
Abstract
Objective
Long-term assessments of gatekeeper training (GKT) with multiple follow-ups are rare. Therefore, the aim of the current analysis is to examine 12-month follow-up outcomes of SafeTALK training in addition to the earlier analysis of pre-, post-, and 6-month follow-up.
Method
Two hundred and sixty two community volunteers participated in half-day (4-h) gatekeeper training sessions. Before, after, and 6- and 12-month follow-up surveys were used to assess participants’ knowledge, efficacy, and reluctance to intervene. Linear mixed effects regression was used in statistical analysis.
Results
Fifty six participants (21.4%) completed the 12-month follow-up, representing an attrition rate of 78.6% from pre-test. Linear mixed model analysis revealed a significant, consistent effect for time for knowledge, efficacy, and reluctance. Post-hoc testing revealed significant differences between scores at pre-test and 12-month follow-up for GK knowledge and efficacy; however, no significant difference was seen between these time points for reluctance to intervene. No significant change was measured between the 6 and 12 months for any outcomes. GK knowledge and efficacy remained significantly above pre-test scores.
Conclusion
The evaluation of the GKT demonstrated the long-term effectiveness of community-based suicide prevention training programs to improve and maintain GK knowledge and efficacy.
Gatekeeper training (GKT) refers to training in suicide prevention provided to people in care roles likely to be in contact with those at risk of suicide and is an important part of any multi-faceted suicide prevention strategy. 1 GKT has been delivered to a broad range of audiences, such as workplaces, 2 schools with both students 3 and staff, 4 and in general community populations. 5 Evaluations of GKT demonstrate the effectiveness in improving GK knowledge, preparedness, behavioural intention, and confidence to intervene.6–9 However, previous literature has identified a general decline in GKT outcomes over time. 10 These findings highlight the need for an increased understanding of the long-term training effects of GKT. Only a few studies have evaluated GKT in the general population. Evaluating the long-term impact of GKT in general or community populations is vital to understanding the potential benefit such training may have in communities and the frequency with which this type of training should be made available to maintain positive GK outcomes.
The present study builds on the previously published evaluation of GKT using pre-, post-, and 6-month follow-up study design. 5 Findings from the previous analysis indicated that, compared to baseline, training effects for three of four outcomes were maintained at 6 months post-training. Namely, knowledge, preparedness, and GK efficacy demonstrated improvement that was preserved over time. When comparing post-training scores, however, this preservation declined in each outcome from post-test to 6-month follow-up. It is unclear if this decline is continuous over time. Therefore, the present analysis aimed to further evaluate the longitudinal effectiveness of GKT in improving knowledge and efficacy, and reducing reluctance towards suicide intervention in a community sample 12-months following training.
Method
Intervention
The GKT involved 12 half-day (4-h) in-person SafeTALK sessions 11 on the Sunshine Coast, Queensland, Australia. Sessions were conducted from February until November 2019. The same GKT facilitator conducted all trainings at the same location.
Recruitment
Recruitment occurred via e-newsletter distribution to members of the Alliance for Suicide Prevention Sunshine Coast and a social media marketing campaign targeting all Sunshine Coast residents. A total of 317 community members voluntarily participated. Informed consent was sought prior to participation. No incentives were offered for participation. Regardless of research participation, all attendees received the same training at no cost with no changes to the provision or content. Demographic information was collected only from consenting participants. All procedures were approved by the University of the Sunshine Coast Human Research Ethics Board (S181250).
Procedure
Data were collected from participants in person immediately prior to and following training and by online survey at 6-month follow-up (for detailed methodology see Holmes et al. 5 ). Twelve months after completing the GKT training session, participants were emailed a link to complete their final follow-up survey. The follow-up survey was provided via an online link available for completion on computer or mobile platforms. Participants were prompted once at 7 days following initial email if they had not completed the survey. The survey was available for 21 days from the initial email. Responses were case matched to pre- and post-test responses via emails linked to participant codes generated from participant names.
Questionnaire
The questionnaire of Wyman et al. 6 was adapted for use in general population. The online 12-month survey included demographic questions (five items) and assessed three GK outcome scales (14 items). The scales assessed were as follows: (i) perceived knowledge; (ii) GK efficacy, and (iii) GK reluctance to intervene. The survey took approximately 5–10 min to complete.
Similarly to the pre-, post-, and 6-month follow-up, 5 the 12-month follow-up assessment demonstrated excellent reliability for the GK knowledge scale and acceptable reliability for GK efficacy and reluctance, as tested by Cronbach’s α (respectively, α = .95, .78, and .80).
Data analysis
Responses were exported from Qualtrics survey software for analysis in IBM SPSS Statistics version 27. The Shapiro–Wilk statistics indicated normal distribution was present for GK knowledge and efficacy outcome measures. However, the assumption of normality was violated for the outcome of GK reluctance. Subsequent analysis of histograms, and skewness and kurtosis statistics indicated acceptable normality of data range −1.5 to +1.5 12 ; and this outcome was preserved for analysis. Little’s test indicated data are missing completely at random (X2 = 286.25, df = 248, p = .058).
Linear mixed effects regression was used to evaluate changes in GK outcomes over time. This analysis was applied for its ability to deal well with missing data in our data set due to attrition at follow-up. Post-hoc testing was conducted to determine differences between specific time points, comparing all four time points to each other.
Results
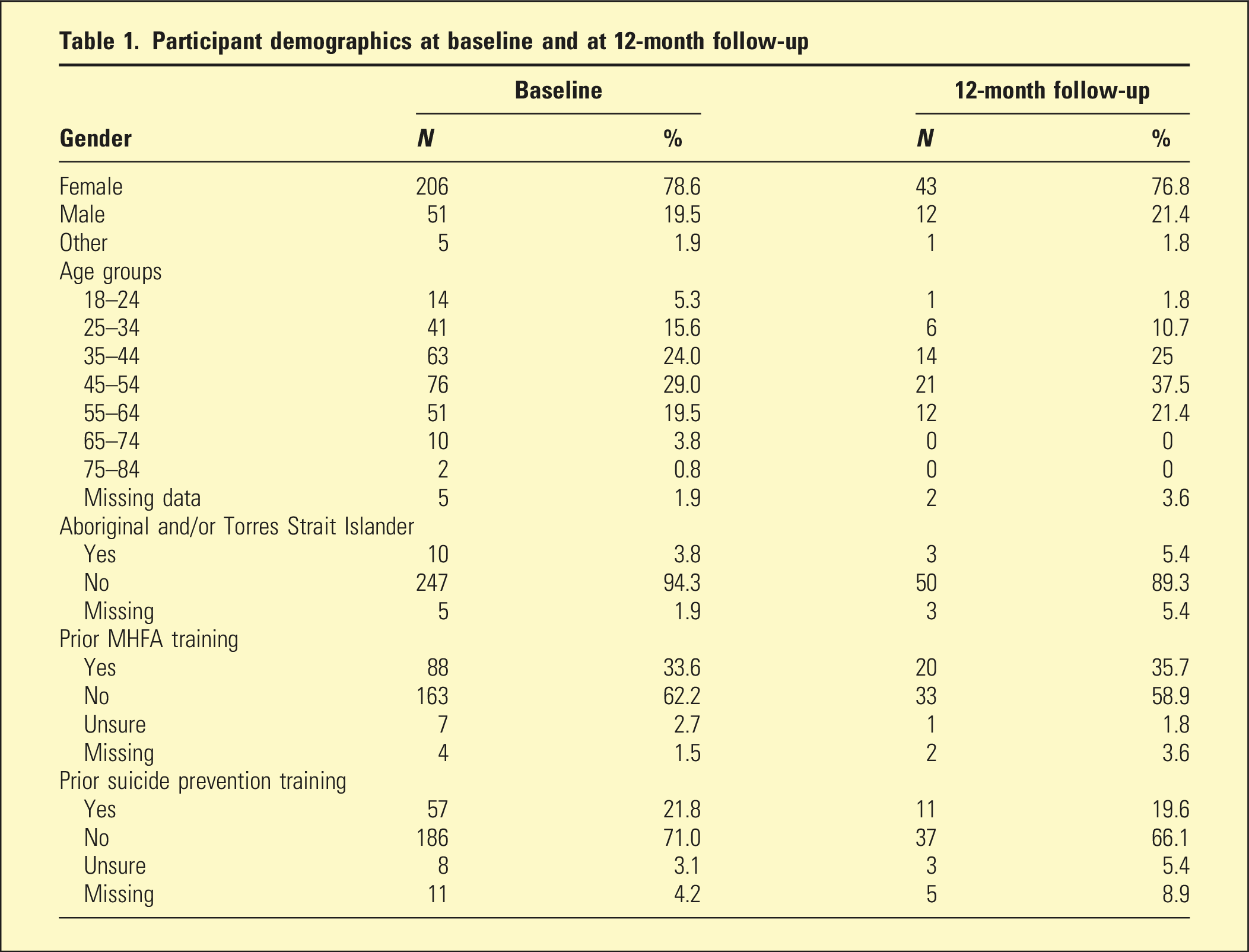
Participant demographics at baseline and at 12-month follow-up
Mean differences for all GK outcomes from pre-GKT to 12-month follow-up
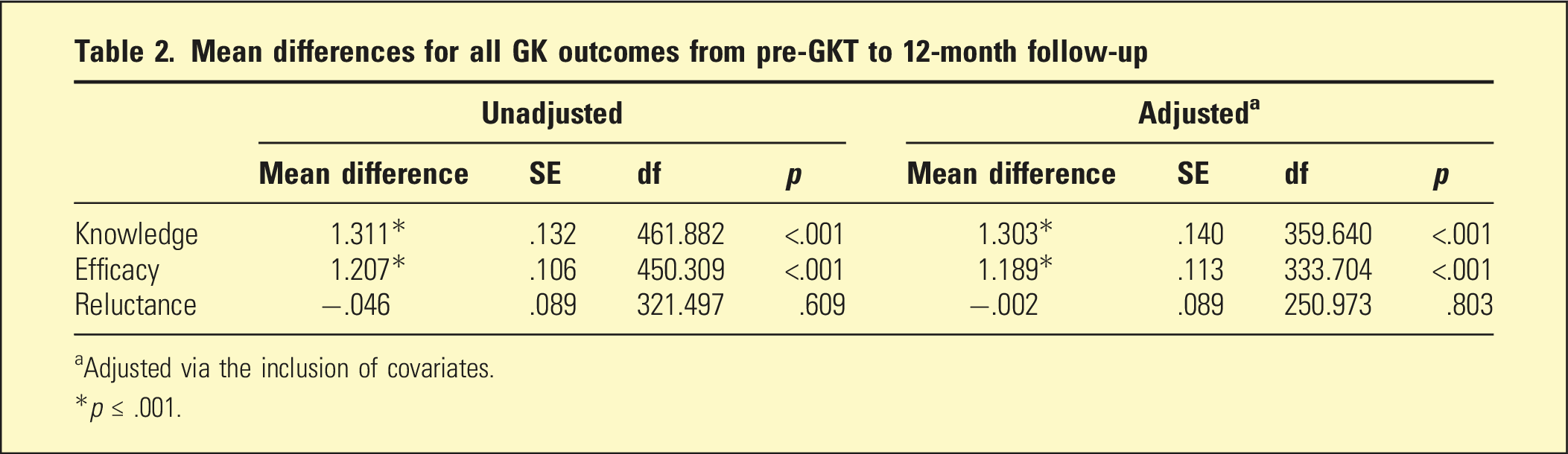
aAdjusted via the inclusion of covariates.
*p ≤ .001.
Estimated marginal mean scores for outcome variables at each time point based on unadjusted and adjusted linear mixed model
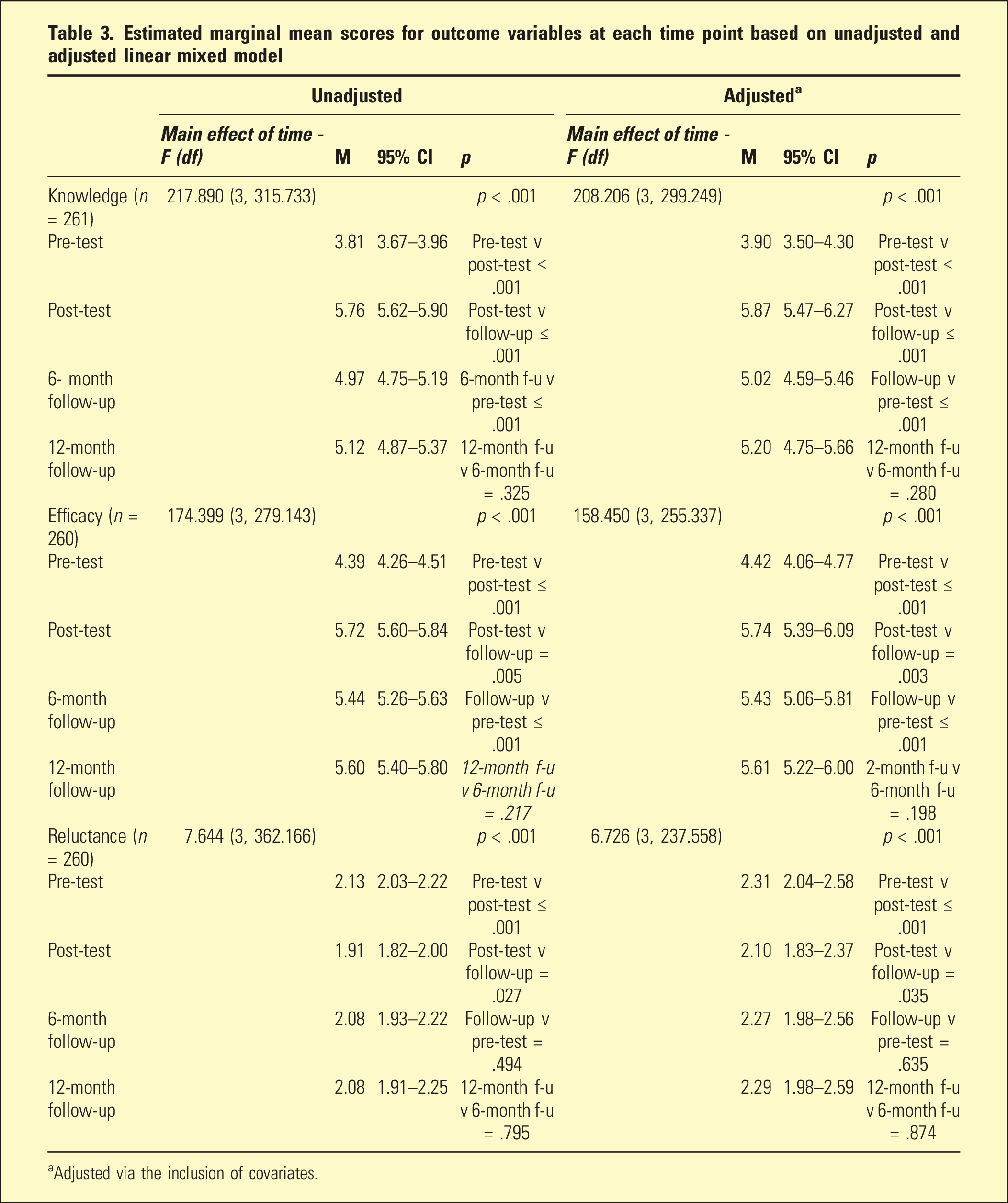
aAdjusted via the inclusion of covariates.
There was no significant change in outcome measure scores between the 6-month and 12-month time points, indicating a plateauing of GK knowledge, reluctance, and efficacy. GK knowledge and efficacy remained significantly above pre-test scores (Figure 1). Mean change over time by outcome measures.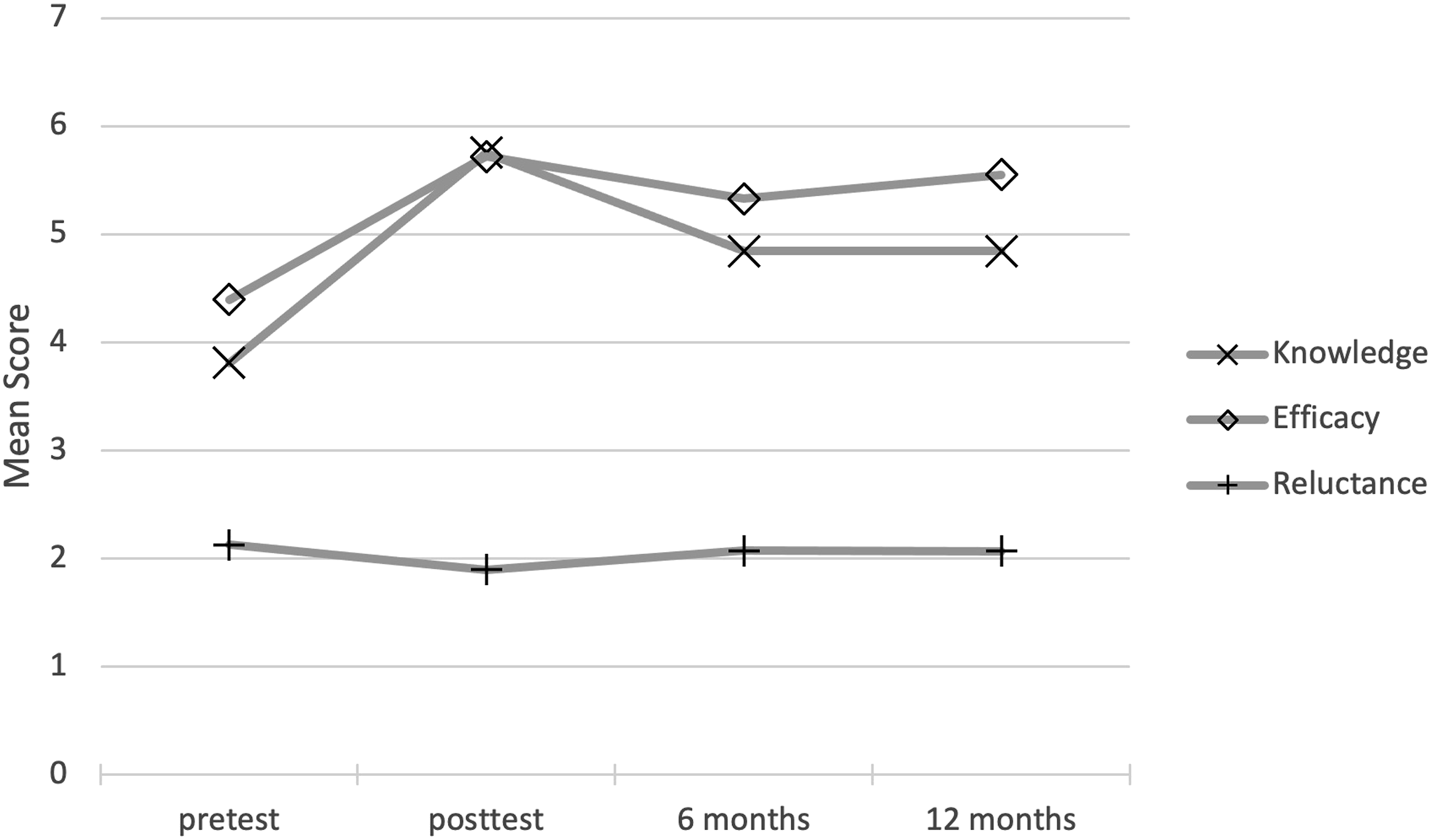
Regarding factors and covariates (Table 2), prior training in suicide prevention was significantly associated with increased knowledge and efficacy (p < .001). Prior training in MHFA was also significantly associated with increased knowledge (p < .05). All other demographic covariates returned non-significant effects.
Discussion
Considering the lack of long-term evaluation, the current analysis aimed to evaluate the maintenance of GKT outcomes in a community sample 12-months after GKT. The 12-month follow-up results found that knowledge and efficacy are preserved above pre-training levels and do not appear to reduce further from 6- to 12 months. This indicates a stabilisation of GK outcomes in trained community members following the 6-month follow-up results and is evidence of a non-linear decline of GKT outcomes. Participant retention of training outcomes over many months increases their knowledge to respond to suicidality if, and when, it is encountered within their community. Likewise, participants’ belief in their ability to provide GK support to someone experiencing suicidality is improved with GKT, and these improvements are enduring. Improving GK efficacy may increase the motivation of individual GKs to apply their skills in practice, increasing the potential for individuals at-risk of suicide to be supported to care. These findings offer significant support for applying GKT in the community, as it is more likely that people trained in GK skills will be able to identify and respond to signs of emotional distress. By creating more opportunities for the earliest possible intervention, GKT in communities could potentially reduce the occurrence of suicidal crises by building a responsive network of support for individuals at risk of suicide that extends beyond formal first responders.
Self-rated scores of reluctance to intervene were found to return to baseline in the community sample investigated in this study. That is, participants’ reluctance to connect people who may be experiencing suicidality with formal support is not significantly changed through GKT. This finding is unfortunate and is possibly due to the enduring nature of individual attitudes (in this case, towards suicide and intervention behaviour). Attitudes are difficult to change and often remain relatively enduring despite education and training interventions. 10 Additionally, the specific GKT intervention used (SafeTALK) does not actively seek to target changing attitudes towards suicide. Instead, it aims to provide education and specific skills pertaining to identifying, interacting with-, and responding to someone at risk of suicide. Nevertheless, reluctance to intervene represents a barrier to GK intervention behaviour in need of further study.
Implications
The significant finding that knowledge and GK efficacy are maintained over 12-month provides considerable insight into the frequency in which GKT should occur within the community. ‘Refresher’ or ‘booster’ training has previously been proposed to mitigate training decline.13,14 However, there is currently no literature to assess the effectiveness or frequency of these proposed sessions. The current study provides an understanding of the non-linear trajectory of decline of training effects and should be considered when developing proposed frequency schedules of refresher training. Findings indicate recommendations for booster training or re-training may include yearly updates. However, support can be interpreted for recommendations of longer intervals until re-training due to the plateau of decline in outcomes between 6- and 12 month following training. There is no evidence currently detailing the trajectory of decline following 12 months; thus, no specific recommendations can be made. What is apparent is the significant improvements over 12 months supporting the longitudinal efficacy of GKT in the general community.
Limitations
Some limitations should be considered. Firstly, the instruments used in this study were adapted for application in a general community sample and have not been validated. Secondly, the sample included volunteers and may be biased towards community members interested in taking action. Thirdly, before and after with follow-up design (single-arm) was used rather than a randomised controlled trial, which limits the comparison with a control group. Lastly, participant attrition did limit the power of analyses that were undertaken. However, attrition rates of this nature stemming from the use of online survey delivery are not uncommon in GKT evaluation literature.8,9 As demographic variance remained comparable across all time points in this study, the reliability of the findings was not critically compromised.
Conclusion
The present longitudinal evaluation of GKT demonstrated the long-term effectiveness of community-based suicide prevention training programs to improve and maintain GK knowledge and efficacy. The long-term preservation of knowledge and efficacy increases GK ability as well as belief that they will be able to identify, support, and connect an individual at risk of suicidality to appropriate assistance.
Footnotes
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Australian Federal Government.