
Abstract
Internationally over the past 25 years a number of studies have reported variations in access to mental health care, utilization of psychiatric services and treatment interventions between ethnic groups [1–6]. Several studies have specifically examined ethnic differences in the use of psychotropic treatments and in particular antipsychotics. Many of the early studies found antipsychotic doses and prescribing rates for high potency first-generation antipsychotics (FGAs) and injectable depot antipsychotics to be higher in ethnic minority groups [7–13]. With the introduction, however, of the second-generation antipsychotics (SGAs) and treatment guidelines that recommended these newer drugs to be used as first-line treatment in schizophrenia, racial disparities in access continued to be reported [14–20]. While most recent studies show that the prescribing gap between ethnic groups has reduced over the last decade as the SGAs have become the mainstay of schizophrenia treatment [21], [22], ongoing racial differences have been reported in clozapine prescribing, the gold-standard antipsychotic for treatment-resistant schizophrenia [21], [23], [24].
In New Zealand (NZ) there has been increasing concern about the inequalities in overall health outcomes, and about the mental health of Māori, the indigenous people who comprise approximately 15% of the population [25–29]. The situation is similar for Pacific people living in NZ who comprise approximately 6.5% of the population [25], [29]. The Asian population in NZ is rapidly growing (approx. 6.4% in 2001 [30]), and although Asian people overall have positive health outcomes compared to the NZ population, their lower use of health services (including mental health services) is of concern [31].
The NZ Mental Health Survey found a higher prevalence of mental disorders (excluding psychosis) in Māori and Pacific people in comparison to the general population of NZ [29], [32]. This was partly explained by sociodemographic differences, especially for Pacific people. Increased rates of admission to psychiatric units for Māori and Pacific compared to European subjects have also been reported and particularly for psychotic disorders [33–37]. Although there is significant interest at a national level, which is supported by government policy [38–40], in identifying and eliminating any disparities in mental health outcomes between ethnic groups, there is less information about community mental health care for serious mental illness (especially psychotic disorders such as schizophrenia) and a lack of information about access to pharmacological treatment of serious mental illness in the major ethnic groups making up the NZ population.
Antipsychotic medication is an integral part of the evidence-based treatment of schizophrenia. Australasian and other international clinical practice guidelines recommend that SGAs are used as first-line treatment and that clozapine is used as soon as treatment resistance is identified. Other prescribing recommendations for antipsychotics include using the lowest effective dose and limiting antipsychotic polypharmacy [41–47].
The National Mental Health Plan (1997) included an objective ‘to prescribe new antipsychotic medication to people who are newly presenting or who can benefit most from changing from older style antipsychotic medications (including those who currently suffer intolerable side effects)’ and specific funding was approved for this express purpose, based on the assumption that by 2001 the SGAs would be prescribed as first-line treatment for psychosis [39]. National under-prescribing of SGAs, however, was reported in a 1999 progress update on meeting the access targets set by the Ministry of Health [48]. Until 1999, prescribing clozapine, risperidone and olanzapine treatment had been limited because funding for patients living in the community was restricted to discretionary use from hospital budgets. Consequently, in an attempt to meet the access targets, these three medications became fully funded on the pharmaceutical schedule in 1999, with the addition of quetiapine in 2001.
The purpose of the present study was to compare antipsychotic prescribing practice over two time periods (4.5 years apart) in the four major ethnic groups receiving outpatient care for schizophrenia in the public mental health services of Auckland, New Zealand.
Methods
Antipsychotic prescribing was examined for adult outpatients attending community mental health services in Auckland on 31 March 2000 (T1), and 31 October 2004 (T2). Auckland has three public health services providing community mental health care for a resident population of 1.2 million people, of whom almost 800 000 are aged between 15 and 64 years (2001 NZ Census [30]). Auckland is the largest city in NZ and the resident adult population is ethnically diverse: 59% European, 10% Māori, 11% Pacific, 11% Asian and 9% ‘other’ peoples [49–51]. The ‘other’ group is made up of Middle Eastern, Latin American, and African ethnicities.
Data collection
Data were collected from the clinical file (both paper and electronic records) by trained researchers for adult outpatients treated with an antipsychotic. This included demographic information (gender, age, and ethnicity), diagnosis and antipsychotic prescribing patterns (type, administration route and dose). Ethnicity was collected as it was recorded in the patient's clinical file; but the way in which ethnicity information was recorded by health services changed over the 4.5 year study duration. At the time of the baseline audit, ethnicity information was usually self-identified and recorded in the initial assessment/admission process and not by any particular definition of ethnicity. By the time of the second audit, new mental health service assessments/admissions often allowed a number of ethnic groups to be self-selected/identified. In general, the study found that a single ethnic group was recorded in the clinical file, and when more than one was identified the researchers recorded only the first. When the ethnicity was unknown or when there was a discrepancy within the body of the case notes, the researchers attempted to clarify the information with case-workers.
The primary working diagnosis (DSM-IV) was recorded from the medical review completed closest to the audit date. These are usually undertaken on a 3 monthly basis to coincide with prescription requirements. The prescribing information was recorded from the medication chart and verified in the body of the clinical notes or with duplicate copies of the prescription wherever possible, as the treatment the prescriber intended the outpatient to be taking on the day of the audit. For the purposes of comparison, antipsychotic daily dose was converted into chlorpromazine equivalents (CPZe mg day−1) and is described elsewhere [52].
The baseline audit identified prescribing differences between ethnic groups for several explicit antipsychotic prescribing variables. Rates of antipsychotic monotherapy, SGA use, depot use, clozapine use and total antipsychotic daily dose were found to differ significantly between the four major ethnic groups comprising the outpatient population. Verbal and written feedback of aggregated findings with attention to best-practice treatment recommendations was provided to all three services primarily to prescribers, pharmacists and service managers [53]. (Two interim audits were also undertaken in two of the three services on an 18 month basis.) In October 2004 (4.5 years after the baseline audit) a final audit was undertaken in all three health services using the same data collection methods (T2). The study received approval from the Auckland Regional Ethics Committee.
Data analysis
Data were entered into an Access database and statistical analyses were conducted using SAS version 9.1 (SAS Institute Inc, Cary, NC, USA). Only those outpatients with a diagnosis of schizophrenia or schizoaffective disorder were included in the analysis. Logistic regression models were used to investigate differences in the proportion of patients prescribed antipsychotics in the major ethnic groups and in particular whether these differences changed over the two time periods. A comparable linear regression analysis was performed on the antipsychotic dose, which was log transformed for analysis to better satisfy assumptions of normality. Covariate adjusted rates and means with 95% confidence intervals from models that included age and sex are presented. The probability level required to demonstrate significance was set at 0.01 because of multiple analyses.
Results
There were a total of 4821 schizophrenia outpatients prescribed antipsychotic treatment over the two time points (T1 = 2285 at 31 March 2000, and T2 = 2536 at 31 October 2004). Those outpatients from the ‘other’ ethnic group and ‘unknown’ were excluded from further analyses because of their small sample sizes, leaving a study population of n = 2236 at T1 and n = 2536 at T2.
Table 1 shows the schizophrenia population at both time points for each of the four major ethnic groups. No difference in gender distribution between the four groups was found at T1 but at T2 the proportion of male patients was reduced in the Asian group. At both time points there was a significant difference in (i) age, with Māori the youngest, European the oldest and Pacific and Asian subjects in between; and (ii) psychiatric hospitalization rates, with Asian the lowest, then Pacific and Māori and European subjects highest. The difference in hospitalization rates is possibly a reflection of the new immigrants in New Zealand, especially Asian people.
Schizophrenia population according to ethnic group (n = 4742)
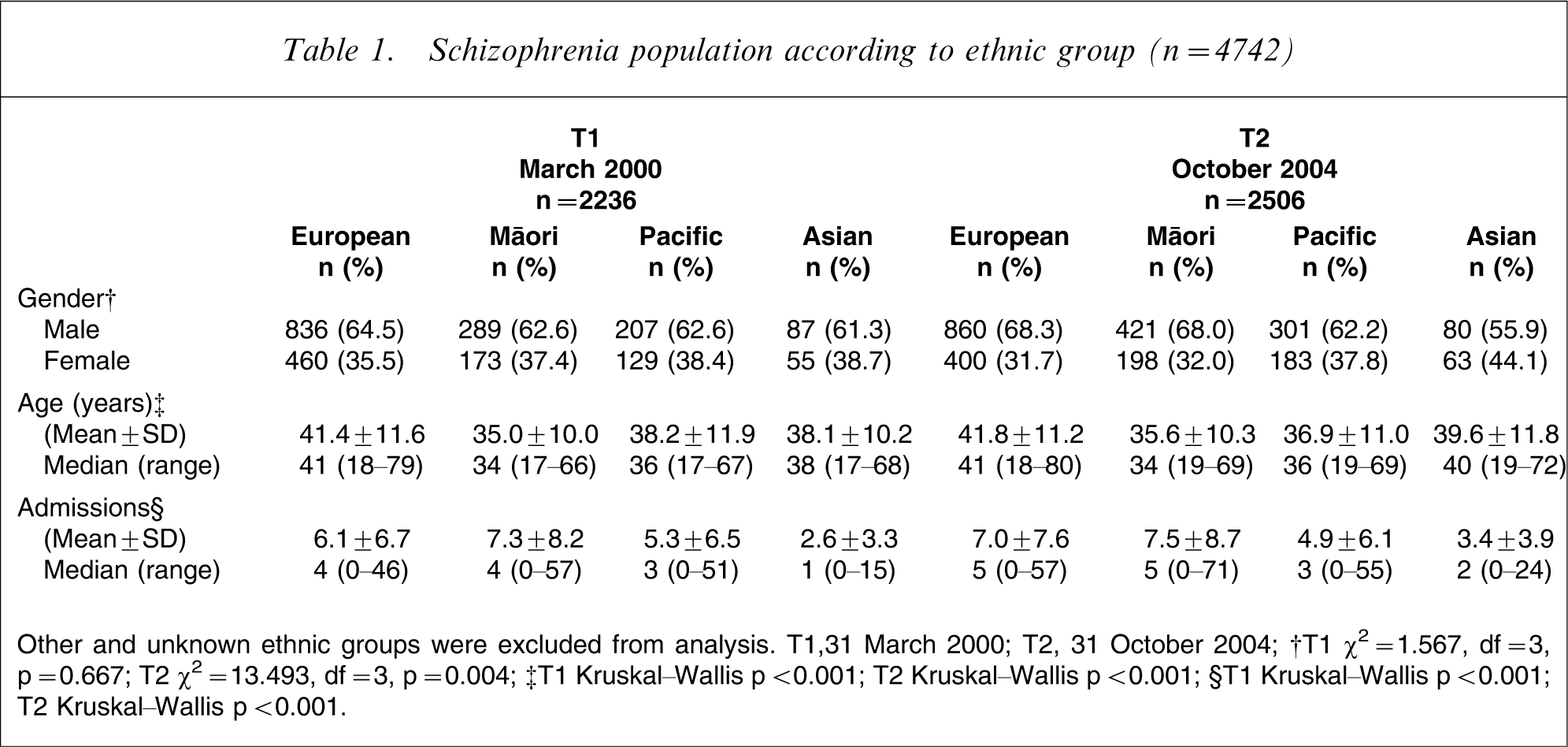
Other and unknown ethnic groups were excluded from analysis. T1,31 March 2000; T2, 31 October 2004; †T1 χ2=1.567, df = 3, p = 0.667; T2 χ2=13.493, df = 3, p = 0.004; ‡T1 Kruskal–Wallis p < 0.001; T2 Kruskal–Wallis p < 0.001; §T1 Kruskal–Wallis p < 0.001; T2 Kruskal–Wallis p < 0.001.
Antipsychotic monotherapy
At baseline there was a significant difference in the adjusted rates of antipsychotic monotherapy between ethnic groups (p = 0.002) (Table 2). The lowest rates were observed for Māori (73%) and highest for Asian subjects (84%). There was no statistical evidence of a difference in the change in monotherapy rates for the four ethnic groups over time (or the interaction effect between ethnicity and time) for either unadjusted or adjusted rates (Figure 1a). While all four ethnic groups had increased rates by the final audit, the change was small in most groups (European 5.1%; Pacific 3.3%; Asian 2.7%). The greatest change was for Māori subjects (12.2%), bringing the rates of antipsychotic monotherapy together for all four ethnic groups at T2 (p = 0.938).
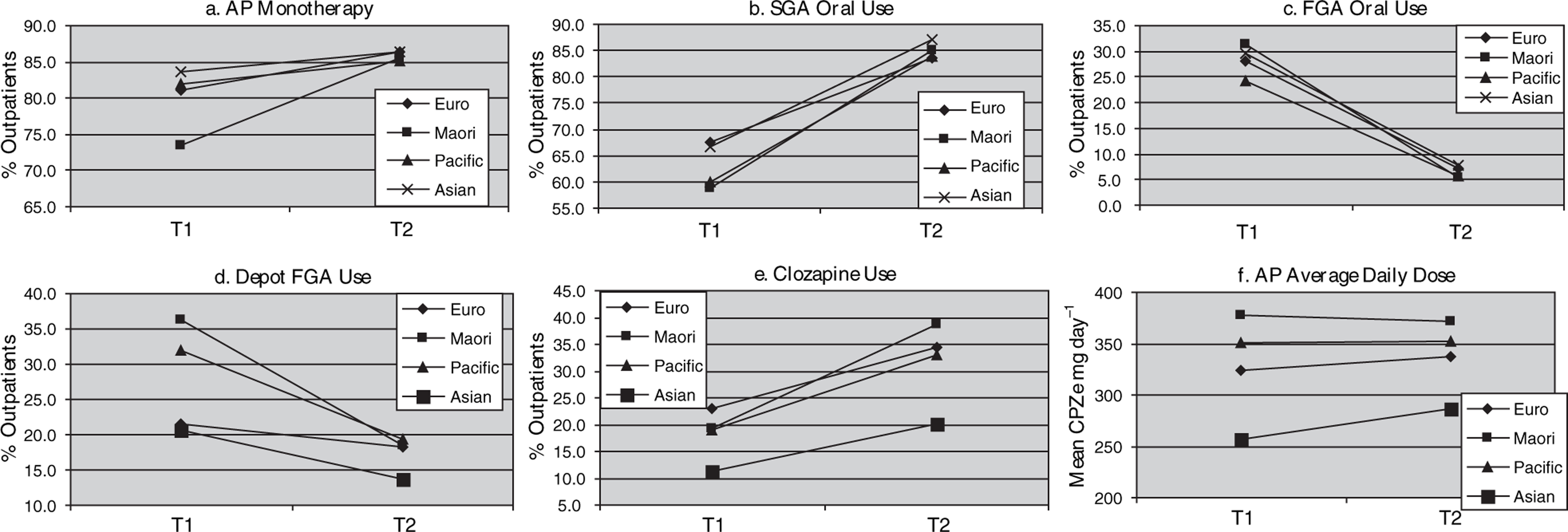
Six prescribing outcome variables (adjusted for age and sex); ethnic group changes between T1 (31 March 2000) and T2 (31 October 2004). CPZe, chlorpromazine equivalent.
Rates of antipsychotic monotherapy prescribing by ethnic group and time
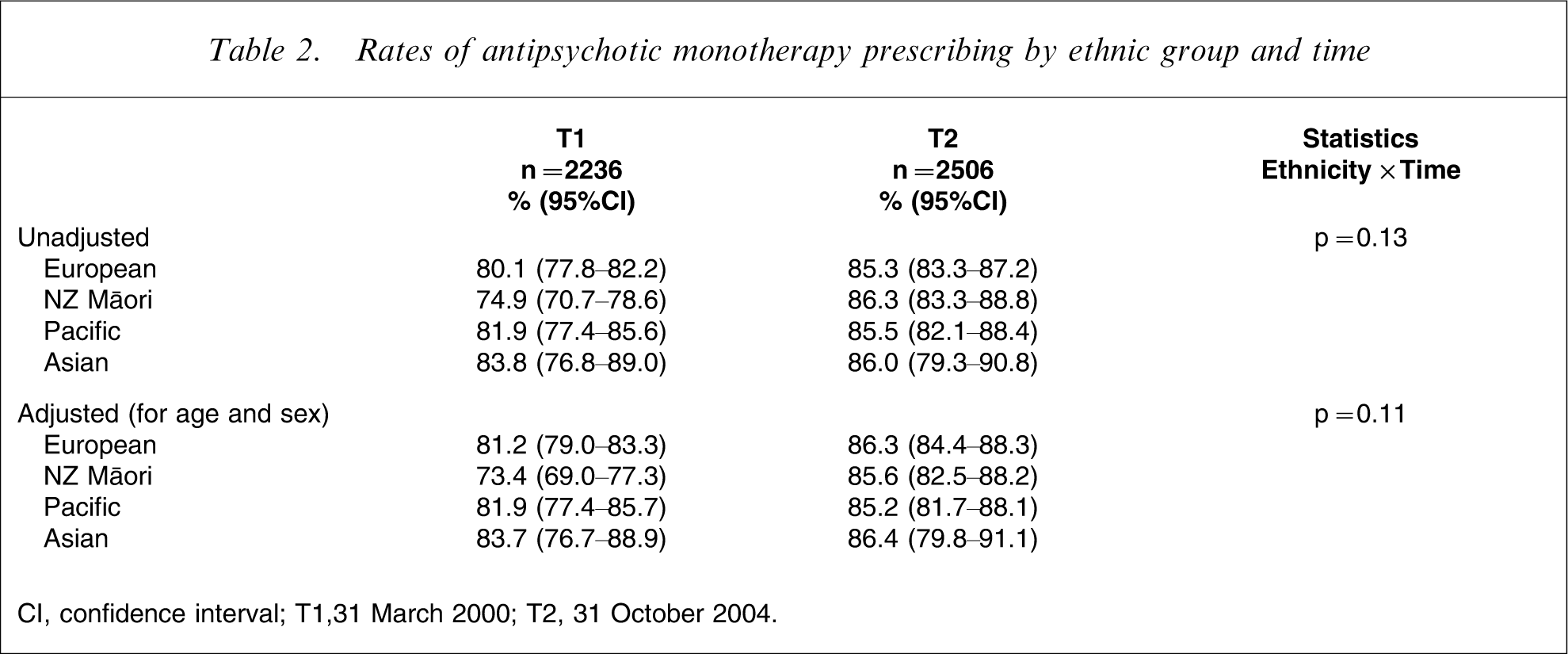
CI, confidence interval; T1,31 March 2000; T2, 31 October 2004.
Second-generation antipsychotic prescribing
The baseline audit found significant differences in the adjusted rates of oral SGA use between ethnic groups (p = 0.004) (Table 3), with Māori and Pacific subjects having the lowest rates (59% and 60%) compared to rates for European and Asian subjects of 67% (Table 3). The size of the change over time varied across groups but after controlling for age and sex it did not reach the probability level set for statistical difference (Table 3). Figure 1(b) shows that all four ethnic groups had rate increases over the study duration (European 16.1%, Asian 20.4%, Pacific 23.8% and Māori 26.3%). When the adjusted rates of oral SGA use were compared at T2 no difference was found between ethnic groups (p = 0.577).
Rates of SGA, FGA and depot antipsychotic prescribing by ethnic group and time
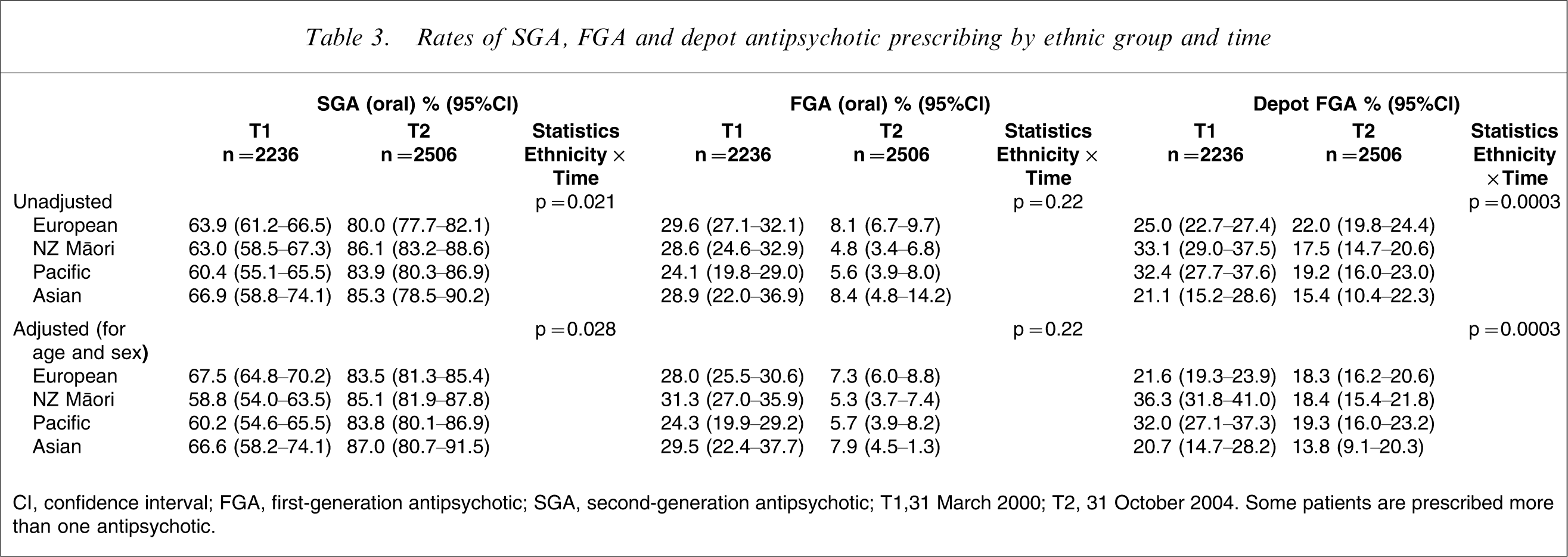
CI, confidence interval; FGA, first-generation antipsychotic; SGA, second-generation antipsychotic; T1,31 March 2000; T2, 31 October 2004. Some patients are prescribed more than one antipsychotic.
Risperidone long-acting injection was not available at T1 and was not funded at T2; there were only 10 outpatients prescribed this antipsychotic by the injectable route at T2 and therefore they have not been included in the analysis.
Depot first-generation antipsychotic prescribing
At T1 there were significant differences in the adjusted rates of first-generation depot prescribing between ethnic groups (p < 0.0001) (Table 3). Māori and Pacific subjects were more likely to be prescribed maintenance treatment by long-acting injection (36% and 32%) when compared to European or Asian subjects (22% and 21%). Over the study duration the prescribing rates for depots reduced in all four ethnic groups. The size of the change over time varied significantly across ethnic groups (Figure 1d), with the greatest change observed for Māori (17.9%) and the smallest for European subjects (3.3%). This effect reached statistical significance in both adjusted and unadjusted analysis of the interaction between ethnicity and time (Table 3). At T2 the adjusted rates of depot use did not differ between ethnic groups (p = 0.490).
Oral first-generation antipsychotic prescribing
The adjusted rates of oral FGA use at T1 were similar between ethnic groups (p = 0.273) (Table 3). Overall a large reduction in use was observed, and by T2 only 5–8% of outpatients were still prescribed these antipsychotics. The size of the change in each ethnic group over time was similar for both adjusted and unadjusted rates (Figure 1c) and there was no difference in adjusted rates of use at T2 (p = 0.649)
Clozapine prescribing
The SGA clozapine was being prescribed at different rates (adjusted) between ethnic groups at the baseline audit (p = 0.007) (Table 4). Asian outpatients were least likely to be prescribed clozapine (11%) compared to Māori and Pacific (19%) and European outpatients (23%). The size of the change over time did not differ significantly by ethnic group (both adjusted and unadjusted rates). All four ethnic groups had increased clozapine prescribing rates by T2 (Figure 1e); Māori increased by 19.6%, followed by Pacific (13.8%) and European (11.5%) and the smallest increase was found for Asian outpatients at 8.8%. At the final audit there was still a significant difference in the adjusted rates of clozapine prescribing between ethnic groups (p = 0.0005) with Asian subjects still having the lowest rates of use (20%) compared to the three other groups, with rates ranging from 33% to 39%.
Rates of clozapine prescribing by ethnic group and time
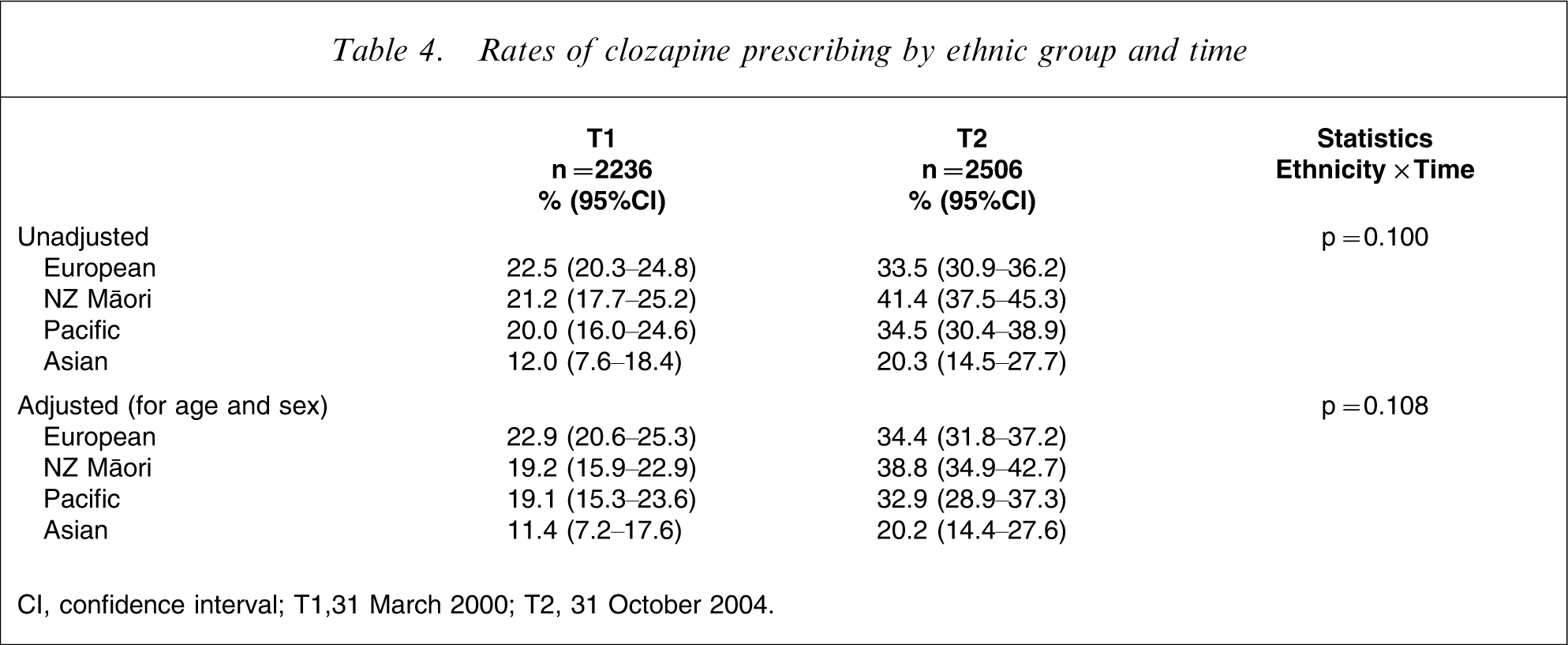
CI, confidence interval; T1,31 March 2000; T2, 31 October 2004.
Antipsychotic dose
The average daily antipsychotic dose (CPZe) prescribed for outpatients at T1 (adjusted) was found to differ significantly between ethnic groups (p < 0.0001) (Table 5). The mean dose ranged from 256 mg day−1 CPZe for Asian subjects to 378 mg day−1 CPZe for Māori; a total difference of 122 mg day−1 CPZe. Figure 1(f) shows that the difference in average daily dose between ethnic groups did not change significantly over time. At T2 there was a mean dose difference between ethnic groups of 86 mg day−1 CPZe and analysis showed this reached the level of statistical significance (p < 0.0001).
Mean antipsychotic total daily dose by ethnic group and time
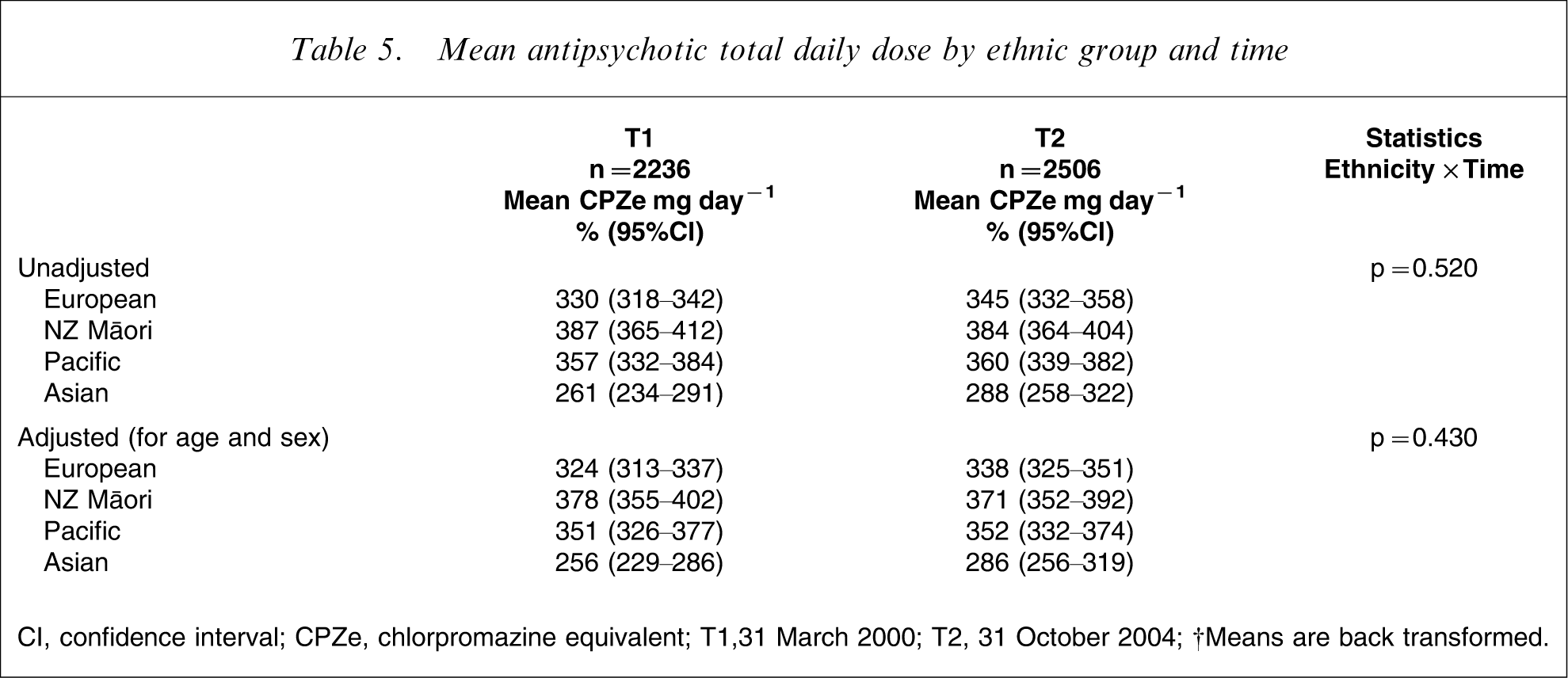
CI, confidence interval; CPZe, chlorpromazine equivalent; T1,31 March 2000; T2, 31 October 2004. †Means are back transformed.
Discussion
Pharmacological treatment with antipsychotics in outpatients with schizophrenia was generally found to be consistent with evidence-based practice guidelines. Differences in baseline prescribing were found between ethnic groups for rates of antipsychotic poly-prescribing, SGA, depot FGA and clozapine prescribing and total antipsychotic dose. Overall five of the six prescribing outcome variables changed over the 4.5 years and only mean antipsychotic daily dose remained consistent across the two time points and with a significant difference between ethnic groups. The average daily dose, however, for each ethnic group was consistent with practice guidance at both time points and did not exceed the recommended maximum for the maintenance treatment of schizophrenia (≤600 CPZe mg day−1) [44].
In the present study we found significantly lower prescribed doses for Asian outpatients that was consistent over time and when controlling for age and sex. There have been mixed reports of ethnic differences in antipsychotic dose in the literature. Studies that have found higher doses prescribed for ethnic minorities such as African–American or Afro-Caribbean subjects have not provided any robust evidence to support the practice but it has often been associated with the prescribing of high potency and/or FGAs [8], [11], [13], [54], [55]. In contrast, several studies have failed to find a difference in antipsychotic dose between black patients and white patients for psychotic disorders [56–59], especially when adjustments for diagnosis, age and gender were made, and Ruiz et al. reported that the dose of antipsychotic needed to obtain a similar clinical response in schizophrenia was the same between black patient and white patient groups [58].
There are, however, fairly consistent reports of lower antipsychotic doses prescribed in Asian treatement populations [60–62] although one study did not find a difference [63]. There are also reports of Asian subjects having higher plasma concentrations of antipsychotics when receiving similar doses [64], [65]. Lin et al. found that significant differences in haloperidol levels existed between Asian and white subjects even after controlling for age, gender, smoking, comorbid illness, concomitant medications and body surface area [65]. The difference was greatest after i.m. versus oral administration of haloperidol, suggesting that pharmacokinetic factors such as hepatic first-pass metabolism is important between ethnic groups. Differences in prolactin levels between Asian and white subjects (independent of the haloperidol concentration effect), also suggested that there may be pharmacodynamic response differences (e.g. receptor sensitivity) between ethnic groups [65]. The pharmacokinetic variation is supported by differences of cytochrome P450 enzyme activities in Asian subjects (e.g. higher rates of a genetic polymorphism that limits CYP2D6 enzyme activity and metabolic capacity) [66], but validation of potential pharmacodynamic, environmental and cultural variations in response to antipsychotics is still required. Additionally, individual patient variables including smoking status and weight have been associated with antipsychotic dose, but these variables were not included in the present study primarily because they were not recorded reliably in the patient file. These may be important variables to include in future studies examining ethnic differences in antipsychotic dose.
In terms of the other explicit prescribing outcome variables, all changed in a positive direction and the gap observed between evidence-based prescribing recommendations and baseline practice for different ethnic groups reduced significantly between 2000 and 2004. The only difference that persisted in October 2004 between ethnic groups was lower rates of clozapine prescribing in Asian subjects. Under-utilization of clozapine in Asian subjects is of concern because of the specific role that clozapine plays in treatment-resistant schizophrenia. There is no reason to suggest that the proportion of people with treatment-resistant schizophrenia will be any different for Asian subjects compared to other ethnic groups and, consistent with other literature, a pilot study comparing Korean–American with white subjects found that Korean subjects required lower clozapine doses but had higher response rates and experienced a higher incidence of mild–moderate side-effects at lower clozapine serum levels (e.g. sedation and anticholinergic effects) than white subjects [67]. Therefore more research is needed to understand why this difference in clozapine utilization for Asian subjects exists.
The greatest changes in prescribing practice were seen for Māori subjects, with reductions in antipsychotic poly-prescribing and for both Māori and Pacific subjects in terms of increases in SGA use and clozapine use alongside reductions in first-generation depot use. Similarly in the USA, Daumit et al. found that the difference in SGA prescribing for psychotic disorders between ethnic groups narrowed throughout 1992–2000, as the overall use of these drugs increased, but the odds were still lower for African–American compared to white and Hispanic subjects in 1998–2000 [22]. More recently, however, a US study of outpatients with schizophrenia attending a community mental health clinic affiliated with an academic centre (2003–2004) found that 95% were prescribed an SGA but that white outpatients were sixfold more likely to be prescribed this treatment than black outpatients after controlling for clinical and sociodemographic confounding factors such as education and insurance status. Of the outpatients who received an SGA, white subjects were more than twice as likely to receive clozapine as part of their regimen. Supporting this, Kelly et al. also found significant under-utilization of clozapine in African–American subjects between 1994 and 2000 [23].
Differences between ethnic groups for SGA prescription rates are not always consistent; both a 2000–2001 study and a 1998–2001 study of inpatient prescriptions found no difference in rates for ethnicity or gender [59], [68]. Alongside the lack of difference for SGA prescribing, however, the latter study found that African–American men more frequently received depot antipsychotics [59]. Overall, the US literature from the last decade indicates that the quality of schizophrenia treatment, particularly clozapine use, differs for some ethnic minorities.
The changes in schizophrenia treatment disparities observed in the present study since 2000 are encouraging. One reason for the absence of most differences in antipsychotic prescribing outcomes in 2004 between ethnic groups may be increased attention to the issue of overall health disparity between ethnic groups as a result of the NZ Government's Health Strategy [25], and increasing attention to addressing disparity in the treatment of mental illness with the development of a National Mental Health Strategy and Blueprint for Services [28], [38], and strategic objectives specifically for Māori [69] and Pacific people [70]. In response to these objectives, health boards in Auckland began to address the specific mental health needs of Māori and Pacific people with the development of culturally appropriate community mental health services. These services were introduced across the three regions of Auckland, initially providing cultural and support services to patients (and their whanau/families) receiving care in mainstream mental health services, but more recently they have incorporated both clinical and cultural services in their delivery of mental health care. The growing Asian population in NZ has also been acknowledged in the last 2–3 years, with the development of Asian health services for cultural and translating support, and Asian mental health nursing positions to provide clinical support to mainstream mental health services for Asian patients and their families.
It has been postulated that in the treatment of schizophrenia, language and communication difficulties could lead to some of the ethnic differences in medication management practices reported in the literature. This may stem from misinterpretation of symptoms and severity of symptoms, misdiagnosis and misinterpretation of medication side-effects. From a patient's (and family's) perspective it may also result in mistrust, poor cooperation with mental health clinicians and poor compliance with treatment. An obvious way of improving this situation is the provision of culturally sensitive services that can match mental health workers with the same ethnic background or spoken language as patients. Studies have shown that matching is preferred by patients, can reduce dropout from services, can improve the patient–clinician relationship and antipsychotic medication compliance, and reduce rates of depot antipsychotic use [71–74]. Although not all Māori and Pacific outpatients in the present study were receiving care from the culturally specific mental health services, increasing cultural awareness and access to cultural and support staff for Māori, Pacific and Asian outpatients in mainstream mental health services may have contributed to the study findings.
A second contributory explanation is the impact of ongoing clinical audit and feedback. The research team provided feedback to all three services after the first audit, highlighting the gap between current and optimal practice in terms of ethnic variations in antipsychotic prescribing. The feedback also included educational meetings focusing specifically on clozapine use in the community; identification of barriers to change; and suggested mechanisms to address the barriers. Ongoing audit and feedback to reinforce prescribing change also occurred in two of the three health services (District Health Boards [DHB] A and B) at two additional time points (in October 2001 and March 2003) before the final audit with all three services in October 2004. A solution implemented by two of the DHBs (A and B) involved in the present study to facilitate the increasing access to oral SGAs and clozapine was the development of assertive community teams. DHB-B in particular increased the size of their mainstream assertive community team and introduced a Māori-specific assertive community team after the baseline audit. The patients who accessed these teams were diagnosed predominantly with schizophrenia and in DHB-B, because of the different ethnic composition of the schizophrenia population, they were predominantly Māori and Pacific people. Frequent assertive outreach including daily medication administration made a significant contribution to the changing patterns of antipsychotic prescribing.
A third possibility may be related to the increasing market share and reliance on SGAs in clinical practice; the range of oral FGAs is rapidly reducing as they are being withdrawn from the market and the cost of SGAs has fallen significantly with the increasing availability of generic products. Finally, considerable efforts have been made by health services and professional and educational organizations to promote the uptake of evidence-based treatments, with the development and dissemination of practice guidelines and treatment algorithms since the mid-1990s. It is likely that all of these explanations contributed to the change in antipsychotic prescribing for ethnic groups between 2000 and 2004, and the overall absence of most disparities in the pharmacological treatment of schizophrenia between ethnic groups in 2004.
The strengths of the present study include the large sample size and ethnic diversity of the study population. The study was also conducted in large public mental health services providing free care to patients. While these patients may not be representative of the socioeconomic status of the general population, they are likely to be representative of the schizophrenia population, increasing the economic homogeneity of the study population. In addition, the prescribing practices reflect >50 practitioners working at multiple sites in different regions. There are limitations, however, in using retrospectively recorded case note information. The cross-sectional nature of the study did not include and control for the many other factors that may have influenced antipsychotic prescribing decisions such as each patient's clinical presentation and severity of symptoms, their comorbid mental and physical conditions and their antipsychotic treatment history.
Ethnicity data in the present study were collected differently to the 2001 census, which allowed a number of ethnic groups to be self-selected and the use of a prioritization algorithm to identify ethnic groups in ranked order. This difference means that conclusions drawn from comparisons between these two datasets should be interpreted with caution. The use of differentially collected ethnicity information to inform national health data sets has been identified as an ongoing problem for NZ. Ajwani et al. found that by including the census data question on mortality data it was possible to improve ethnicity data quality. They recommended that health services should implement the standard 2001 census question in their data collection systems [75]. Misclassification of ethnicity may also have caused errors in the rates reported in the present study, but it is not possible to predict in which direction this may have confounded the findings.
The present study found that most baseline differences in antipsychotic prescribing between ethnic groups resolved over time, with equal access for outpatients to recommended best practice with antipsychotic treatment in schizophrenia. These findings are not consistent with reports of the experiences of ethnic minorities in the Northern hemisphere. Further work is required to look at differences in access to clozapine treatment in Asian subjects.
Footnotes
Acknowledgements
The authors would like to thank Mental Health Services of Counties Manukau, Auckland, and Waitemata District Health Boards (DHB), Eli Lilly NZ, AstraZeneca NZ, Janssen-Cilag NZ and Novartis NZ for unrestricted research grants. Thanks also to the data collectors, Kirsten Norris, Jocelyn Byrd, Andrea Kelleher, and Karen Day, and Mental Health Services staff from the three DHBs. We are also grateful to Assoc. Professor Tim Lambert for database and statistical support in the initial stages of this project, Dr Grant Paton-Simpson for database support, Dr Gail Robinson for clinical support and Dr Joanne Baxter, Dr Sylvia van Altvorst, Dr Tamasailau Suaalii-Sauni, Assoc. Professor Janie Sheridan and Professor Peter Joyce for their feedback and support.