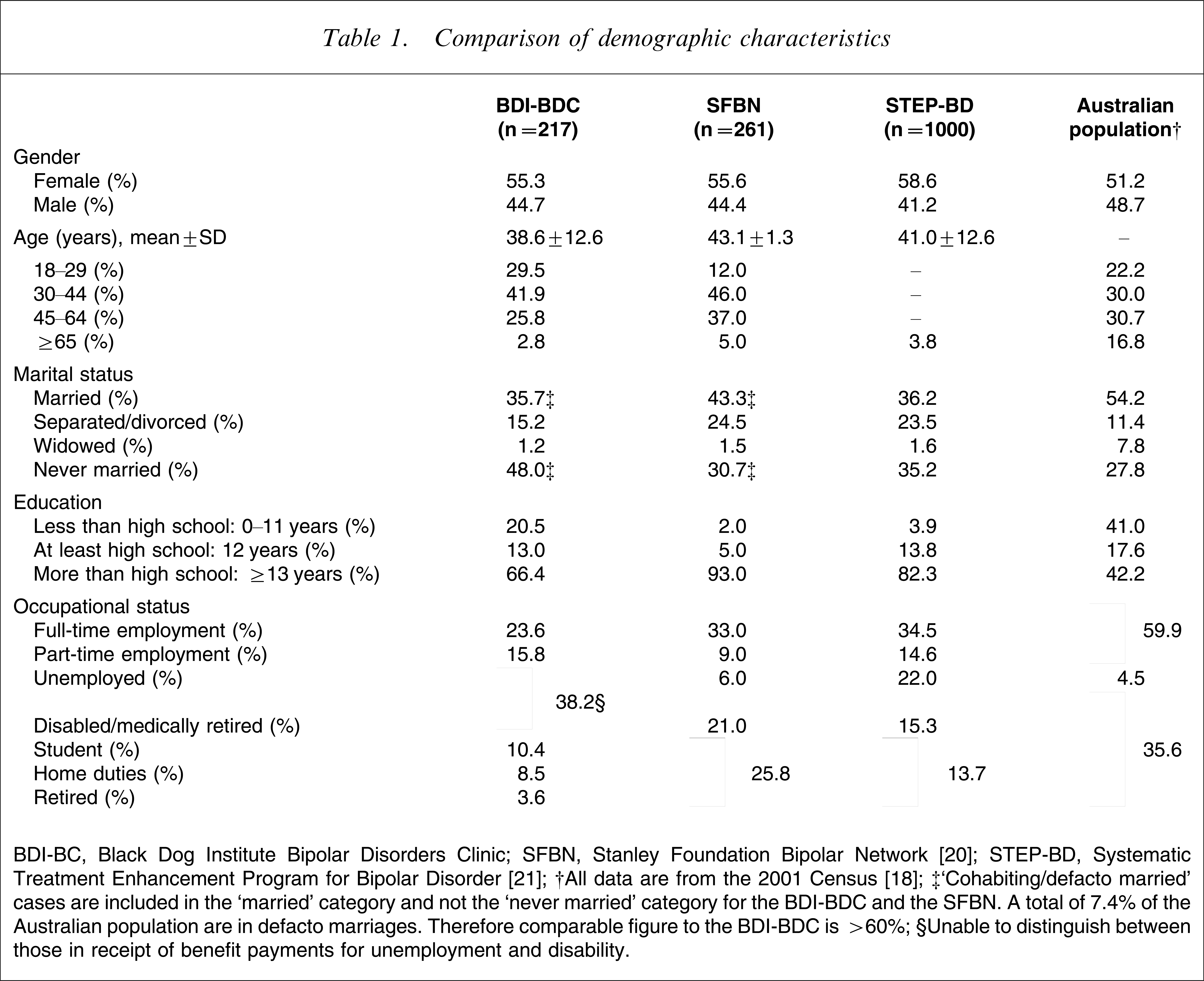
Table 1 presents the sociodemographic characteristics of the BDI-BDC sample in comparison with the SFBN and the STEP-BD populations. Table 1 also provides comparative figures for the Australian general population. Where relevant, differences in the distribution of characteristics between the Australian and US populations will be described in the text.
Comparison of demographic characteristics
BDI-BC, Black Dog Institute Bipolar Disorders Clinic; SFBN, Stanley Foundation Bipolar Network [20]; STEP-BD, Systematic Treatment Enhancement Program for Bipolar Disorder [21].
†All data are from the 2001 Census [18].
‡‘Cohabiting/defacto married’ cases are included in the ‘married’ category and not the ‘never married’ category for the BDI-BDC and the SFBN. A total of 7.4% of the Australian population are in defacto marriages. Therefore comparable figure to the BDI-BDC is >60%.
§Unable to distinguish between those in receipt of benefit payments for unemployment and disability.
Age and gender
Similar to the other samples, the BDI-BDC recruited a higher proportion of women compared to the Australian general population (55.3% vs 51.2%). The mean ages in the three clinical samples were all within a narrow range, between 38.6 years and 41.0 years. Compared to the Australian general population, the BDI-BDC had higher proportions of individuals in the 18–29 years and the 30–44 years age categories (7% and 12% higher, respectively), and a substantially smaller proportion of individuals in the ≥65 years age group. This pattern of overrepresentation in the lower age brackets and marked underrepresentation among those ≥65 years was also found in the STEP-BD sample. Twenty-one per cent of the STEP-BD population was in the 15–24 year age range, compared to 14% of the US population. In contrast to the other samples, the SFBN had a smaller proportion of individuals in the study's youngest age group compared to their local general population, 12% compared to 26%. This may reflect the bias towards treatment refractoriness in that latter sample.
Relationships
Lower rates of current marriage (or stable de facto relationships) and higher rates of marital disruption than in the local general population are evident across all clinical samples. It is to be noted in Table 1 that the true degree of disparity in marital status between the BDI-BDC and the Australian population is under-stated by a mismatch in data categorization. Of those in the BDI-BDC, 36% were in either registered or de facto marriages compared to >60% of the Australian population.
Education and employment
All three clinical samples were more highly educated than their local general populations. The SFBN represents the extreme, with 93% having some tertiary education and 2% having less than a high school education. The distribution of educational achievements in the BDI-BDC is more consistent with that of the local general population than that of the SFBN or the STEP-BD.
Overall levels of employment were lower in the BDI-BDC sample compared to the general Australian population, and full-time employment was lower in this clinic sample than in the SFBN and STEP-BD groups. Levels of unemployment and government disability support benefits were high in all the clinic samples. Thirty per cent of BDI-BDC patients reported being in receipt of disability benefits at the time of assessment.
Clinical characteristics
Diagnosis
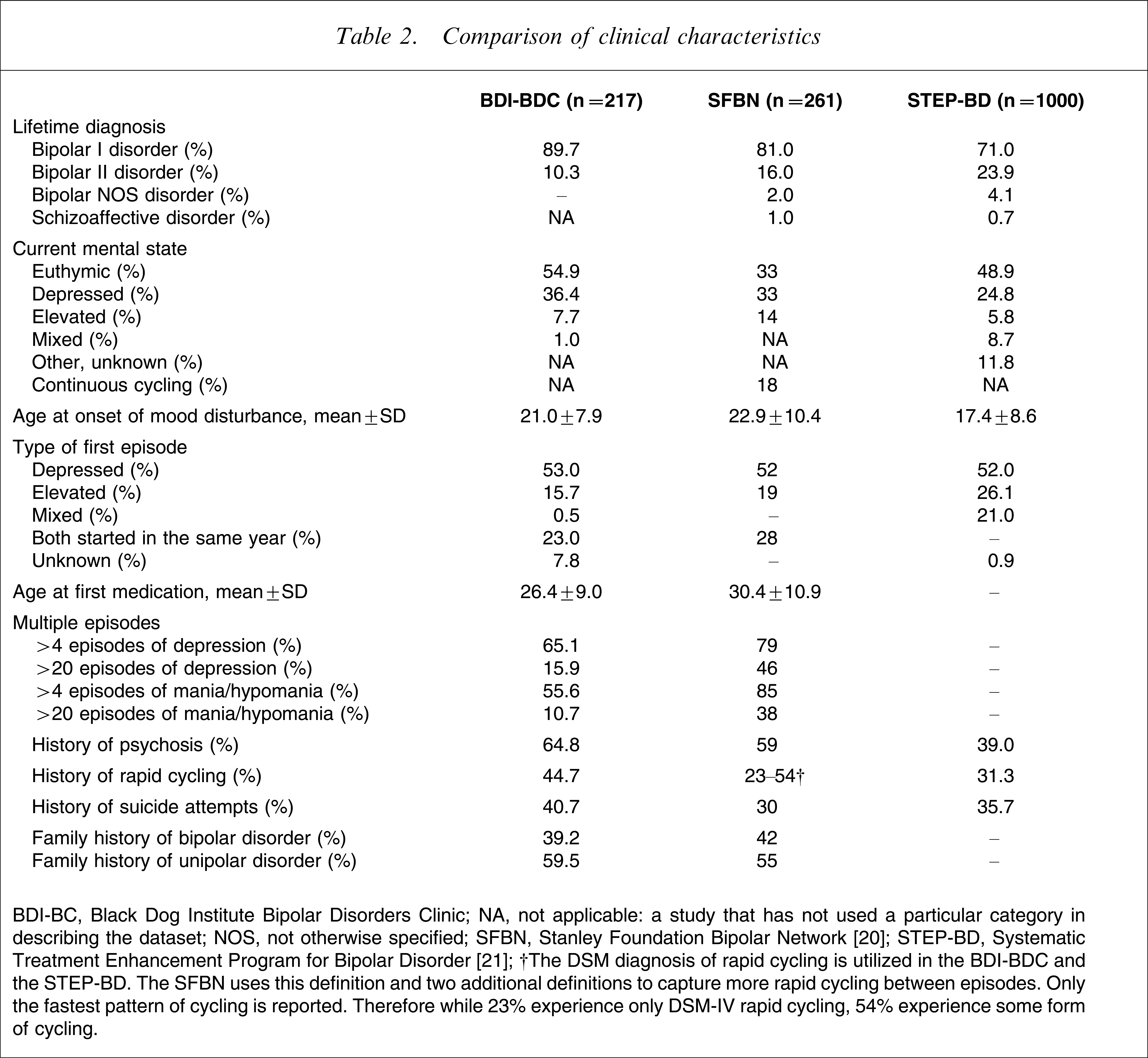
As detailed in Table 2, the majority of patients in all three samples were diagnosed with DSM-IV bipolar I disorder, with the BDI-BDC having the highest proportion (90%). The prevalence of bipolar II disorder ranged from 10% in the BDI-BDC to 24% in the STEP-BD; the diagnosis of bipolar NOS was uncommon. At the time of study entry, around half of the BDI-BDC and STEP-BD samples and one-third of the SFBN sample did not meet DSM-IV criteria for a current episode of mood disturbance. The majority of patients with an episode of mood disturbance meeting DSM-IV criteria were experiencing major depression.
Comparison of clinical characteristics
BDI-BC, Black Dog Institute Bipolar Disorders Clinic; NA, not applicable: a study that has not used a particular category in describing the dataset; NOS, not otherwise specified; SFBN, Stanley Foundation Bipolar Network [20]; STEP-BD, Systematic Treatment Enhancement Program for Bipolar Disorder [21].
†The DSM diagnosis of rapid cycling is utilized in the BDI-BDC and the STEP-BD. The SFBN uses this definition and two additional definitions to capture more rapid cycling between episodes. Only the fastest pattern of cycling is reported. Therefore while 23% experience only DSM-IV rapid cycling, 54% experience some form of cycling.
Age of onset of mood disorder
The BDI-BDC and the SFBN populations similarly reported the mean age of onset of first mood disturbance to be in the early 20s, while the STEP-BD reported mean onset in the late teens. The proportions of patients with an early onset of bipolar disorder (defined here as onset of significant mood disturbance prior to age 18 years) were also similar in the BDI-BDC and the SFBN samples: 38% and 31%, respectively. Just over half of all the three clinical samples reported depression as the first episode of mood disturbance. Due to data collection methods, however, in one-quarter of SFBN and BDI-BDC cases the mood type of first episode could not be established because the first depressed and elevated episodes occurred in the same year. Unipolar mania was rare; for example, only 1.6% of BDI-BDC subjects reported that they had never experienced an episode of depression.
Age at first treatment
The mean age at which BDI-BDC subjects first received psychotropic medication was slightly younger than that for the SFBN (mean 26.4 years vs 30.4 years). Furthermore, the mean delay between onset of mood disturbance and first receipt of psychotropic medication was almost twice as long in the SFBN compared to the BDI-BDC sample: 10.4±10.9 years compared to 5.8±7.9 years. It is of note, however, that for the BDI-BDC sample the median delay between first mood disturbance and medication was considerably shorter than the mean, being 2 years, suggesting a degree of distortion from outlier patients who had prolonged delays to initiation of treatment.
Age at diagnosis of bipolar disorder
Substantial delay also occurred between the first episode of elevated mood and the diagnosis of bipolar disorder. In the BDI-BDC sample, the median delay was 2±6.2 years, with 25% of patients not being diagnosed with bipolar disorder within 5 years of their first episode of elevated mood. Almost three-quarters of patients in both the BDI-BDC and in the SFBN reported one or more hospital admissions for mood disturbance, with almost 30% reporting five or more admissions.
Episode type and number
Greater numbers of both depressed and hypomanic/manic episodes were reported in the SFBN sample. The differences between the SFBN and the BDI-BDC populations were more pronounced for episodes of elevated mood than episodes of depressed mood, and in the proportions of patients reporting >20 episodes of each mood polarity. A high degree of variability in the number of episodes experienced by patients exists in BDI-BDC sample and, as is the case for many of the illness characteristics, the distributions are negatively skewed. Thus, while the mean number of episodes of depression was 14.0±20.2, the median was 7.5. The mean number of episodes of elevated mood was 11.2±19.4 and the median, 5.
Psychosis and rapid cycling
The proportion of subjects in each sample who reported experiencing psychotic features with episodes of mood disturbance at some stage of their life varied substantially across the three samples, from 39% in the STEP-BD to 65% in the BDI-BDC. These differing rates are consistent with the differing proportions of bipolar I and II disorder diagnoses. Rapid-cycling bipolar disorder, as defined by the DSM-IV criteria of four or more episodes of mood disturbance within 1 year, was more frequently identified in the BDI-BDC compared to the STEP-BD samples (45% vs 31%). Direct comparisons with the SFBN were not possible for this characteristic.
Suicide attempts
Reports of suicide attempts ranged from 30% to 40% across the three samples. Ninety per cent of BDI-BDC subjects with a history of suicide attempts reported them within the context of depressed mood. Only 10% reported attempts within a mixed mood context; attempts either between episodes or during elevated mood were rare.
Family history
Family histories of both bipolar disorder and unipolar depression were commonly reported by subjects in both the BDI-BDC and the SFBN samples. In both samples, around 40% reported a family history of bipolar disorder and >55% identified unipolar depression within their families.
Discussion
Despite data collection across three continents and the use of independently devised recruitment methods, the sociodemographic characteristics of the three samples were remarkably similar. Female gender and younger age were overrepresented compared to the general population. Functional impairment, indicated by marital status and labour force participation, was clearly more common among the study subjects than in the general population. In all three samples, prior educational attainment was higher than in the general population.
The BDI-BDC recruited a higher proportion of subjects with bipolar I disorder than the other centres. Despite the diagnostic differences in sample compositions, however, many of the clinical characteristics were broadly similar across the three samples, confirming commonality in many of the clinical features of bipolar disorder in the mainly outpatient setting, irrespective of the country under study. Approximately half of each sample was euthymic and approximately one-third was in a DSM-IV episode of depression at study entry. One-half reported depression as their first episode of mood disturbance. Similar proportions identified positive family histories of bipolar disorder (40%) and unipolar depression (55%).
Other clinical characteristics demonstrated more variation between the samples. The STEP-BD population reported an earlier age of onset. The SFBN subjects reported higher numbers of overall episodes, but psychotic features and suicide attempts were less common than in the BDI-BDC sample. These distinctions may reflect either differences in data collection methods or true differences in sample compositions in terms of age, diagnosis or severity of illness. These differences highlight the need to be aware of such sample characteristics when interpreting other findings (such as treatment outcome) in these large bipolar disorder samples.
While discussing age of onset in these samples, it is important to note that accuracy of recall of age of onset of any mental illness has been demonstrated to be poor when using standardized interview schedules. On average, studies have shown that respondents estimate onset as between 5 and 10 years prior to interview irrespective of current age [22]. This recall bias is sensitive to amelioration by methods that encourage the respondent to engage in more active and extensive memory search. For example, standardized age of onset distributions from the National Comorbidity Survey Replication (NCS-R), a survey that used such methods, reported a very wide range for age of onset of bipolar disorder, with a median age of 25 years [1].
Higher rates of psychosis, rapid cycling and suicide attempts among the BDI-BDC compared to the STEP-BD samples suggest a more severely ill patient profile in this Australian clinic population. This is consistent with the clinic context, with many patients being referred by their clinicians because of treatment resistance. Furthermore, the greater rates of psychotic symptoms are consistent with the higher prevalence of bipolar I disorder in the BDI-BDC sample [23].
Treatment seeking is high among individuals with bipolar disorder, with >90% obtaining treatment, albeit frequently with substantial delays after the onset of symptoms [24]. In the Australian National Survey of Mental Health and Wellbeing (NSMHW) among patients with any 12 month diagnosis of a mental health disorder, only 35% reported consulting a health professional in the previous 12 months [25]. The rate among those with bipolar disorder in that same survey, however, was 70%, with one-third specifically consulting a mental health professional [2]. In placing these three clinical samples (BDI-BDC, SFBN and STEP-BD) in context, it is important to bear in mind that all the respondents were treatment seeking and furthermore that they were assessed within specialist rather than routine health-care contexts. Consequently, it would be expected that the bipolar disorder populations captured by these methods should differ in terms of treatment-seeking behaviour from those identified by epidemiological surveys.
It is likely that the gender distribution within these clinical samples reflects gender differences in treatment-seeking behaviour rather true differences in the gender prevalence of bipolar disorder. Nationally representative surveys in the USA, the Netherlands and Australia have found no significant gender differences in the 12 month or lifetime prevalence of bipolar disorder [2, 26, 27]. It is of interest that the NCS-R reported some gender-specific differences, with longer delays and lower rates of treatment contact in male patients [23].
Treatment seeking is also related to education level, with those at higher levels being better equipped to seek out and access care [24, 28]. This bias to higher educational achievement is commonly found in these types of datasets [28]. Thus although higher levels of education are commonly found in clinical studies, US epidemiological surveys have found some evidence for a negative association between bipolar disorder and prior educational level [26, 29], and Dutch and Australian epidemiological surveys have found no associations between these characteristics [2].
Disability or functional impairment is also reported to influence treatment-seeking behaviour [28]. All three samples in the present study demonstrated high levels of marital disruption and unemployment. A significant relationship between marital disruption and bipolar disorder diagnosis was reported in the Australian NSMHW [2]. No significant associations, however, between bipolar disorder and unemployment have been identified in community samples [2, 27]. It would appear that, as Coryell et al. observed, impairment in relationships is associated with lower levels of illness severity than impairment in the employment domain; unemployment therefore is not sufficient to differentiate between treatment and non-treatment seekers [30].
Limitations
The primary limitation of this dataset has been explored in detail throughout this paper. As a clinic sample, it does not necessarily provide data representative of subjects with bipolar disorder in the community. All clinical study methodologies have this limitation to some degree. In contrast, survey methods, while arguably producing more representative datasets, are unable to capture sufficient numbers of bipolar disorder cases to allow for the calculation of precise estimates of specific features other than the broadest characteristics. Population survey methods are therefore equally limited and cannot be reliably used to produce an adequate descriptive base of clinical phenomenology.
In the BDI-BDC and other samples, both cross-sectional and longitudinal retrospective data have been collected. While retrospectively collected data are subject to criticism due to problems of recall bias, we would argue that these are somewhat ameliorated by the clinic context. Cognitive psychologists, in their studies of the organization of information in memory and retrieval strategies, have shown that experiences that are recent, distinctive, salient or unique are more easily remembered [31]. The challenge of dates in particular can be aided by charting experiences in relation to other more salient life events [32]. Therefore, in the BDI-BDC (as in other samples) patients were frequently asked to focus upon their worst ever episode of depression, mania or hypomania when providing information on symptomatology. Furthermore, these more challenging recall tasks were contained in the structured clinician-administered questionnaire, which followed a detailed comprehensive unstructured clinical interview. During the clinical interview the patient was encouraged to map out the course of their illness and chart this against major life events.
Conclusions
The present report highlights the marked commonalities of the sociodemographic and clinical characteristics of patients with bipolar disorder recruited predominantly from outpatient settings across three different continents: Australia, North America and Europe. It also demonstrates some critical distinctions between such samples, emphasizing the need to be aware of these when interpreting findings, such as naturalistic and treatment outcome, from different bipolar disorder datasets.
Footnotes
Acknowledgements
This research was enabled by funding from the Australian NHMRC Programme Grant for Depression and Bipolar Disorder No. 510135.