
Abstract
New Zealand population data indicate an increase in substance use among youth in New Zealand since the mid-1980s [1], with alcohol, cannabis and nicotine reported as the three most commonly used substances [2]. Official statistics show that 79% of 14–17-year-olds in New Zealand have consumed alcohol before the age of 15 years, while 10–15% have tried cannabis at least once by the age of 15 years [2].
Associated with high rates of substance use are relatively high rates of substance use problems. The Dunedin Multidisciplinary Health and Development Study has found that 10% of participants had a diagnosis of alcohol dependence at 18 years and 5% had a diagnosis of cannabis dependence [3]. The Christchurch Health and Development Study (CHDS) similarly found that 24% of young people met the criteria for a diagnosis of alcohol or cannabis dependence by 18 years of age [4]. The CHDS also found high rates of coexisting disorders among young people with substance use problems. As many as 30% of the study cohort aged between 16 and 18 years met criteria for a substance use disorder with coexisting mood, anxiety or conduct disorder [4].
Although there are no published New Zealand data, international research indicates that rates of comorbidity among adolescents in alcohol and other drug (AOD) treatment vary between 40% and 90% [5–8]. Despite the large number of young people with significant mental health and substance misuse issues, treatment seeking among this population is not high, reported as <10% in the CHDS [4].
Although these data suggest that only a small number of youth with mental health and addiction issues present for treatment, very little is known about the type of youth who do attend AOD treatment in New Zealand. It is arguable that knowledge of the characteristics of the young people who currently use AOD treatment services may assist not only in promoting treatment services for existing users but also in identifying groups of young people who are not accessing services. Such information would be useful in establishing strategies to target these groups and to develop services that might meet their particular needs.
The current study addresses this issue by providing data from a randomized sample of young people who attended one of eight youth AOD treatment services in New Zealand during 2003–2004.
Methods
Participants
Participants included in the present analysis were drawn from a study designed to examine factors associated with youth retention in a range of youth-specific AOD treatment settings in Aotearoa, New Zealand. Participants were eligible for inclusion in the present study if they had attended one of eight youth-specific AOD services selected to take part in this study during 2003 or 2004. These eight services were selected from a possible 11 services in New Zealand that met the criteria of being either a youth-specific AOD treatment service, an AOD treatment service with a youth-specific stream, or a general youth mental health service with an AOD treatment stream. Each type of service was also required to have at least three staff members. These eight services were chosen because they provided sufficient geographical spread and adequate ethnic representation of New Zealand youth. These services included two mainstream day and residential services (therapeutic communities), one mainstream outpatient service (harm reduction), one Pacific outpatient service (harm reduction), one kaupapa Māori outpatient service (harm reduction) and two kaupapa Māori residential services (abstinence based). The services were situated in Auckland, Hamilton, Hawkes Bay and Christchurch, New Zealand.
Using a computer-generated formula participants were randomly selected from a total pool of 660 possible participants. It was calculated that with a total sample size of 140 participants, there would be 80% power to detect effect sizes >0.5 between split subsamples. During recruitment, contact attempts were made with 433 of the 660 possible participants in random order. Of these 433 participants, 79 (18.2%) were recruited to take part in the study. Of the remaining pool 313 possible participants (72.3%) were not able to be contacted despite extensive efforts and 41 (9.5%) were able to be contacted but declined to be interviewed. Given the low rate of successful recruitment ethics permission was further sought to conduct confidential file searches for a selection of the non-participant group. In this way a participant group (n = 79) and a non-participant group (n = 105) combined to form the sample (n = 184) reported on in this paper. Participants and non-participants were shown to be similar across most variables, but non-participants were more likely to have had a diagnosis of conduct disorder at treatment entry (p < 0.01) and participants were more likely to have been diagnosed with a substance use disorder only at treatment entry (p = 0.01).
For reasons of privacy, recruitment and non-participant file searches were conducted by a trained staff member (either administrative or clinical) within each treatment service. Participant file searches were conducted by researchers from the National Addiction Centre or trained interviewers from each treatment service. File searches provided information on sociodemographic and clinical details at the time of treatment entry including age, gender, ethnicity, living circumstances, substance use diagnosis, mental health diagnosis, source of referral, treatment duration, the presence or absence of criminal convictions and time spent in correctional facilities or under the care of Child, Youth and Family Services (CYFS).
Statistical analysis
Data were entered into SPSS 13.0 (SPSS, Chicago, IL, USA), from which descriptive and comparative summaries were generated. χ2 tests for independence, Fisher's exact tests and Spearman's rank order correlation were performed to explore relationships between independent variables and treatment modality. Statistical significance was inferred for p < 0.05.
Results
Sociodemographic profile
Sociodemographic characteristics of the full sample when they entered AOD treatment in 2003–2004 are shown in Table 1. Patients attending treatment ranged in age from 13 to 20 years (median = 16.1 years). Male subjects were significantly older when they entered treatment than female subjects (16.4 and 15.6 years respectively, p < 0.01). The majority of patients were male (62.0%) and represented three main ethnic groups: European (51.1%), Māori (37.0%) and Pacific (8.2%). On entering treatment most patients were living with family members (76.5%). No significant gender differences were found for ethnicity or living circumstances.
Young people attending AOD treatment in New Zealand in 2003/2004: treatment entry
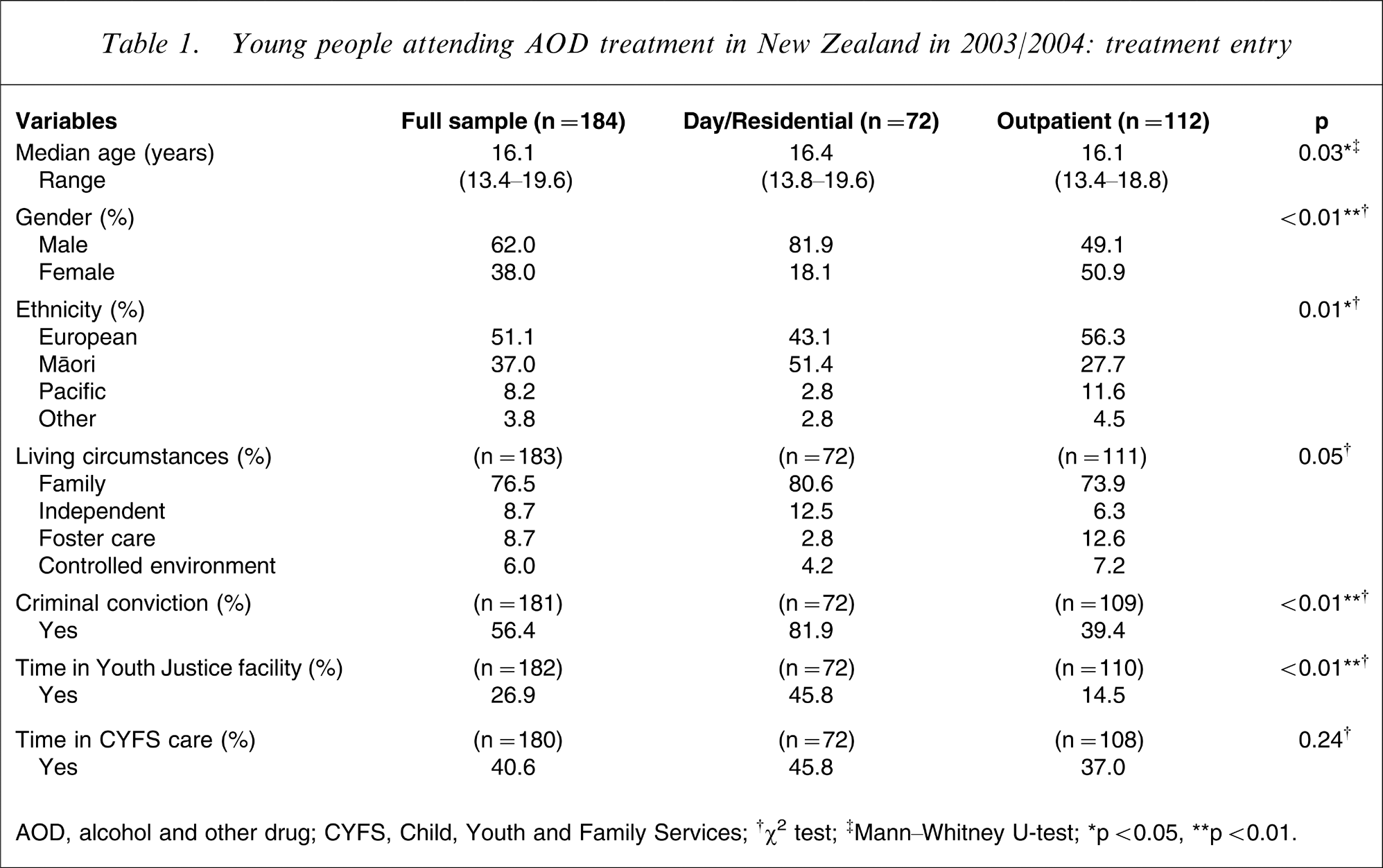
AOD, alcohol and other drug; CYFS, Child, Youth and Family Services;
High rates of criminal offending were apparent among this sample, with more than half (56.4%) reported to have had a criminal conviction prior to entering treatment. Significantly more male (71.2%) than female subjects (32.9%) had been convicted of a crime (p < 0.05). Forty per cent of the sample had spent time in the care of the CYFS with no significant gender differences found in this regard.
There were a number of differences found between treatment modalities. Youth attending outpatient services were significantly younger when they entered treatment (median age = 16.1 years) than youth attending day/residential treatment services (median age = 16.4 years). Significantly more male subjects attended day/residential services (81.9%) than outpatient services (49.1%). This reflected an overall gender difference within treatment services, where the majority of participants attending day/residential services were male, while male and female subjects were represented equally in outpatient services (49.1% and 50.9%, respectively). Youth attending day/residential services were also more likely than youth attending outpatient services to have been convicted of a crime (81.9% vs 39.4%) and to have been incarcerated for their offending (45.8% vs 14.5%). No significant differences were found in the numbers of youth who had been under the care of CYFS.
Substance dependence and psychiatric profile
A number of treatment services did not record information related to substance dependence and coexisting psychiatric conditions as part of their routine file data. In all, 57.1% of treatment files had no record of an individual's nicotine use, 38.6% had no record of an individual's alcohol dependence status and 33.2% of files had no record of an individual's cannabis dependence status. Files were classified as having no diagnostic information if regular use of a particular substance had been reported (i.e. >10 times) but results of diagnostic assessment had not been reported. Using this definition, it is possible that criteria for dependence or abuse were not met for a particular substance and therefore not recorded. It is also possible, however, that an individual might have met criteria for abuse or dependence on a particular substance but a specific assessment was not made and so this was not reported. Researcher feedback indicated that lack of assessment, rather than lack of reporting, was the main reason that substance use diagnoses were not made.
Lack of reporting of substance dependence was significantly greater among outpatient treatment services than day/residential treatment services.
Table 2 presents rates of substance use diagnoses among those treatment attendees for whom a record of substance dependence status was kept.
Substance use diagnoses among young people attending AOD treatment in New Zealand in 2003/2004 for whom substance dependence status was recorded
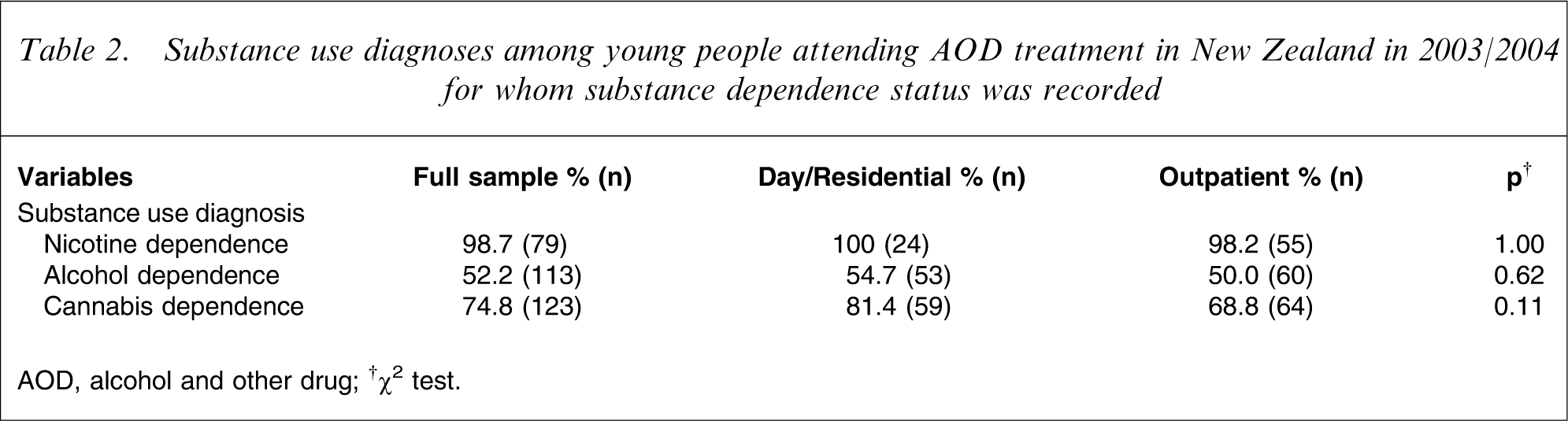
AOD, alcohol and other drug;
Rates of substance dependence recorded at treatment entry varied according to substance type, with the majority of participants presenting with a diagnosis of nicotine dependence (98.7%), cannabis dependence (74.8%) and alcohol dependence (52.2%). There were no significant gender differences or differences between treatment modalities found.
The mental health diagnoses listed in Table 3 reflect the four main mental health diagnoses reported at treatment entry in participant files. Conduct disorder was the most common diagnosis reported (37.5%), with significantly more youth attending day/residential services being diagnosed with conduct disorder (48.6%) than those attending outpatient services (30.4%, p < 0.05). No differences were found between treatment modalities for recorded diagnoses of depression (23.0%), attention-deficit–hyperactivity disorder (ADHD; 14.1%) and panic disorder (1.6%). High levels of comorbidity were also noted among this sample, with 53.8% of participants presenting with at least one substance use disorder and one mental health disorder. One-fifth (20.1%) of participants, however, were not diagnosed with any mental health or substance use disorder when they entered treatment. This high proportion of ‘no diagnoses’ and the low rate of reported anxiety disorders among this population is likely to be an artefact of the poor assessment and recording practices mentioned earlier.
Psychiatric profile at treatment entry of young people attending AOD treatment in New Zealand during 2003/2004
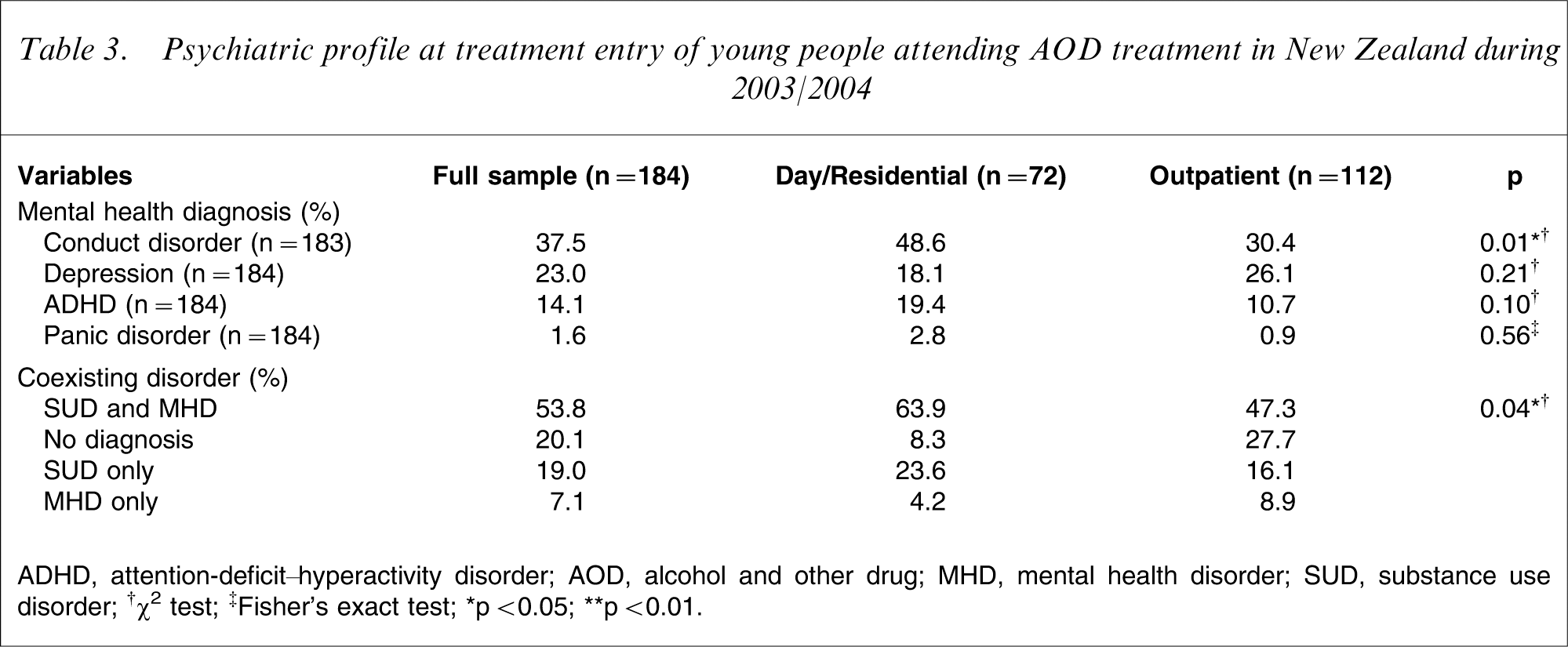
ADHD, attention-deficit–hyperactivity disorder; AOD, alcohol and other drug; MHD, mental health disorder; SUD, substance use disorder;
Gender differences were noted between internalizing and externalizing disorders. Significantly more female than male subjects were diagnosed with depression (37.7% and 14.0%, respectively, p < 0.01) and significantly more male than female subjects were diagnosed with conduct disorder (51.8% and 14.3%, respectively, p < 0.01) and ADHD (21.9% and 1.4%, respectively, p < 0.01).
Treatment profile
The majority of young people attending AOD treatment were referred from sources classified as ‘other’ such as education, health and family (68.3%), and almost one-quarter were mandated to treatment by the justice/court system (24.0%). Very few young people (7.7%) had self-referred to treatment. There were no significant differences between treatment modalities in this regard.
One hundred and twelve young people (60.9%) attended outpatient treatment, and 72 (39.1) attended day or residential services. In order to allow for comparison between treatment modalities in terms of treatment length, an ‘early dropout’ variable was created. Early dropout was defined as leaving outpatient treatment before the third session and leaving day/residential treatment within the first month of treatment. These criteria were based on those commonly used in clinical practice. These cut-offs fall well below the median stay of 3.4 months in day/residential treatment and 6.4 sessions in outpatient treatment, and as such indicate a group of young people who drop out of treatment well before the average patient. Across both treatment modalities 22.3% of patients dropped out of treatment early. No differences between treatment modalities were noted.
Differences between modalities were, however, noted in the reasons that patients were discharged from treatment. While approximately half of all patients (51.1%) were discharged for reasons that were conducive to treatment (i.e. completed treatment, met court conditions, returned to school, found a job etc.), significantly more youth attending day/residential treatment were discharged for reasons that were not considered to be conducive to treatment such as disciplinary reasons and self-discharge without staff recommendation (61.1% vs 39.3%, respectively).
No significant gender differences were found for any of the treatment profile variables.
Discussion
Of greatest importance in this study is the finding that regardless of treatment modality, young people who present to AOD treatment in Aotearoa, New Zealand bring with them a range of complex needs, particularly substance use and mental health issues, educational issues and criminality. Male and female subjects were found to present with different issues in relation to age, psychiatric comorbidity and criminality. The extent to which staff skills are adequate in order to respond to the complexity and diversity of the treatment needs with which youth present at AOD services is an issue that requires further attention.
The present findings highlight the importance of reflecting on service modality and utilization. An obvious gap in service utilization was seen in respect to the lack of female youth who attended day and residential treatment services. Despite an increasing rate of substance use being identified among New Zealand female youth [9] and despite approximately equal numbers of male and female participants attending outpatient services, young women appear not to be utilizing residential treatment services. It is likely that this can, in part, be attributed to a lack of treatment services providing suitable residential accommodation for young women. In New Zealand to date there are no female-specific youth AOD residential programmes, and those residential programmes that do offer spaces for female subjects have only restricted placements available for young women. Anecdotally at least, there is much frustration expressed by referring agencies at the lack of residential beds available for young women. This is an issue that requires immediate attention at both a service provider and funding level.
Concerns about adequate funding and staff competencies (attitudes, knowledge and skills) emerge from the underreporting of mental health and substance use diagnoses on treatment files. Despite more than half of the young people in the present study being diagnosed with at least one comorbid mental health and substance use disorder, the high rate of non-reporting of substance dependence and the high number of young people with no reported diagnosis, suggests that the rates of mental health and substance dependence calculated for this sample could be considerably lower than the actual levels of substance dependence present among youth attending these services. Although it is beyond the scope of the present study to ascertain how and why this issue arises, it is evident that such underreporting may have serious negative consequences for youth entering AOD treatment services in New Zealand. Sterling and Weisner, who noted discrepancies between file reports of psychiatric diagnosis and self-reported measures of youth self-report, suggested that this discrepancy arises out of the hesitancy by some providers to record psychiatric diagnoses, particularly for lower severity cases, resulting in less psychiatric intervention for these young people, which may impact negatively on their treatment outcomes [7].
Issues around treatment retention were also identified in the present study, with approximately one-quarter of young people attending AOD treatment dropping out of treatment early and shorter median lengths of stay being reported than expected for optimal treatment outcomes [10]. In addition, nearly half (47.8%) of all young people who attended these AOD treatment services in New Zealand were discharged for reasons that were deemed not conducive to treatment. This is a concerning statistic that raises some serious questions about the suitability of youth AOD services to fully address the needs of the young people who attend them. Although further investigation is required to more fully delineate specific reasons for this type of discharge, the high number of discharges based on disciplinary grounds leads one to contemplate the role that a change in service structure, to allow a more youth-friendly environment, might play in alleviating some of these issues. Harrison and Asche remarked that adolescent services are traditionally modified adult services and are, therefore, unlikely to be able to deal with the complexity of problems faced by adolescents [11].
Services that more realistically convey a true youth service would need to reflect a positive youth development model and take a systemic approach, thereby acknowledging the uniqueness of each individual as well as the multiple systems he or she is engaged with [12–16]. Such an approach focuses on dealing holistically with a young person's needs within a developmental context, and on engaging a youth participation approach that allows young people to be active in the development, management and running of a service and allows individual clients within the service to be active in the development and management of their individual treatment plan.
Limitations
There are several limitations. First, these data were collected from existing treatment files. Because of missing data, especially with regard to reports of mental health and substance use diagnoses, it is likely that the profile described underrepresents a number of the issues faced by young people entering treatment services. Most importantly, it is likely that an underestimate of the comorbidity issues faced by young people entering AOD treatment is presented in this paper.
Second, the services included in the present study were neither a randomized sample nor an exhaustive selection of all possible AOD treatment services available to youth in New Zealand. The findings, therefore, should be viewed as a broad snapshot rather than a definitive profile of youth attending AOD treatment in New Zealand. The present study, however, provides a first, and therefore, unique profile of young people who enter AOD treatment services in Aotearoa, New Zealand, thereby establishing a platform for further research, not only for improving the quality of the data but, moreover, in improving the quality of treatment provided.
Footnotes
Acknowledgements
Funding for this study was provided by the Alcohol Advisory Council of New Zealand (ALAC).