
Abstract
The purpose of the present paper was to identify, from the voluminous literature on efficacy and safety in new-generation antidepressants (NGAs) with depressed children and adolescents, practical clinical strategies for acute phase treatment. To this end a pragmatic survey of studies and reviews was undertaken. Meta-analyses of randomized controlled trials of NGAs in depressed children and adolescents have noted a comparative lack of efficacy, and a weak but statistically significant increased risk of self-harm and suicidal thoughts. But NGA prescription rates and youth suicide rates are generally inversely related, and ensuing ‘black box’ warnings about NGAs, by deterring NGA prescribing, have possibly contributed to rising youth suicide rates. In moderate–severe depression, benefits for fluoxetine and possibly other NGAs demonstrably outweigh risks. NGAs are not present in adolescents who die by suicide. Concern about NGA risks must be balanced against risks of non-treatment. While mild depression entails regular review, psychoeducation, self-care strategies and psychological interventions, NGAs should be administered concurrently with psychological treatments if depression is moderate– to severe, or if mild depression persists. Patients should be warned about off-label status of NGAs in depression, serious side-effects such as ‘activation’, suicidality, emotional blunting and manic switches, the need for adherence and avoiding abrupt discontinuation. They should be monitored early and regularly. Better evidence is required regarding psychological treatments, clinical course, and clinical practice trends. In moderate–severe depression the risk of suicide if NGAs are not used may outweigh any risk of self-harm associated with them.
The prescription of antidepressants to children (ages 1–11) and adolescents (ages 12–17) is currently controversial, with recent expert and public debate dominated by concerns over efficacy and, particularly, safety of the new-generation antidepressants (NGAs). On the one hand, the efficacy of NGAs (selective serotonin re-uptake inhibitors (SSRIs) and serotonergic–noradrenergic antidepressants (SNAs)) is questionable for their commonest indication (depression in young people) and they are reportedly associated with increased risks for self-harm [1–3] and suicidal thoughts [1], [3]. On the other hand, at a population level, youth suicide victims are almost never taking antidepressants [4–8], and decreased suicide rates are associated with increased antidepressant prescription rates, although evidence is weakest for adolescents and children [9–12]. These contrasting findings highlight the difficult task clinicians face in weighing competing risks, identifying clinical strategies and individualizing treatment.
Numerous meta-analyses and/or systematic reviews have considered this topic generally [12–16] and in children and adolescents [1], [3], [17–28]. This pragmatic review focuses on NGA usage with depressed adolescents, and acute phase management, because little is known about treating chronic depressive conditions. In the light of the voluminous, yet changing evidence, it offers parameters regarding NGA treatment.
Rise and fall of antidepressant usage by young people
Although the typology of child and adolescent depression is contested and it has risk factors distinguishing it from adult depression [29], it is, like the latter, common, disabling and potentially dangerous. Depressive disorders affect 3.0% of Australians aged 6–17 in the previous year [30], and the USA lifetime prevalence of an episode of major depressive disorder (MDD) for 15–18-year-olds is approximately 14% [31].
Often chronic, it also carries significant social, psychological and physical morbidity and the burden of stigma. Depression, although a cardinal risk factor for child and adolescent suicide (the odds ratio is 11–27 [32]), remains underrecognized and under-treated [33].
Prescription rates for adults and children rose through the 1990s, levelling off around 2000, and in the USA are now in decline [34], [35]. Practice guidelines in the late 1990s suggested that NGAs were more effective, safer and better tolerated by children than tricyclic antidepressants (TCAs) [36]. Certainly they were (and are) less lethal in overdose [37]. Widespread prescribing created a disincentive for pharmaceutical companies to conduct paediatric research. Increased agreement that depression occurs in children [38] – with a form like that in adults and the same DSM-IV criteria – may have implied (not necessarily correctly) a similar pathogenesis and treatment response.
Efficacy/effectiveness of antidepressants in depression
The TCAs fell out of favour early on, with initial and follow-up meta-analyses of their effectiveness [39], [40] indicating no useful effects in pre-pubertal children, but possibly modest effects in adolescents, particularly with increasing age.
Randomized clinical trials (RCTs) of fluoxetine [41], [42], sertraline [43] and paroxetine [44] concluded that SSRIs were beneficial in children. Meta-analyses, however, raised major questions about the efficacy of NGAs, and found that (possibly) only fluoxetine showed efficacy for depression [17], [27]. In early 2004, the US Food and Drug Administration (FDA) reviewed published and unpublished trial data on efficacy of SSRIs in paediatric depression. From 15 paediatric trials it concluded that only three (two fluoxetine trials [41], [42] and one citalopram trial [45]) showed evidence of efficacy, defined as a statistically significant (p < 0.05) superiority of active medication over placebo on the primary outcome measure. A trial of paroxetine [44] was positive on several secondary end-points but not the primary outcome, while two sertraline trials had a positive primary end-point only when their data were pooled and analysed [43]. Skepticism was expressed regarding skewing towards positive results for some studies [17].
The placebo effect is marked. The Kirsch and Antonuccio meta-analysis of nine studies of antidepressants in child depression, found that placebo response was 87% of the drug response, 75% of SSRI response, and 97% of TCA response [46]. The therapeutic relationship and non-specific aspects of (even pharmacological) interventions may help explain this [17].
Anti-depressant benefits may be more evident with more severe depression and for adolescents (i.e., with increasing age). This belief, although challenged [47], is supported by the benchmark Treatment of Adolescent Depression Study (TADS) [48], funded by the National Institute of Mental Health (NIMH). The TADS methodology has been variously criticized, especially regarding its double-blind comparison of fluoxetine and placebo but lack of blinding when comparing cognitive behavioural therapy (CBT) and combined fluoxetine and CBT [49], [50]. But one of its strengths is including participants similar to those in clinical practice (96% with moderate to severe depressive symptoms; clear impairment; over half with co-morbid mental disorders; and 29% with clinically significant suicidal thinking). TADS assessed the risk–benefit balance by calculating the number needed to treat to benefit (NNT) and the number treated before a harm-related event occurred (NNH). For fluoxetine, the NNT for ‘much or very much improvement’ was 4 and the NNH was 25 (3 and 50, respectively, when combined with CBT [51]), clearly suggesting that treatment benefits outweigh risks. Combined treatment surpassed fluoxetine for moderate depression and depression with significant cognitive distortion, but not marked to severe depression [52]. Another (albeit non-placebo) comparison [53] supports this, suggesting symptom relief is critical for successful psychotherapy in this group. By 36 weeks, combination treatment, fluoxetine alone and CBT all produced clinically meaningful improvement although CBT did not catch up till week 30 and fluoxetine alone had more treatment-emergent suicidal events [54].
Finally, the Bridge et al. meta-analysis assessed clinical response and risk for reported suicidal ideation and attempts in 27 RCTs [18]. In 13 MDD trials it found a pooled difference in rates of response between antidepressant and placebo of 11% (95% confidence interval (CI) = 7–15) and an NNT of 10, compared with a difference of 1% (95%CI = −0.1 to 2%) and an NNH of 112 for harm-related events [18]. Pooled response rates for MDD were higher for adolescents than children, for those with shorter rather than longer depressive episodes, and in trials with less sites. For children (<12 years) with MDD, only fluoxetine (three trials) showed benefit over placebo. No evidence was found for publication bias. Full remission rates, however, are only between 30 and 40% [28], [52], [55].
These clinical trials suggest that fluoxetine is efficacious in paediatric depression [19]. Sertraline may also be effective: NNTs range from 2 to 10, and are greater for adolescents than children [56].
Efficacy/effectiveness of antidepressants in other disorders
Unlike for depression, antidepressants for obsessive–compulsive disorder (OCD) are regarded as clearly effective, despite only a dozen studies [57]. Anxiety also responds better to antidepressants [58].
Bridge et al. confirm this, showing a pooled difference in response rates between antidepressant and placebo for MDD of 11% (95%CI = 7–15%), for OCD of 19.8% (95%CI = 13.0–26.6%), and for non-OCD anxiety disorders of 37.1% (95%CI = 22.5–51.7%) [18]. This gradient in strength of effect is possibly due to the chronicity, stability and greater homogeneity of anxiety, compared with depressive disorders [18], [59], [60].
‘Suicidality’ and black-box warnings
In the early 1990s case reports linked fluoxetine and suicidality in adults [61–63] and children [64]. The concept of ‘suicidality’, which includes suicide attempts, planning or preparation, potentially dangerous behaviour, and suicidal ideation, is imprecise and its usage criticized [22]. Either way, meta-analyses of 17 RCTs by manufacturer Eli Lilly [65] and an FDA advisory group [66] found no link.
In mid-2003 GlaxoSmithKline (GSK) informed the UK's Committee of Safety in Medicines (CSM) and the FDA of increased risks of suicidality associated with paroxetine use in children and adolescents. This prompted CSM and FDA warnings against paroxetine in this group. The FDA then asked all NGA manufacturers for patient-level datasets on paediatric suicidality [13]. Preliminary analyses suggested increased risk [20]. Standardized re-coding of suicidal content by Columbia University experts preceded further FDA analyses of pooled data from 24 RCTs, of which 16 studied efficacy for MDD, four for OCD, three for social or general anxiety disorders, and one for attention-deficit–hyperactivity disorder. They included five SSRIs (citalopram, fluvoxamine, fluoxetine, paroxetine and sertraline), and four SNAs or atypicals (venlafaxine, mirtazapine, nefazodone, and bupropion) [1].
These data combined with publicity and concern from officials, committee members and families of children who died by suicide, induced the FDA in October 2004 to issue ‘black box’ warnings for all antidepressants, not just the analysed NGAs. The Committee on Human Medicinal Products of the European Medicines Agency concluded that paediatric depression should be treated with antidepressants (including fluoxetine) only in special cases [67]. The Australian Therapeutic Goods Administration (TGA) in 2004 summarized that ‘the strongest association has been found with paroxetine and venlafaxine, but sertraline, citalopram and fluoxetine have also been implicated, with fluoxetine possibly having the smallest risk. There are very few data for fluvoxamine’ [68].
The FDA analyses, re-analyses and a further independent re-analysis gave consistent although not identical results: suicidality occurred in just under 2% of patients, with a higher incidence in antidepressants compared with placebo, and relative risk and odds ratio was approximately 2.0 [1], [20], [21]. For example, Hammad et al. found suicidality of 4% versus 2%, risk ratios for individual analysed antidepressants of 1.4 to 5.5, and an overall risk ratio for all analysed antidepressants of 2.19 (95%CI = 1.50–3.19) [1]. Causal significance has been attributed to this finding [1]. Venlafaxine was the only individual drug for which increased risk was statistically significant [1] (although adult venlafaxine users have a higher burden of suicide risk factors [69], [70]).
Supporting the FDA findings, a UK-based nested case–control trial of antidepressants for first-episode depression found weak evidence of increased non-fatal self-harm with SSRIs versus TCAs in 3830 people aged 10–18, but not adults [2]. Unlike the FDA, however, Bridge et al. used a random effects model (like [21]) that assumes and assesses heterogeneity across studies rather than ignoring it, thus providing more conservative estimates of effect size [18]. They included several new studies and considered risk differences as well as risk ratios, because trials with no events could not be included in the latter estimates. While they found the same increased risk for suicidality across all trials and indications, pooled risk differences within diagnostic groups (MDD, OCD, anxiety disorders) were not statistically significant. For OCD and anxiety disorders, as for MDD, suicidality risk ratios were increased at least twofold, but the higher base rate for suicidality in MDD makes this of greater clinical significance in MDD. The overall risk–benefit profile was favourable for these disorders [18]. A possible conclusion is that suicidality appears related to the disorder rather than the treatment.
In adults, although SSRIs are efficacious [71], concerns have been raised about suicidal and homicidal thoughts and behaviour in medico-legal case reports [72–75]. Systematic reviews of trials involving 40 000 and 87 650 adults, respectively [14], [15] noted increased risks of suicide attempts and self-harm, but not suicide. Recent FDA analyses [76] found that in younger patients the odds of suicidality were higher when receiving antidepressants than when receiving placebo, and the reverse in older patients. Thus in May 2007 the FDA extended its black-box warning to include adults aged 18–24 [77].
Quality of evidence
The FDA findings, while consistent and highly influential, received widely ranging criticisms. The RCTs underpinning them provide constrained information. They frequently group children and adolescents, and exclude participants with marked to severe depression, psychotic or melancholic features, comorbid conditions and suicidal thoughts, thus removing more severely ill patients for whom clinicians would use pharmacological treatment. Their brief duration (usually 3–8 weeks) does not mirror clinical practice's longer-term treatment [78]. The FDA's Adverse Event (AE) Reporting System for spontaneous or elicited reports of suicidality at regular reviews does not gauge the real AE rate, because increases were associated with media publicity and the advent of online reporting [79]. No statistical risk was found when questionnaire data on suicidal ideation/behaviour completed at each clinical review were used [3]. Risk estimates were reduced when random effects models and pooled risk differences were used [18], [21].
Moreover, the Columbia AE re-classification necessarily involved inferences: stated suicidal intent was often absent, and it omitted standard criteria, such as explicit lethal intent, an objective plan and failure to notify others, found in suicide assessment scales [22]. Suicidal behaviour with an active drug is more likely to provoke concern than such behaviour with placebo. Finally, RCT dose regimens often fail to appreciate developmental pharmacokinetics of NGAs in children, therefore potentially contributing to reported safety and tolerability concerns [25], [80].
Youth depression: public health problem, ideological dispute, clinical dilemma
In the present controversy, different public health interests are pitted against each other. In responding to youth depression and rising suicide rates, governmental, medical and psychiatric bodies have emphasized the hazards of untreated depression. This remains pertinent even though suicide rates moved downwards from the late 1990s. This response, however, encountered growing concerns regarding pharmaceutical company influence in researching and marketing drugs and in promoting illnesses to patients, prescribers, governments and regulatory bodies.
There have been complaints about publication bias (approximately 50% of paediatric depression studies were unpublished, and all had negative results [19]); pharmaceutical funding to authors of studies and clinical guidelines; and failure of regulators to act [74]. Authors of antidepressant trials have been criticized for consistently exaggerating or ‘cherry-picking’ data on benefits, and downplaying risks [17]. This mirrors a wider debate about the medicalization of unhappiness, the social origins of depression, and the role of therapeutic drugs in society and with children [49], [74], [81–83].
Regulatory advice may also ignore some clinical realities. The TGA notes that ‘the marketers of fluvoxamine and sertraline (indicated for OCD) advise against use in children and adolescents with MDD, and of citalopram, escitalopram, paroxetine, venlafaxine and fluoxetine warn or caution against use in patients aged less than 18 years for any indication’ [68]. It has approved sertraline and fluvoxamine for use in OCD in children, and the older tricyclics amitriptyline and imipramine for nocturnal enuresis, but no antidepressant for childhood depression or anxiety. Similarly, the UK's CSM resolved that only fluoxetine shows a favourable risk–benefit ratio in paediatric depression [84]. Yet comorbidity is an unavoidable clinical reality [85]. Unsurprisingly, most child and adolescent psychiatrists and many paediatricians regularly use NGAs for treating mood, anxiety and OCD. In the USA, where most child NGA prescriptions are for anxiety disorders and the FDA approves fluoxetine only for adolescents with mood disorders, prescribers prefer off-label drugs such as sertraline [86]. The authors have sought information regarding child NGA prescriptions from Medicare Australia, but this is not available in the public domain.
While the black-box warnings denoted extremely serious risk, the clinical trial data were underpowered for detecting small risk differences (particularly for individual drugs), so their translation into risks for clinical practice is complicated. Among 4582 FDA patients there were no completed suicides.
For these reasons the warnings were contentious: many feared that they would discourage diagnosis and treatment especially by generalist practitioners [13], [87]. This may have now happened [88]. Recent US and Netherlands data show rising suicide deaths coinciding with reduced antidepressant prescribing [35].
What are the risks of no treatment?
The debate to date has largely considered the risks of treatment. Evidence regarding the risks of no treatment is discussed less often, or has only newly emerged.
RCTs clarify the question of efficacy (i.e. whether treatments improve outcomes under controlled conditions), not effectiveness (i.e. the effects of treatment on health outcomes approximating usual care) [89]. One cannot conduct clinical trials that have suicide as an outcome for ethical reasons, and because RCTs are not designed to investigate rare events such as suicide or attempted suicide [16]. Observational studies, although they may be more prone to bias and confounding than RCTs [12], are also required [90]. Studies with much larger adolescent samples conclude that antidepressants reduce risk for suicide attempts, which is highest in the month before starting an antidepressant, and steadily declines with length of treatment [91], [92]. Five observational studies show that child and adolescent suicide is associated with a complete or substantial relative absence of antidepressants [4–8]. A Finnish cohort study of hospitalized non-psychotic suicide attempters found that current use of any antidepressant was associated with a markedly increased risk of attempted suicide, and also a markedly decreased risk of completed suicide and death [93]. Last, an ecological analysis of the relationship of suicide and SSRI prescriptions across 27 countries over time that controlled for many confounding variables within and across countries reported a strong inverse relationship between antidepressant prescriptions and suicide for those aged 15–24 years [10]. A recent US analysis confirms this [9]. The latter consistent correlations across space and time are not causations (e.g. there may be a relationship with progressive mental health programmes), but they reduce the plausibility of valid competing explanations.
Antidepressant treatment guidelines
What do clinicians make of this? Clinicians have long recognized, and research confirms, that suicidal behaviour may be elevated during the first month of TCA or NGA treatment (although this was not replicated in the paediatric trial data [3]) [5], [94]. This may simply mean that antidepressants are being prescribed for the right indication [95]. The FDA strongly suggest that in some children and adolescents the starting of SSRIs can induce agitation or akathisia, ‘suicidality’, irritability and aggressive behaviour. Cessation, or increasing or decreasing the dose, may also be risk times [1], [3]. Also, like other antidepressants, NGAs may induce emotional blunting (a subjectively disconcerting absence of affect) and manic switches, especially in cases of bipolar depression, with altered or unstable mood [96]. How common these side-effects are with NGAs, and their relationship with suicidality, is unclear. Regarding suicidality, the role of withdrawal side-effects (due to poor adherence or short half-life), susceptibility to side-effects (e.g. due to slow metabolism), NGA dosage, type and half-life, time during treatment, and severity of disorder, also require clarification [1], [18], [55].
Given the frequent conjunction of depression (treated or untreated) and suicidal behaviour in youth, it is not surprising that depressed youth taking NGAs may become suicidal. Several hypotheses are possible. One is that NGAs generate, intensify or disinhibit suicidal ideas, emotions and behaviours. Another is that NGAs’ effects on depression may be delayed, partial or absent. A third is that NGAs through clinical improvements or having more side-effects than placebo, may increase reporting of existing suicidal feelings or behaviour [23], [24], but NGAs, by effectively treating depression, may also reduce suicide. This paradoxical finding [93] may be partly explained by noting that although those with suicidal thoughts and attempts are at risk for suicide, most do not suicide, and their profiles differ somewhat from those who suicide [97].
The Australian Adverse Drug Reactions Advisory Committee (ADRAC) judged that SSRI use in children and adolescents with MDD and other psychiatric conditions should occur only within comprehensive patient management [68]. The Joint Colleges of Psychiatry, General Practice, and Physicians recommended that children and adolescents continue to access these medications, and observed that ‘not treating depression is more likely to result in harm than is the appropriate use of antidepressants’ [98].
The UK NICE guidelines that recommend psychological treatments should always be the first line of treatment for depressed and suicidal adolescents, and medication offered only when psychological treatments (4–6 sessions) have failed. This does not accord with recent evidence [99]. Combination fluoxetine and CBT may be most effective for moderate or marked depression, and fluoxetine for more severe depression [52], [53]. CBT and interpersonal psychotherapy are effective, but for how long requires clarification [54], [100]. Neuroimaging suggests that antidepressants act on different brain sites than psychotherapeutic approaches [101]. Their relief of mood, anxiety and neurovegetative symptoms may enable patients to use psychotherapy [102]. Also, maldistribution of mental health workforces may mean that psychotherapy is not available.
An algorithm for NGA use that reflects evidence at time of writing is presented in Table 1. Mild depression (as per DSM-IV) without serious risk warrants regular review, capitalizing on significant remission rates without treatment, and may require psychoeducation, self-care strategies, and/or specific psychotherapies [100]. But NGAs should be used if mild depression persists or if depression is moderate to severe. They should be accompanied by lucid information geared to the patient's level of enquiry, appropriate cautions, early and frequent reviews, and psychological treatments. Like all interventions, they require thorough assessment (with family and school involvement as appropriate), identification and treatment of comorbid conditions, and a supportive therapeutic relationship [55]. Understanding the circumstances of adolescents and their attitudes to mental health problems, services, professionals and medications is critical to engagement, effective treatment and adherence. Barriers to trust, such as consent for treatment and confidentiality, also require attention.
Antidepressant use and the management of adolescent depressive disorders
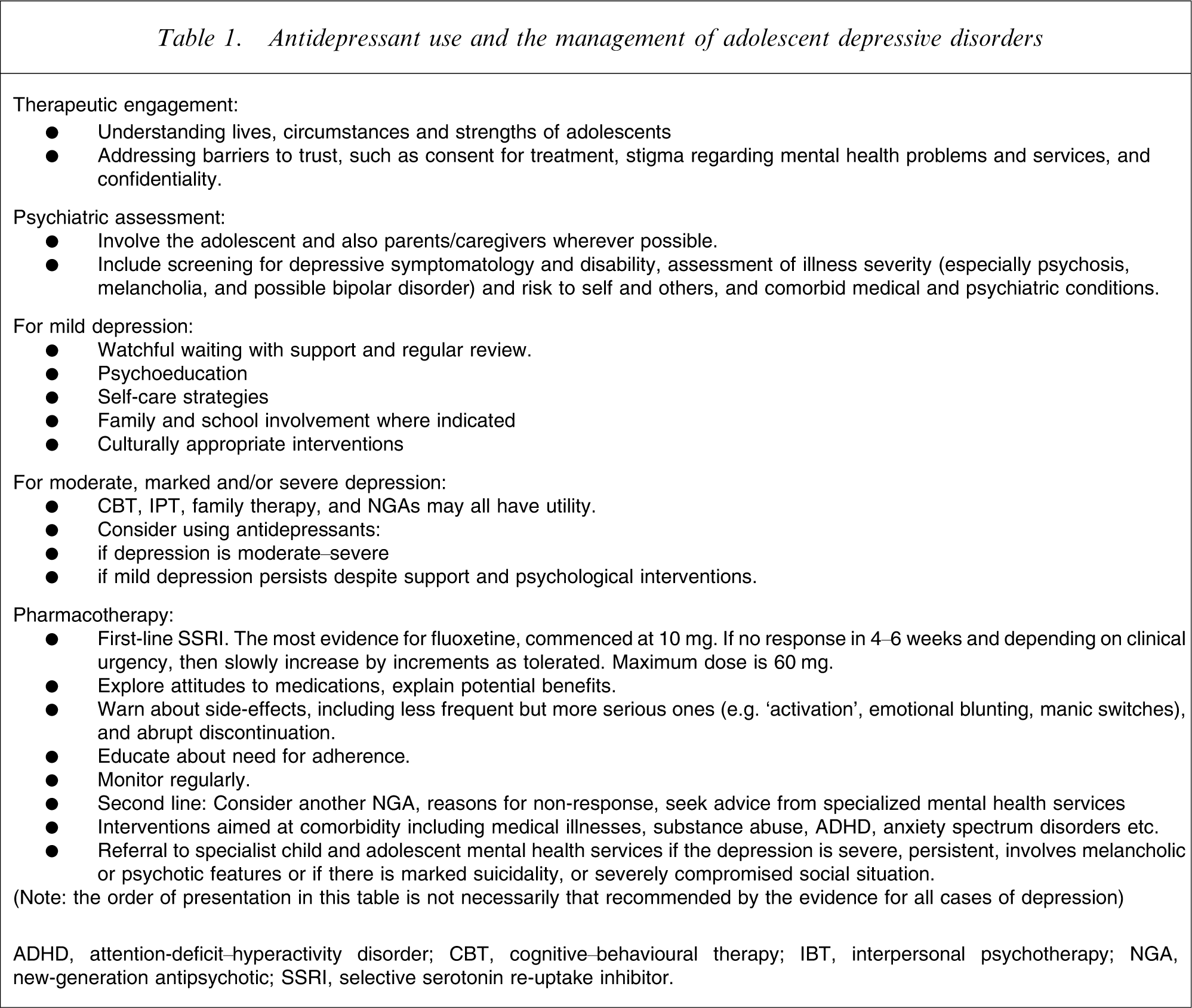
ADHD, attention-deficit–hyperactivity disorder; CBT, cognitive–behavioural therapy; IBT, interpersonal psychotherapy; NGA, new-generation antipsychotic; SSRI, selective serotonin re-uptake inhibitor.
NGAs are frequently well tolerated. Their side-effects are dose dependent and may subside with time (e.g. dizziness, nausea, anxiety, diarrhoea, asthenia, tremor, sweating, insomnia or somnolence, and sexual dysfunction). But clinicians should be vigilant concerning these less frequent but serious symptoms. Withdrawal or discontinuation symptoms, commonly characterized by dizziness, nausea and anxiety, may be avoided by tapering the dose. Switches between antidepressants should follow guidelines from appropriate sources [103]. Clinicians should also be aware of the rare increased propensity for bleeding (surgical teams should be informed regarding NGA patients) and serotonin syndrome, seen with overdoses, amphetamine misuse and some drug interactions and idiosyncratic reactions, which is characterized by neuromuscular and autonomic hyperactivity and altered mental status. Venlafaxine may increase blood pressure and heart rate, while mirtazepine may cause increased appetite, weight gain and somnolence, and may be used to treat insomnia [102].
Prior to commencing NGAs, patients and parents where appropriate should be given the foregoing rationale, and information about mode of operation and side-effects, including possible suicidal thoughts and behaviour. They should be told that all NGAs are off-label for depression in Australia. Questions about potential addiction may be answered by stating that antidepressants do not create chemical tolerance, but they may be associated with withdrawal symptoms. Responses and side-effects, including suicidal thoughts, should be noted throughout treatment. Daily scoring of mood and suicidality may be useful. Adverse events should be reported to drug review committees.
Because fluoxetine is most demonstrably effective, it should be used first unless otherwise indicated. No dose-response studies exist, so a low starting dose (10–20 mg) is advisable. Children may need less than adolescents [80], and early initial review (1–2 weeks) is warranted. If response is inconclusive and side-effects are not limiting, then one should slowly increase in increments, allowing time for response. An adequate trial lasts at least 4 weeks at the minimum effective dose [102]. Some patients may require 60 mg [54], [104].
If fluoxetine is not successful, NGAs such as sertraline or citalopram and/or CBT may be considered [105]. Reasons for response failure should be systematically examined [55]. Small open studies and adult RCTs may support lithium and T3 augmentation respectively. ECT or antipsychotics may also be considered in severe or psychotic mood disorders [55], [106]. There are no published RCTs of transcranial magnetic stimulation.
Clinicians should appraise potential NGA interactions with other medications, especially those metabolized by hepatic CYP-450 enzymes (websites with current information include http://medicine.iupui.edu/flockhart, http://www.preskorn.com, and http:///www.pdr.net [103]).
Of particular importance is to identify possible bipolar depression. Symptomatic diagnosis can often be difficult, but early onset, psychosis, pharmacologically induced mania/hypomania and family history of bipolar illness add weight to this [105]. Young people with this condition may be more likely to show suicidal behaviour, manic switching, and may benefit from mood stabilizers [103]).
Any patient not responding to an initial NGA trial, with severe or complex depression or suicidality, or a seriously compromised social situation should probably receive consultation from or be referred to mental health services or a child and adolescent psychiatrist.
Illnesses such as depression and OCD are chronic, recurrent illnesses, continuous with adult disorders, yet information predicting relapse and longer term efficacy and safety of antidepressants is minimal [25]. Expert opinion suggests continuing NGAs for 6–12 months to achieve full remission and avoid relapse [54], [107]. More and severer episodes, longer recovery times, comorbidities and cumulative risk factors should indicate the need for longer treatment [52], [55].
Conclusion
Meta-analyses in recent years noted comparative lack of efficacy for NGAs, and also suicidality and other hazardous effects in a small group of child and adolescent patients. This may be particularly so with children, whose pharmacokinetics are undeveloped compared with adults. But other recent RCTs and more comprehensive meta-analyses conclude that NGAs are effective in depression especially of moderate–severe intensity, and benefits outweigh risks. Observational studies provide converging indirect evidence of NGA effectiveness, which must now be considered likely to overall prevent youth suicide, even if NGAs may increase the risk of youth suicidality (e.g. [1], [5]), a risk that probably reduces with length of treatment [92].
Much is still unknown about ‘suicidality’ and its correlates with NGAs. Further NGA research must rely on clinical trial registers to avoid publication bias. Psychological treatments need more research and dissemination strategies. Better evidence is required regarding clinical practice and longitudinal trends.
The pendulum has not merely swung to the opposite pole. Noting regulatory warnings, clinicians must weigh risks of treatment and no treatment. Patients should be consulted about this complex condition. Its commonness, chronicity, and the uncertainty of relapse prediction argue for assertive, continuing treatment that maximizes patient safety. In moderate–severe depression the risk of NGAs may be less than that of suicide if they are not used.
Footnotes
Acknowledgements
This research was supported by NHMRC Program Grant 510135. Thanks to Bob Goldney and Jon Jureidini for robust debates about evidence, thanks to Joseph Rey and two anonymous reviewers for their conceptual input and their critiques, and to our patients, whose concern about this issue prompted this review.