
Abstract
Mental illness, drug and alcohol use and personality disorders are major problems affecting prisoner populations [1–3], and are all risk factors for increased criminal recidivism, particularly violent and sexual offences [4]. Compared with community samples, prisoners have reported higher rates of anxiety (12 month prevalence rate of 38%, compared to 13%), affective disorders (46% and 10%, respectively) and substance use disorders (66% and 10%) [5]. Despite the high prevalence of psychiatric disturbance among prisoner populations, few studies have examined psychopathology in terms of temperament and character traits, and none have used the Temperament Character Inventory (TCI) to explore the relationship between substance use, depression and anxiety. As such, the aim of the present study was to assess whether TCI scores could be used to identify predictors of depression and anxiety and patterns of substance use.
Although personality can be described utilizing a dimensional or categorical approach, there is strong criticism towards categorical approaches. It is more likely that personality traits lie on a spectrum and that the boundaries between what is normal and abnormal is, at best, viewed as a blurred line or a ‘patch’ [6]. Dimensional approaches, such as Cloninger's psychobiological model of personality, place personality on a spectrum allowing for a gradation of trait expression. This model uses the TCI to derive four temperament and three character dimensions. Cloninger's theory specifies four temperament dimensions (novelty seeking (NS), harm avoidance (HA), reward dependence (RD), and persistence (PS)) and three character dimensions (self-directedness (SD), cooperativeness (CO), and self-transcendence (ST)). While Cloninger initially hypothesized that temperament factors are linked to specific genes and that character traits reflected learned behaviours [7], recent research has suggested that all dimensions are pleiotropic expressions of the same gene, but that while temperament traits develop early in life, character traits continue to be influenced by the environment well into adulthood [8]. The TCI has been validated in both clinical [6] and non-clinical samples [9], [10] as a measure of personality traits.
The associations between temperament factors, mood disturbance and anxiety disorders have been extensively studied [11–14]. High NS has been found to be critical in the development of suicidality [12]; high HA has been associated with symptoms characteristic of non-melancholic depression (i.e. individuals who are less likely to experience vegetative symptoms) [12], and low SD has been associated with symptoms of both anxiety [13] and depression [11], as well as being associated with a higher probability of being diagnosed with a personality disorder [15]. Furthermore, when combined with high PS, low SD has been shown to be associated with restless sleep and subjective symptoms of depression [12]. These findings suggest that temperament not only affects an individual's susceptibility to symptoms of depression and anxiety, but also the type of symptoms experienced.
Temperament factors have also been shown to play an influential role in substance misuse, affecting substance choice, severity of use, route of administration [16], and type of substance-use disorder [17]. The TCI has identified high NS, high impulsivity (a subgroup of NS), low HA [18], [19] and higher levels of ST [17], as the most salient variables that characterize heroin users. Others have used the TCI to demonstrate an association between high ‘shyness to strangers’ (a subdimension of HA) and moderate drinking [20]. Treatment compliance, which is often poor in substance misusers [21], may also be linked to temperament. For example, a person who is rating higher on the NS scale might disengage from a treatment programme before any benefit is evident because it is ‘too boring’. Additionally, both depression and anxiety have a negative impact on motivation. Therefore temperament and character, as well as depression and anxiety, could be considered to be important factors to take into consideration when designing treatment programmes and endeavouring to engage substance users in treatment [17].
In the present study we examined the relationship between temperament and character (measured by the TCI), substance misuse and the relationship that each has with depression and anxiety, with the aim of identifying characteristics that may have implications for treatment programmes for prisoners during and after their sentence. The findings are based on data from two large NSW surveys of prisoners’ mental health that incorporated the TCI as a measure of temperament
Method
Participants
The sample consisted of 1322 inmates who had completed all sections of the TCI as part of a screening programme to determine the mental health status of the State's prisoner population. The main findings have been described in detail elsewhere [22]. Participants were either part of a reception sample (n = 799) or had been sentenced (n = 523) and screened as part of the 2001 NSW Inmate Health Survey [22].
Reception prisoners consisted of those received into custody following a court appearance and screened within 24 h of admission. Male reception prisoners were mainly at the State's main reception centre in the Sydney metropolitan area or at three, smaller, non-metropolitan sites. All female prisoners were at the main women's reception centre in the Sydney metropolitan area. ‘Sentenced prisoners’ were those currently serving a prison sentence when recruited into the 2001 NSW Inmate Health Survey [2]. The overall response rate for the sentenced prisoners was 85% [2]. Participation in both studies was voluntary and confidential. All participants provided written consent and were informed that they could withdraw from the study if they wished to do so. Participants received $5 for participating in the surveys.
Assessment and measures
Interviews were undertaken by either Justice Health mental health nurses (reception prisoners) or by forensic psychology Masters students and Justice Health mental health nurses (sentenced prisoners). Participants were assessed with the same screening instrument used in the Australian National Survey of Mental Health and Wellbeing [23]. This consists of the Composite International Diagnostic Interview – Auto (CIDI-A) [24] with a range of other screening instruments (e.g. Kessler Psychological Distress Scale, a psychosis screener, General Health Questionnaire (GHQ) and Short Form 12 (SF-12) General Health Survey). The CIDI-A yields both DSM-IV and ICD-10 diagnoses. Substance use disorder, according to the CIDI-A, is categorized into opiate use disorder, sedative use disorder, and stimulant use disorder. Participants were classified into four groups of substance users based on ICD-10 diagnoses of substance use disorder: (i) no disorder; (ii) alcohol disordered (i.e. alcohol use disorder only); (iii) mono-disordered (i.e. one substance use disorder that was not alcohol related), and poly-disordered (i.e. more than one substance abuse disorder that was not alcohol related). They also completed the 144-item TCI [9].
Statistical analysis
The TCI scores were transformed to have a mean of zero and a standard deviation of 1, so that the seven dimensions could be compared. This did not change the relationship between the groups. Mean scores for drug-related variables were adjusted for age and sex (no differences were found when means were adjusted for affective, anxiety or psychotic disorders).
Logistic regression analyses were performed to identify factors that independently predicted inmates’ prevalence of (i) depressive and/or (ii) anxiety disorders. Sex, age, substance use and type of offence were selected for the first step of the model, with TCI dimensions being entered in the final stage of the model. Analysis of variance (ANOVA) was used to examine associations between inmate characteristics (sex, age, substance use, type of offence) and TCI scores. Tukey's honestly significant difference (HSD) test was used for post-hoc comparisons.
Results
Sample characteristics
At completion of the collection, 84% (n = 1104) of the sample were men, 34% were under 25, 48% were between 25 and 40 years and 18% were >40 years. Eighty per cent (n = 1062) of the sample were Australian born and 57% (n = 754) had not completed high school. ICD-10 diagnosis of major depression was made for 15% (n = 194) and for any anxiety disorder (post-traumatic stress disorder, agoraphobia, social phobia, generalized anxiety disorder, panic disorder, or obsessive–compulsive disorder), 35% (n = 467). Eighty-four per cent (n = 1112) of inmates were current tobacco smokers, of whom 98% classified themselves as ‘regular’ smokers. Overall, 54% (n = 714) had a 12 month ICD-10 diagnosis of a substance abuse disorder. Among those with a substance use disorder 14% (n = 97) were alcohol disordered only, 32% (n = 230) used one substance (i.e. mono-disordered), and 54% (n = 387) used two or more substances (i.e. poly-disordered). In the mono-disordered group, 54% (n = 124) had opioid use disorder, 23% (n = 52) stimulant use disorder, 20% (n = 47) cannabis use disorder and 4% (n = 8) sedative use disorder (not including tobacco use). Among those using multiple substances, 53% (n = 203) reported use of two substances, 23% (n = 88) reported three substances and 24% (n = 93) reported use of four substances.
In the past 12 months 43% had injected drugs, and 26% of all prisoners reported injecting drugs at some point in their time in prison. Drugs injected while in prison included heroin (83%), amphetamine/speed (47%) and cocaine (26%). Many of those who had injected drugs had taken more than one type of drug in the past 12 months (43% two drugs, 11% three drugs).
TCI scores by age and gender
ANOVAs were conducted to examine the impact of age and gender on the TCI scales. Statistically significant effects were found for NS for both sex (F(1310,1) = 6.8, p = 0.009) and the three pre-defined age groups (F(1310,2) = 13.7, p < 0.001). There was also a significant difference in CO scores when analysed by age (F(1310,2) = 14.1, p < 0.001 and gender (F(1310,1) = 13.5, p < 0.001). Women had higher mean scores for the NS scale (74.3 for women, 58.3 for men), and CO scale (72.1 for women, 66.5 for men), and also reported significantly higher mean scores than men on the HA scale (66.2 vs 45.3, F(1310,1) = 11.7, p = 0.001) and ST scale (69.7 vs 48.4, F(1310,1) = 18.3, p < 0.001). Post-hoc comparisons using the Tukey HSD test indicated that the >40 age group recorded significantly higher CO score (F(1321,2) = 34.0, p < 0.001) and SD score (F(1321,2) = 16.9, p < 0.001), but significantly lower NS scores (F(1321,2) = 41.1, p < 0.001) than the two younger age groups.
TCI and type of drug use
Significant stepped trends between the different substance use groups were found across all TCI dimensions (Figure 1). The mean scores for NS were highest among the poly-disordered group, lower for the mono-disordered group, lower again for the alcohol only disordered group, and lowest for those with no substance use disorder. Similar stepped trends were shown for HA, which was lowest in the no substance use group, and highest in the poly-substance use group. RD, PS, CO and SD were lowest in the poly-disordered, compared to the no disorder group. The poly-disorders group reported higher mean ST scores compared to all other groups. Prisoners who had injected drugs during the past 12 months scored higher on NS and HA, and lower on PS, SD and CO, than non-injectors.
Temperament and Character Inventory (TCI) dimensions and substance use. CO, cooperativeness; HA, harm avoidance; NS, novelty seeking; PS, persistence; RD, reward dependence; SD, self-directedness; ST, self-transcendence. Mono, mono-disordered (i.e. one substance use disorder that was not alcohol related); Poly, poly-disordered (i.e. more than one substance abuse disorder that was not alcohol related).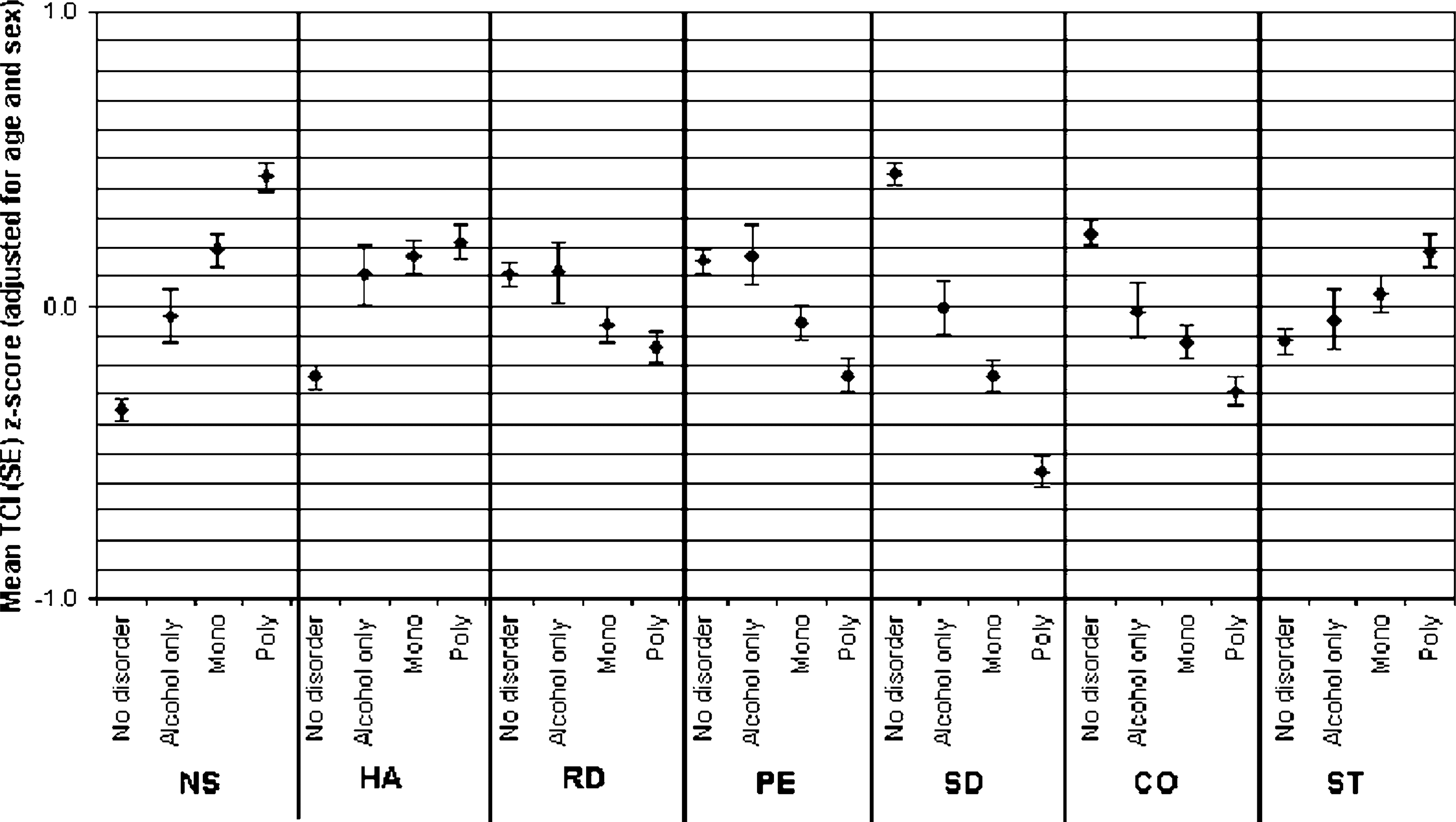
Inmate predictors of psychopathology
Logistic regression analyses were used to predict a 12 month history of depression and anxiety. Predictor variables included gender, age, substance use, and offence type, all entered before the TCI dimensions in a stepwise model. Offence type significantly predicted 12 month prevalence of depression, with sexual (odds ratio (OR) = 2.32, 95% confidence interval (CI) = 1.06–5.06, p = 0.035) and unspecified offenders (OR = 3.24, 95%CI = 1.44–7.29, p = 0.004) more likely to be depressed than violent and non-violent offenders.
The TCI dimensions that predicted depression history were high scores on the HA scale (OR = 1.02, 95%CI = 1.01–1.03, p < 0.001) and low SD (OR = 0.99, 95%CI = 0.97–0.99, p < 0.001). Being female (OR = 2.29, 95%CI = 1.59–3.28, p < 0.001) and a poly-substance user (OR = 2.12, 95%CI = 1.49–3.02, p < 0.001) predicted a 12 month prevalence of anxiety disorders. Older age (>40 years) reached a level of borderline significance (OR = 1.53, 95%CI = 1.00–2.36, p = 0.051) in predicting anxiety. No relationship was found between anxiety and the type of offence committed. The TCI dimensions that were associated with anxiety were higher HA (OR = 1.03, 95%CI = 1.02–1.04, p = 0.00), higher PS (OR = 1.02, 95%CI = 1.01–1.02, p < 0.001), lower SD (OR = 0.98, 95%CI = 0.97–0.99, p < 0.001) and higher ST (OR = 1.01, 95%CI = 0.99–1.01, p = 0.001).
Conclusions
The present results support previous findings on the relationship between temperament, anxiety [13] and depression [12]. Overall, the 12 month prevalence rates for depression (15%) and anxiety disorders (35%) were high compared with the general Australian community (11% and 9%, respectively) [5], but were in line with previous studies examining inmate populations [25], [26].
Female offenders reported higher mean scores for NS, HA, RD, CO, and ST, compared to male offenders. These findings are similar to those in the general population [27], [28], except for the higher NS scores female offenders [27]. It is postulated that high risk-taking and sensation-seeking traits in female offenders influence their engagement in available drug and alcohol intervention programmes.
A linear relationship was found between the number of drugs used and temperament/character dimensions, with poly- and non-substance users scoring on opposite extremes. Poly-substance users recorded significantly higher mean scores for NS, HA and ST and lower for RD, PS, SD and C. With regard to Cloninger's character traits, the more severe the substance use, the more likely that inmates will have character traits manifesting immaturity, self-destructiveness, irresponsibility, and an inability to define or pursue meaningful goals (SD); the less likely they are to be cooperative, empathic, compassionate, helpful and focused on others (CO); yet the more likely they are to show a greater intrinsic desire for self-actualization, creativity, and spirituality (ST) [17], [29]. These are character traits and thus potentially changeable and more amenable to intervention. Given the tendency for substance-misusing inmates to be less self-motivated to engage in rehabilitation, incorporating incentives that appeal to them prior to entering rehabilitation programmes might be beneficial, as well as assertive and continual assistance and encouragement to achieve treatment goals. Lower CO suggests that group settings might not be ideal for this population; and for the more severe substance users some form of individual work might be required.
The present findings are consistent with a previous report [30] that heroin-users rated more highly on ST than their alcoholic counterparts. In a substance abusing population, however, ‘spirituality’ may be linked to more severe psychopathology such as psychosis, but clear links have previously been drawn between ST and the broadened ideology of creative perspective and experience [31].
It is interesting to note that the inmate substance abusing group had higher HA scores than community samples of substance users [17], [29]. This suggests a possible partial explanation for the inmate population's vulnerability to engage in substance use. Having a desire to pursue novel and exciting situations (higher NS), but at the same time feeling anxious about such situations (higher HA), potentially creates conflicts. While this may illustrate separate aspects of drug use, it is also possible that these may be linked. It could be postulated that inmates with this temperamental make-up are at greater risk for substance misuse because they utilize substances to achieve the duel goal of enabling themselves to feel less anxious about pursuing stimulating, novel and exciting situation that they perceive as too risky when sober. With regard to this, it may be that being intoxicated removes the conflict (caused by high NS and HA) by reducing the expression of HA traits.
High HA and low SD scores were associated with depression and anxiety in the past 12 months, whereas those with anxiety disorders also had higher PS and ST scores. No association was found between low RD, elevated CO and depression or anxiety in the present study. SD has been shown to independently predict depression and anxiety, indicating that this character trait might be a vulnerability factor for negative affectivity [14]. Inmates who are depressed even in the absence of substance misuse require assertive encouragement in developing treatment goals and may benefit from approaches that promote activity, social integration and peer support [32], such as cognitive behavioural therapy and interpersonal therapy, rather than a pharmacological approach. The high prevalence rates of depression and anxiety disorders are often complicated by substance use in this population and standard single-focus treatment approaches may not be valid. We recommend tailoring of treatment programmes for individuals, respecting their psychiatric history and temperamental style.
It is, perhaps, unsurprising that the smoking rates within substance using inmates were almost at 100%. High prevalence rates of smoking among marginalized populations, including inmates, have been reported previously [33], [34], with i.v. drug users having the highest use [Belcher J et al.: unpubl. obs., 2006]. Despite these high prevalence rates many smoking offenders express a desire to quit, yet this population has traditionally been neglected by smoking cessation campaigns [33]. Smoking has been considered to be the gateway to many other drugs, and is thought to contribute to the continued use and relapse of other drugs [35]. Addressing this issue in the context of the specified intervention is likely to have treatment implications for illicit drug use.
Limitations
Some researchers have suggested that health data collected from prisoners are inaccurate because inmates’ responses may be biased by social desirability and/or feelings of generalized distrust. These claims, however, have never been systematically verified, and others have reported that information obtained via self-report from inmates is valid [36]. The present findings on the prevalence of mental disorders (such as depression and anxiety disorders) are consistent with two previous studies using NSW inmates [22], as well as international studies [3], [37]. Recently, Richmond et al. used biochemical validation of self-reported tobacco abstinence and a medical record validation of hospital attendance, and self-reports were found to be accurate [38].
Another limitation of the present study was that no comparison group was available to determine if similar relationships existed between temperament, character, substance use, and psychopathology within the general population. Future research in this area is warranted.
Addressing substance use in an offender population is probably one of the most vital therapeutic interventions that could be pursued in a correctional setting if the aim is to reduce offending. Clinical and offender populations can differ not only in vulnerabilities to mental conditions but also in dimensions of temperament and character. Currently most drug treatment programmes in prison follow a ‘one size fits all’ approach, with little regard for personality. The present study suggests that temperament and character inventories may be useful to identify individuals most at risk, as well as to tailor treatment in both prison and post-release (community) treatment programmes to assure their suitability for certain individuals.
Footnotes
Acknowledgements
Nadine Smith for statistical analyses and preparation of tables. NSW Justice Health Mental Health Nursing Staff for data collection; particularly David Cain, Christine Muller, and Dale Owens. Lucinda Wedgwood is supported by programme 222708 and 510135 NSW Infrastructure Grants from the Centre of Mental Health, NSW Department of Mental Health. Ethics approval was independently granted by the NSW Justice Health (formerly Corrections Health Service), and the NSW Department of Corrective Service's Human Research and Ethics Committees.