
Abstract
Short-term psychodynamic psychotherapy (STPP) is a widely practised form of psychological intervention. Given that the Roth and Fonagy (1996) review concluded that there was a lack of confirming evidence for STPP, the current review is focused on studies published between 1996 and 2006 that evaluate the efficacy of STPP. As a result of a systematic literature review, 18 studies were found that met inclusion criteria consistent with those used by Roth and Fonagy (1996) for selection of studies, patient groupings and definition of therapeutic method. In general these studies add to an increasing body of evidence suggesting that STPP can be an effective psychological treatment for individuals experiencing mental health problems. Specifically, for depression STPP can be equal in effects to other psychological treatments and is significantly better than no treatment in the short term. Furthermore, emerging process data indicate that there is a significant relationship between the use of specific psychodynamic therapeutic techniques and the alleviation of depressive symptoms. Increasing evidence has emerged to support STPP as a treatment for generalized anxiety disorder, panic disorder and some personality disorders. There remains limited evidence for the use of STPP treatment for patients with anxiety disorders that relate more to stress. Very limited and inconclusive evidence currently exists to support STPP as a treatment for bipolar disorder, eating disorders and drug dependency. Future research needs to include broader assessment measures, long-term follow up, studies that maintain an identifiable focus, and research that includes a focus on psychotherapy process variables as they interact with outcomes.
Psychodynamic therapy continues to be a popular therapeutic approach among clinicians, with 14–40% explicitly subscribing to this orientation [1], [2]. But psychodynamic therapy is frequently criticized as lacking the evidence that would justify its use [3]. It is therefore notable that during the last decade high-quality empirical studies have been produced that respond to this deficit. The aim of the present review was to evaluate the efficacy of short-term psychodynamic psychotherapy (STPP) using a systematic literature review of studies produced in the decade 1996–2006. The review is structured so that findings can be used to inform the clinical use of STPP according to DSM-IV diagnostic categories.
Defining short-term psychodynamic psychotherapy
Psychodynamic practice today differs from traditional psychoanalysis in many ways, reflecting an attempt to increase its application and effectiveness for a wider range of patients [4]. The postulate of unconscious mental processes remains an underlying principle. Contemporary psychodynamic psychotherapy aims to elucidate a patient's unconscious conflicts, encourage the expression and resolution of disturbing emotional states, create conditions in which the patient gains insight, and explore predisposing factors arising from the patient's developmental history. These aims are achieved by focusing on current and past interpersonal relationships and via the therapeutic effects of the patient–therapist relationship, which is considered to be the core mechanism of therapeutic change [5]. For the purposes of this review, STPP is defined as an explicitly time-limited and focused therapy that clearly applies these concepts in its therapeutic techniques. Such a definition covers a variety of treatments that may be called psychodynamic psychotherapy and time-limited psychoanalytic psychotherapy in the literature. The short-term nature of the treatments reviewed is here defined as being a maximum of 40 sessions and a minimum of seven sessions; a definition used because it is the standard applied in previous meta-analyses [6], [7].
Previous reviews
In 1996 Roth and Fonagy concluded that there was a lack of evidence to clearly demonstrate that STPP was an effective psychological therapy [8]. At that time, many existing randomized controlled trials (RCTs) tended to use ‘psychodynamic therapy’ as an ill-defined comparison treatment to trial more recently developed therapies. But, based on studies with such methodological limitations, Roth and Fonagy did find a limited amount of evidence suggesting that STPP shows promise as a treatment of depression, post-traumatic stress disorder, eating disorders, personality disorders and interventions with children. After examining results for anxiety disorders, for example, the review was able to locate acceptable empirical support only for the treatment of post-traumatic stress disorder (PTSD). Roth and Fonagy found some evidence for the use of STPP in the treatment of eating disorders, with limited evidence suggesting the use of a manualized supportive–expressive (SE) psychotherapy for bulimic patients [8]. In the case of personality disorders the authors found only a small number of controlled studies with inconclusive results.
The empirical support for STPP had increased considerably by the time Fonagy et al. updated their review in 2005 [9]. In that paper they included all recent studies of psychoanalytic psychotherapy, this time also considering open trials. The authors discussed more than 50 studies that compared a variety of different psychodynamic treatments to other therapies or medication and compared individual treatments to having a combination of treatments. Results suggested that the greatest treatment efficacy was to be found when medication is used alongside psychotherapy. While the evidence is by no means compelling, the Fonagy et al. updated review suggested that outcomes of STPP therapy were comparable with those obtained by other therapeutic methods such as cognitive behavioral therapy (CBT), solution-focused therapy (SFT) and superior when compared to patients on a waiting list and treatment as usual [9]. Nine studies absent from their study will be included in the present review.
Leichsenring et al. conducted a meta-analysis of 17 RCTs of STPP used for specific psychiatric disorders for the period 1970–2004 [6]. That meta-analysis found significant effect sizes comparing pre-treatment and post-treatment measures for target problems (Cohen's d = 1.39), general psychiatric symptoms (Cohen's d = 0.90), and social functioning (Cohen's d = 0.80). These findings were stable over time and positive outcomes tended to increase at follow up. Further, they found large standardized mean differences between STPP on targeted problems as compared to waiting list controls and treatment as usual (Cohen's d = 1.17). Importantly, STPP did not differ as a treatment of targeted problems when compared to other psychological treatments such as CBT (Cohen's d = 0.04) and was found to be generally more effective than CBT at follow up (Cohen's d = 0.23).
The present review differs from previous ones in several ways. First, the review is focused specifically on short-term therapy as defined here. Second, because there has been considerable debate on the restriction of the evidence base for psychotherapies to RCTs, the current review adopts a broader definition. The evidence used in the present review is not limited to RCTs but also includes open trial investigations provided that they are replicable. The review also gives consideration to the interaction between therapeutic processes and outcomes [9], [10]. Although process studies do not in themselves establish evidence for the efficacy of a given therapy, such studies contribute to understanding the mechanisms that are associated with therapeutic change. The third major difference is that the present review is limited to trials published in the last decade, thereby creating an updated review of the most current evidence base for contemporary forms of STPP.
Method
The present review used inclusion criteria derived from Roth and Fonagy [8]. In order to be considered, study design required comparison of the treatment to a control condition or another treatment condition, preferably with randomization to the treatment groups. The present review also considered open trials. Process studies offer a valuable supplement to outcome studies and therefore were included [11]. To be included in the current review the study needed to clearly describe the therapeutic method and be of sufficient clarity to be used as a basis for clinical training. Preferably the description of therapeutic method was based on a published therapy manual. Patient groups to whom the treatment was applied were restricted to adult patients who presented with common mental disorders diagnosable using the DSM-IV-TR. Other criteria for studies to be included in the present review were that the therapeutic method must clearly fit the description of psychodynamic therapy as defined here.
Selection of papers
The following databases were examined for empirical studies that met the selection criteria: Academic Search Premier (EBSCOhost), PubMed, MEDLINE, PsyInfo, psycARTICLES, psycInfo, ProQuest Dissertation Abstracts, and Digital Thesis Program (Australasian and International). The following electronic resources were explored: Wiley Interscience, Psychoanalytic Electronic Publishing (PEP) as well as meta-analyses conducted by the Cochrane Library and Campbell Collaboration. Key texts and citations from peer-reviewed publications were also accessed. The following search words were used: psychodynamic, psychodynamic psychotherapy, short-term psychodynamic, time-limited psychodynamic, short-term dynamic psychotherapy, outcomes psychodynamic, trials psychodynamic, and, where extended criteria were required, the term ‘psychotherapy’ was used.
Results
General characteristics of studies under review
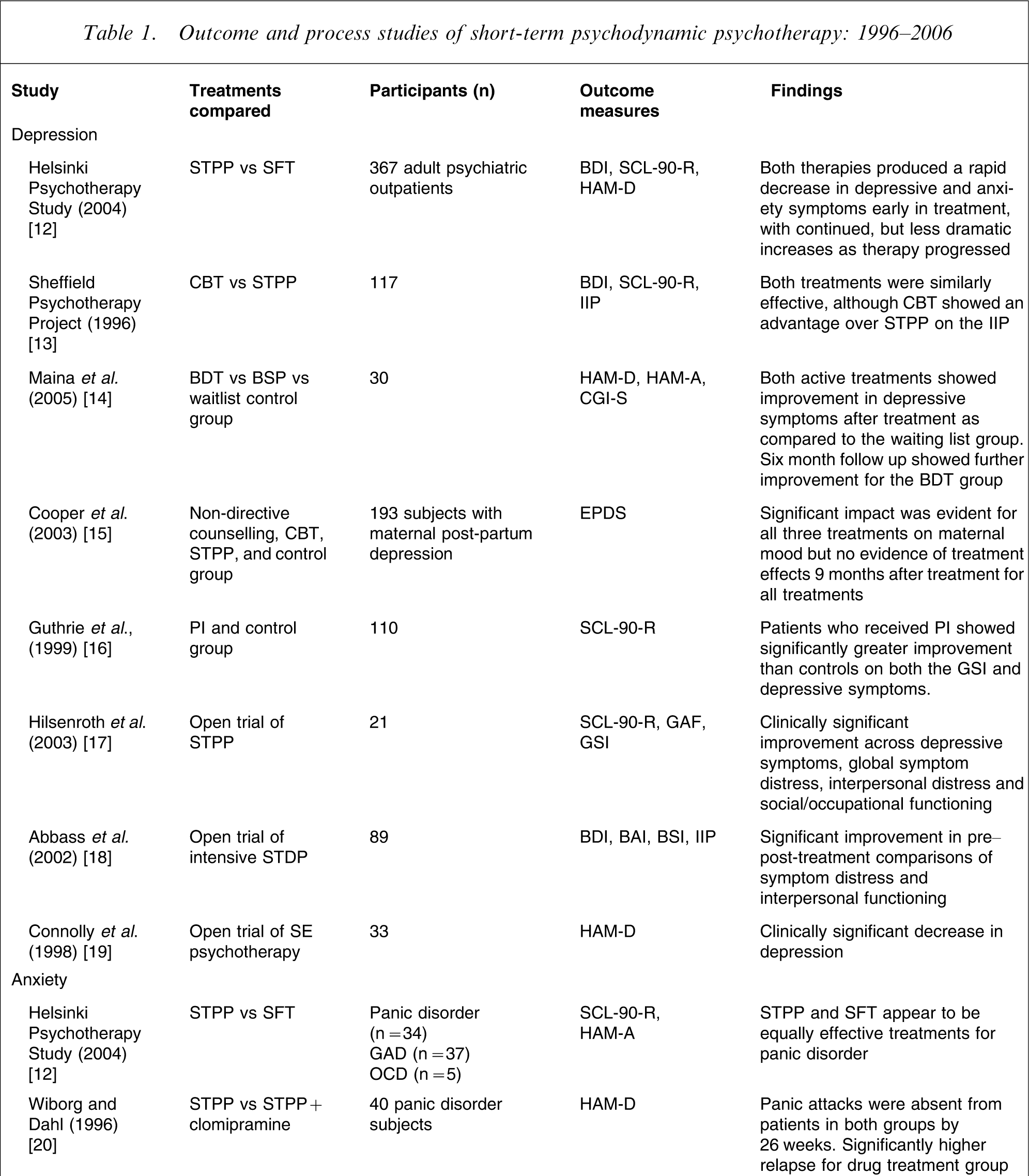
Eighteen studies satisfied the inclusion criteria. A summary of these studies is presented in Table 1. Fifteen of these studies were outcome focused and three were process focused. Results of studies were separated into the diagnostic categories that were the focus of the treatment and are discussed separately when a single study covered more than one diagnostic category.
Outcome and process studies of short-term psychodynamic psychotherapy: 1996–2006
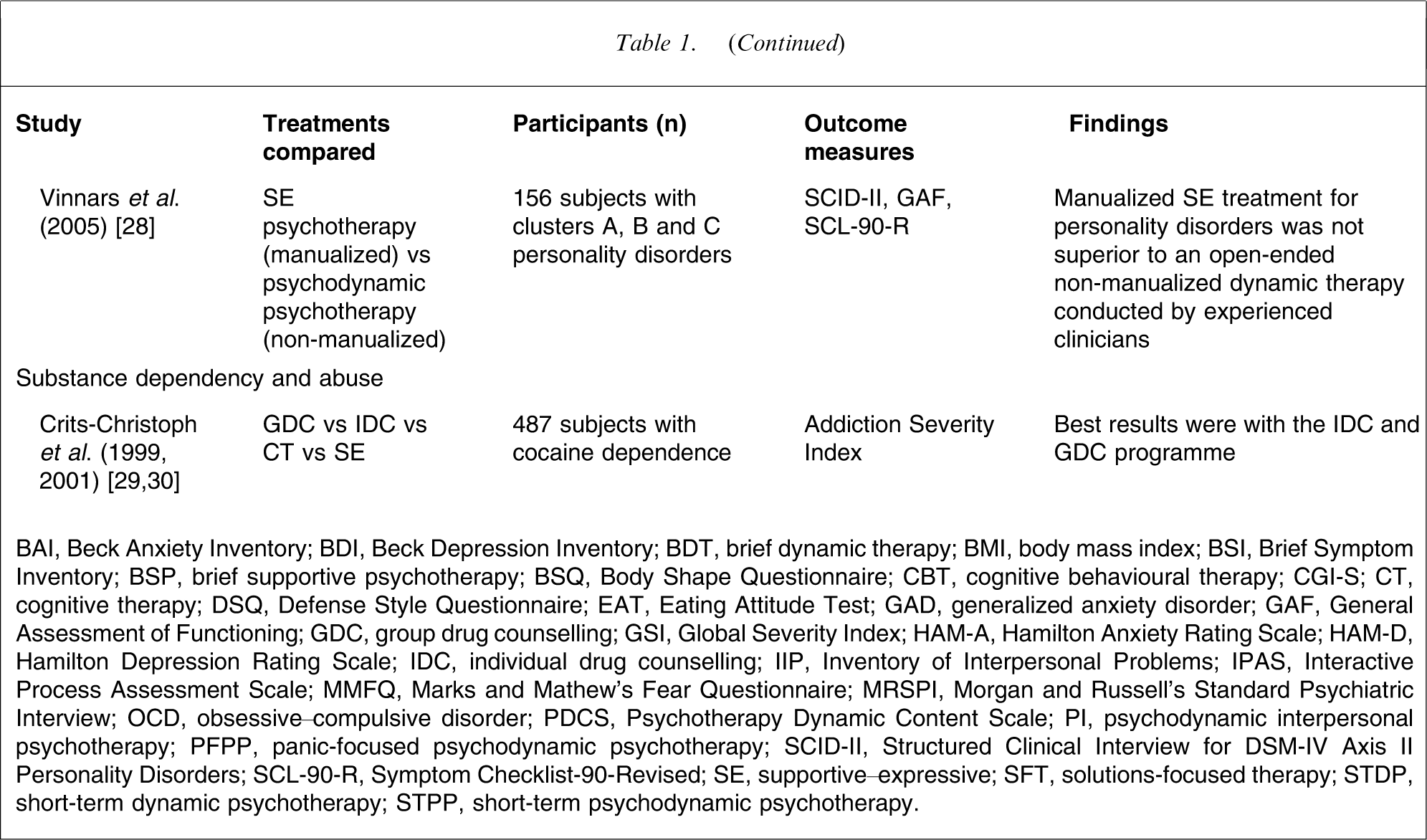
BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; BDT, brief dynamic therapy; BMI, body mass index; BSI, Brief Symptom Inventory; BSP, brief supportive psychotherapy; BSQ, Body Shape Questionnaire; CBT, cognitive behavioural therapy; CGI-S; CT, cognitive therapy; DSQ, Defense Style Questionnaire; EAT, Eating Attitude Test; GAD, generalized anxiety disorder; GAF, General Assessment of Functioning; GDC, group drug counselling; GSI, Global Severity Index; HAM-A, Hamilton Anxiety Rating Scale; HAM-D, Hamilton Depression Rating Scale; IDC, individual drug counselling; IIP, Inventory of Interpersonal Problems; IPAS, Interactive Process Assessment Scale; MMFQ, Marks and Mathew's Fear Questionnaire; MRSPI, Morgan and Russell's Standard Psychiatric Interview; OCD, obsessive–compulsive disorder; PDCS, Psychotherapy Dynamic Content Scale; PI, psychodynamic interpersonal psychotherapy; PFPP, panic-focused psychodynamic psychotherapy; SCID-II, Structured Clinical Interview for DSM-IV Axis II Personality Disorders; SCL-90-R, Symptom Checklist-90-Revised; SE, supportive–expressive; SFT, solutions-focused therapy; STDP, short-term dynamic psychotherapy; STPP, short-term psychodynamic psychotherapy.
Mood disorders
There is a growing body of quality research emerging to support the use of STPP as a treatment for depression. Of the eight studies identified, four studies were focused specifically on the treatment for patients with unipolar depression. There has been little current research into STPP for patients with bipolar disorder during the past decade. The small sample sizes in these studies and lack of data specific to this disorder make the results for the use of STPP for the treatment of bipolar disorder inconclusive.
The Helsinki Psychotherapy Study used a randomized design to compare the effects of four different forms of psychotherapy as a treatment of depressive and anxiety disorders [12]. Treatments studied were SFT, STTP, long-term psychodynamic psychotherapy and psychoanalysis. SFT has its conceptual origins in systemic family therapy and operates by identifying a focal problem and confining the therapy to finding a solution to this problem within the context of a positive working alliance. Finnish adult psychiatric outpatients (n = 367) were recruited who met DSM-IV criteria for depressive and anxiety disorders during a 6 year period. Results for STPP and SFT were available and these indicated that both treatments produced a rapid decrease in depressive and anxiety symptoms early in treatment, with continued, but less dramatic, increases as therapy progressed. Of the 82% of patients diagnosed with a mood disorder at baseline, 30% no longer met diagnostic criteria by the 7 month follow up and improvements continued at the 12 month follow up. There were no statistically significant differences between the two forms of treatment on outcome measures of depression. Knekt and Lindfors conclude that although both forms of treatment can be effective in clinical practice, neither can be relied upon to produce recovery in all patients [12]. Although that study was thorough and comprehensive, it is limited because the STPP treatment was not fully manualized, therapist level of adherence was not recorded and follow up beyond 12 months is not currently available.
The Sheffield Psychotherapy Project studied the effects of CBT and STPP on patients with a diagnosis of major depression [13]. Patients (n = 117) were randomly assigned to either eight or 16 sessions of CBT or STPP. Overall results showed both treatments to be similarly effective, although CBT showed an advantage over STPP on the Inventory of Interpersonal Problems. Results found that at 1 year follow up, patients who had received eight sessions of CBT had maintained improvements more than those who had received eight sessions of STPP. But for those receiving 16 sessions the results for both treatments were similar. For both treatments, patients who received 16 session treatments had greater improvement than patients who received eight sessions. Findings also suggested that patients with more severe symptoms of depression required longer treatment. These findings imply that eight sessions of STPP may be an insufficient intervention for the treatment of major depression.
Maina et al. conducted an RCT comparing brief dynamic therapy (BDT) and brief supportive psychotherapy (BSP) with a waitlist control group in the treatment of minor depressive disorders for 30 patients [14]. Assessment was conducted before and after treatment and at 6 months follow up for the two treatment groups and at 9 months after admission into the study for the waiting list group. Both BDT and BSP patients recorded a significant improvement in depressive symptoms after treatment on all rating scales as compared to the waiting list group, who showed no change. Results at the 6 month follow up showed further improvement for the BDT group on all measures. The authors concluded that BDT is a promising treatment for patients with minor depressive disorders and that BDT is more effective than BSP for patients with minor depressive disorders in the longer term. This is a well-designed study but, as the researchers acknowledge, longer term follow up and a larger sample group would be required in a replication study.
In a controlled trial for the treatment of maternal post-partum depression Cooper et al. randomly assigned 193 women to one of four conditions: non-directive counselling, CBT, psychodynamic therapy and routine primary care (control group) [15]. The aim of that study was to examine the impact of three forms of psychological treatment on maternal mood compared to a control group. Assessments were made at the end of treatment (4½ months), then at 9, 18 and 60 months follow up. Results recorded at the end of treatment showed a significant impact of all three treatments on maternal mood, as measured by the Edinburgh Postnatal Depression Scale. Psychodynamic treatment created a greater decrease in depression than the control group, but results indicated that there was no evidence of treatment effects 9 months after treatment for all treatments. These results indicate that STPP is equally useful in improving maternal postnatal mood disorders in the short term but equally ineffective in the long term.
Guthrie et al. conducted a controlled trial of 110 patients, randomly assigning 55 patients to psychodynamic interpersonal psychotherapy (PI) and 55 patients to a treatment-as-usual control group [16]. The study was aimed at measuring the cost-effectiveness of PI for high users of psychiatric services who had enduring non-psychotic symptoms and who were not helped by other treatments and who were usually considered to be difficult-to-treat patients. Eighty-three patients received an ICD-10 diagnosis of unipolar mood disorder. Patients received eight sessions on a weekly basis. The therapy model was manualized and adherence was monitored. A battery of measures was used throughout the treatment and at a 6 month follow up. Results indicated that patients who received PI had significantly greater improvement than controls on both the Global Severity Index and the depressive subscale of the Symptom Checklist-90-Revised (SCL-90-R) at the 6 month follow up. PI-treated patients had statistically significant improvement for social functioning at the 6 month follow up and improved quality of life compared to the controls. The findings suggest that PI is a promising treatment for this group of patients and that a substantial reduction in health-care use and costs can be achieved in the 6 months following such treatment.
An uncontrolled trial by Hilsenroth et al. recruited a patient group of 21 who attended an average of 30 sessions over a 7 month period and received STPP for depression [17]. Results showed statistically and clinically significant improvement across depressive symptoms, global symptom distress, interpersonal distress and social/occupational functioning and large effects sizes. For the 71% who completed treatment, reliable change was recorded Reliable Change Index (RCI) > 1.96 while no patients showed deterioration during treatment. Although that study was limited by its small sample size, the authors claimed that these findings show that STPP produces effects that are comparable with other forms of psychological treatment of depression [10]. A unique feature of that study was its use of the Comparative Psychotherapy Process Scale [31] as a measure of the therapeutic process. Use of this measure found a strong association between psychodynamic–interpersonal technique and change in depressive symptoms (r = 0.57, p = 0.006).
Abbass evaluated the effectiveness and efficiency of intensive short-term dynamic psychotherapy (STDP) in a private psychiatric clinic [18]. The 89 patients recruited included patients diagnosed with both major depression (n = 38) and dysthymic disorder (n = 21). Results indicated significant improvement in pre–post-treatment comparisons of symptom distress and interpersonal functioning. Self-reported symptoms moved from the clinical to normal range after an average of 15 h of therapy. The author estimated cost savings to the heath-care system of more than $CAD400 000 in the 12 months after treatment. That study used a clear therapeutic method and included outcome measures of health-care utilization (length of stay in hospital before, during and after the treatment), medication changes and employment status. The study was limited due to it being carried out by the one therapist and the lack of control makes firm conclusions about the effectiveness for this treatment for specific disorders difficult to ascertain.
Connolly et al. conducted an open trial on patients (n = 33) with a diagnosis of major depression who were treated with 16 sessions of SE psychotherapy [19]. The aim of the trial was to evaluate the relationships between therapist interventions and treatment adherence in SE treatment. Results showed a statistically and clinically significant decrease in depression over the 16 weeks of treatment using the Hamilton Rating Scale for Depression with a very large effect size (Cohen's d = 1.91). The authors also suggested that increased therapist interpretations in early treatment can enhance outcomes [32].
Anxiety disorders
In 1996 Fonagy and Roth were unable to identify any methodologically satisfactory research into the effects of STPP for the treatment of anxiety disorders. In the past decade, however, there has been a considerable increase in the amount of research conducted into the use of STPP with this patient group.
The Helsinki Psychotherapy Study mentioned earlier included some patients diagnosed exclusively with panic disorder (n = 34), generalized anxiety disorder (n = 37) and obsessive–compulsive disorder (n = 5) [12]. Findings indicate clinically significant improvement in anxiety symptoms at 7 months and these were maintained through to the first year follow up. Both of the STPP and SFT groups recorded significant remission at the 7 month assessment point. At 7 months 56% of patients receiving STPP no longer met clinical criteria as compared with 42% for those treated with SFT. That study did not use a no-treatment control group and the comparison group also showed improvement. There was no statistically significant difference between the treatment groups, suggesting that STPP and SFT may be equally effective treatments for panic disorder. At 12 months follow up, a 34% decrease on the Hamilton Anxiety Rating Scale was recorded for patients treated with STPP and a 28% decrease for those treated with SFT, but again this difference was not statistically significant. Workability, personality functions, and social functioning were only slightly improved. Albeit based on small sample sizes, these findings suggest that STPP may be effective over the longer term for some patients presenting with anxiety disorders and that STPP can potentially offer rapid relief from anxiety symptoms.
In a controlled study, Wiborg and Dahl combined brief dynamic psychotherapy with drug treatment for patients diagnosed with panic disorder [20]. The patients (n = 20) received clomipramine for 9 months or clomipramine for the same amount of time combined with 15 weekly sessions of brief dynamic psychotherapy (n = 20). The results showed that panic attacks were absent from patients in both groups by 26 weeks following commencement of treatment, as measured by the Hamilton Rating Scale for Depression. When the drug treatment was terminated the relapse was significantly higher for the group who received only clomipramine. There were lower scores for most anxiety measures in the group with combined treatment at the 9 month follow up. This research shows promising results for the addition of BDT with clomipramine, compared with the drug treatment alone for panic disorder.
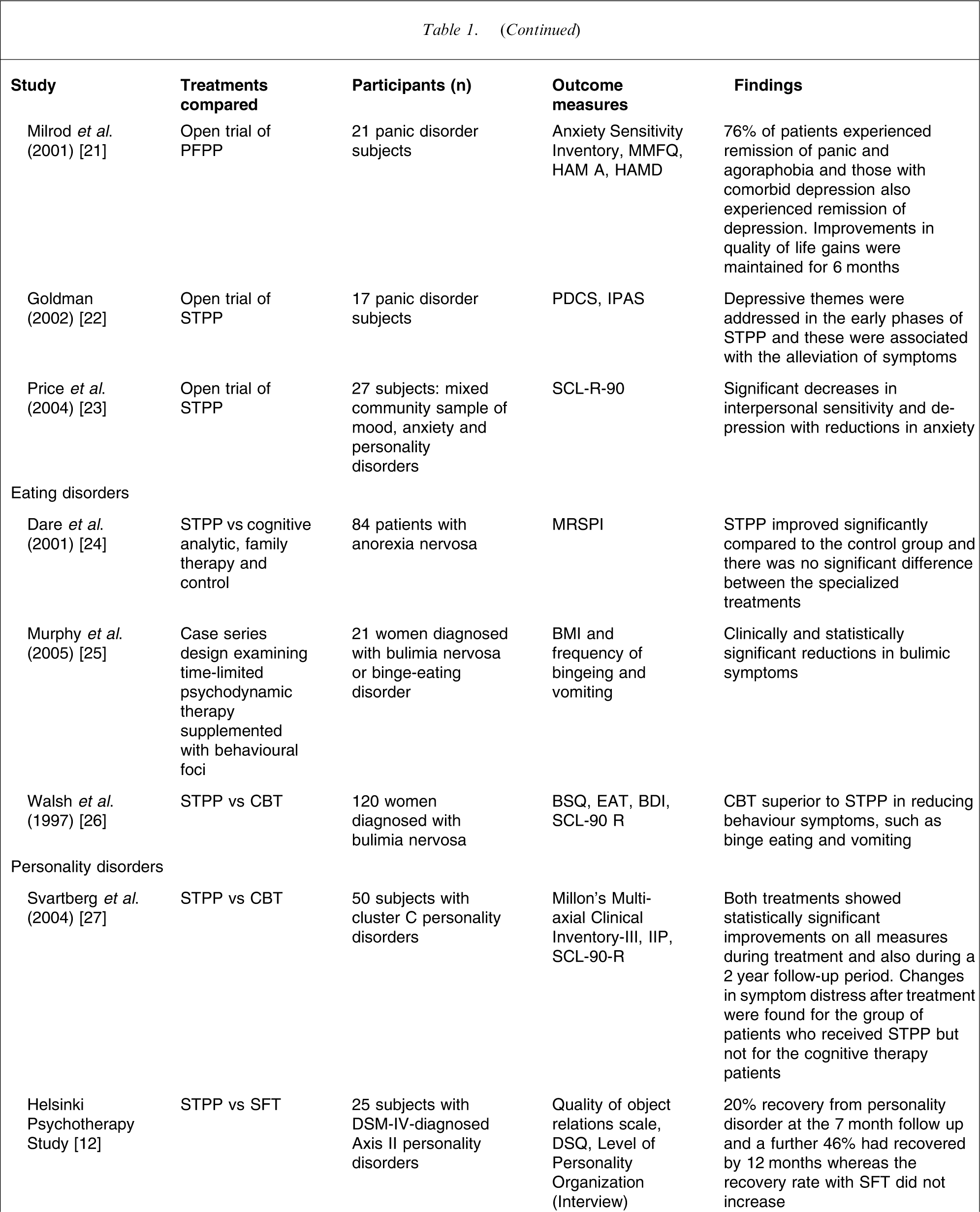
Milrod et al. conducted an open trial with a treatment designed specifically for panic disorder [21]. Twenty-one patients diagnosed with DSM-IV panic disorder were treated with a manualized treatment: panic-focused psychodynamic psychotherapy. Results showed that 16 patients (76%) experienced remission of panic and agoraphobia. Treatment completers with comorbid depression also experienced remission of depression. The researchers found that there were substantial improvements in quality of life that were consistent across all measures and that gains were maintained at 6 months follow up. Results showed clinically significant improvements across outcome measures of anxiety sensitivity, panic disorder severity, agoraphobic cognitions and body sensations with large within-group effect sizes. This research indicates that a well-structured STTP shows promise as a non-pharmacological treatment for panic disorder but requires further testing against proven treatments and controls.
There are also valuable process studies emerging that investigate the effective components in anxiety treatments. For example, in a study of the psychotherapeutic process in the treatment of comorbid conditions of depression and anxiety, Goldman studied 17 patients with a primary diagnosis of panic disorder [22]. Symptom severity measures as well as the Psychotherapy Dynamic Content Scale were used to measure process variables. Findings suggested that when depressive themes where addressed in the early phases of STPP these were associated with the alleviation of symptoms, adding to the investigation of underlying psychosocial and psychological factors in panic disorder. A further study using the Interactive Process Assessment Scale in research on the use of STPP for the treatment of panic disorder showed that interpretations delivered in the early phases of treatment can exacerbate symptoms, whereas transference interpretation later in treatment could be connected with symptom relief [33].
Price et al. conducted an open trial to assess the effectiveness of STPP for adults with a history of childhood sexual abuse (CSA) [23]. A total of 27 patients presenting to a university-based community outpatient setting included 12 with a history of CSA and 15 without such a history. The CSA group presented with both mood disorders (n = 9) and anxiety disorders (n = 4), and 58% (n = 7) also met criteria for a DSM-IV personality disorder. Treatment was informed by STPP treatment manuals and duration varied according to clinical judgement and treatment progress. The mean number of sessions was 26 sessions over a 6 month period. Following treatment, the CSA group reported significant improvements in symptoms according to the Global Severity Index of the SCL-90-R with a large effect size (Cohen's d = 0.83). The CSA group also had significant decreases in interpersonal sensitivity and depression, with reductions in anxiety also noted. The CSA patients were able to establish and maintain a positive therapeutic alliance equal to those with no history of sexual abuse. That study suggests that STPP shows promise as an effective treatment for adults who present with mixed high-prevalence disorders in the context of a history of CSA.
Eating disorders
Dare et al. conducted an RCT with 84 adult outpatients presenting with anorexia nervosa [24]. The patients were assigned to one of four different treatments: focal psychoanalytic psychotherapy, cognitive analytic therapy, family therapy or low-contact routine treatment (control). According to predetermined outcome categories, of the 17 patients who completed 1 year of the programme of focal psychoanalytic psychotherapy: three recovered, four improved significantly, four improved and six had a poor outcome. Results indicated that patients who received STPP improved significantly compared to the control group and there was no significant difference between the specialized treatments. Given that the group had a relatively poor prognosis (late age of onset, long duration of illness, history of unsuccessful treatment) focal psychoanalytic psychotherapy could be a valuable treatment for some adult outpatients with anorexia.
Two studies were found that examined the use of STPP as a treatment of bulimia. Murphy et al. used an integrated approach in which a psychodynamic approach was used in tandem with a behavioural focus (such as weighing in and monitoring of food behaviours), and showed limited efficacy [25]. But the study had methodological problems associated with unclear therapeutic method and an integrated approach. Walsh et al. found CBT to be superior to STPP in reducing behaviour symptoms such as binge eating and vomiting and that STPP did not appear to be of benefit for patients with bulimia [26].
Personality disorders
Svartberg et al. found that STPP showed promising results as a treatment for cluster C personality disorders [27]. Fifty outpatients meeting the criteria for one or more cluster C personality disorders and not for any other personality disorders were accepted into the study. Forty sessions of a manualized STDP were compared to the same amount of sessions of a cognitive therapy (CT). Both therapies were specifically designed to be treatments for personality disorders. Both treatments showed statistically significant improvements on measures of symptom distress, interpersonal functioning and personality pathology during treatment and also 2 years after treatment. Although the pattern of improvement following treatment was generally similar for both therapies, changes in symptom distress after treatment were large for the group of patients who received STPP (Cohen's d = 1.01) but only moderate for the CT patients (Cohen's d = 0.49). Given the small sample size and the considerable variation within follow-up scores, however, the difference between these effect sizes did not reach statistical significance. Two years after treatment 54% of the STDP patients and 42% of the CT patients had recovered symptomatically and approximately 40% of the patients in both groups had recovered in terms of interpersonal problems and personality functioning. Limitations of the study were an absence of a no-treatment group, lack of observer-rated measures and small sample sizes. But these results show that STDP is a promising treatment for at least cluster C personality types, and the post-treatment improvement suggests that the recovery patterns may differ according to the psychological treatment model used.
The Helsinki Psychotherapy Study, as earlier described, also treated 25 patients diagnosed with only a DSM-IV personality disorder [12]. Results for STPP treatment show that there was approximately a 20% recovery from personality disorder at the 7 month follow up and a further 46% had recovered by 12 months, whereas the recovery rate with SFT did not increase. These results add further support for there being enduring benefits for patients with personality disorders receiving STPP treatment.
Vinnars et al. randomly assigned patients to two STPP treatments (n = 156): SE psychotherapy (n = 80) and community-delivered psychodynamic psychotherapy (n = 76) [28]. The SE therapy was based on Luborsky's treatment manual [4], whereas the community-delivered approach was psychodynamically informed, but was not manualized. Personality disorders were grouped into clusters A, B and C as defined by DSM-IV. A battery of outcome measures including the Structured Clinical Interview for Personality Disorders and the SCL-90-R were used, along with a 2 year follow up to assess the persistence of treatment effects. The manualized SE treatment decreased the severity of personality disorders and psychiatric symptoms as well as improving functioning. Although the results for manualized SE treatment for personality disorders were promising, it was not superior to an open-ended non-manualized dynamic therapy conducted by experienced clinicians.
Substance dependency and abuse
Crits-Christoph et al. conducted a study into the use of STPP for the treatment of cocaine dependence [29], [30]. The study was designed to compare four treatments for cocaine-dependent patients: stand-alone group drug counselling (GDC), individual drug counselling (IDC), CT and SE therapy. By 6 months 39% of patients in the IDC and GDC group reported use of cocaine in the past month, whereas 57% of patients in CT and GDC, and 49% in SE and GDC reported use. Overall the four treatments showed significant improvement in cocaine use from baseline and in the 12 month follow up (p < 0.001), but the best results were achieved by the IDC and GDT programme (p = 0.02).
Discussion
The present review has identified 18 studies that satisfied the selection criteria. Overall eight studies found STPP to be equally effective to comparison psychological treatments; two studies found STPP to be less effective than other treatments for bulimia and cocaine additions, respectively; two studies found STPP to be more effective than other comparison treatments, both for personality disordered patients. Other results from the present review found five studies that showed STPP to be useful in bringing about substantial decreases in symptoms but which had no comparison group. A further four studies were process studies that identified significant relationships between specified psychodynamic techniques and improved patient outcomes.
The diagnostic groups of depression and anxiety provide the most promising results for STPP. No current studies into STPP for the treatment of depression found the treatment to be less effective than other therapies, four found it equally effective, one found it better than another treatment in the long term, and one found it better than treatment as usual. Two studies showed evidence that STPP is as effective as CBT in the treatment of depression. For anxiety, one study found STPP to be better than drug treatment alone and three showed a substantial reduction in symptoms. These results are encouraging compared with research for anxiety disorders, which a decade ago could identify only CBT as an evidence-supported therapy.
Rather than concluding that the general demonstration of equivalent outcomes in psychotherapy only demonstrates yet again the so-called dodo bird effect, careful examination of both superiority and inferiority of STPP is of great value. The Guthrie et al. finding that STPP is better than usual outpatient treatment for patients who are notoriously unresponsive to treatment [16] suggests an important addition for the management of this patient group. The Maina et al. finding that BDT for depression is superior to BSP at the 6 month follow up [14] suggests that different therapies may well have different patterns of post-treatment effects, which ought to be examined routinely for all outcome studies. Also, BDT combined with drug treatment was found to be useful in decreasing relapse in patients with panic disorder when compared to drug treatment alone [20], again suggesting that STPP may be more effective when combined with pharmacotherapy. In contrast, there continues to be a lack of evidence for the use of STPP as a treatment of eating disorders and substance abuse. These researchers suggest that focused drug counselling might be of benefit early on in treatment to address the drug use, and a more exploratory psychotherapy used subsequently to address the patient's vulnerability to relapse.
This review highlights the need for more reliable implementation of STPP in outcome research. Seven of the studies used in the present review were manualized and the others describe their clinical approaches as being guided by psychodynamic principles. Three of the studies did not indicate whether they were manualized. Nevertheless, when a manualized form of psychodynamic psychotherapy was compared with a non-manualized version there was no difference in the results [28], suggesting that the use of manualization may not have a negative impact on outcome per se. But clarity of definition of the therapy under consideration is as important for gaining methodological rigour in research as it is in the training of therapists. Although most of the studies considered training important, several lacked detail with regard to training or were unclear on this issue.
While most studies monitored the therapist adherence to the therapeutic model many did not measure this directly. Seven studies used scales specific to their intervention to measure therapist adherence, while two studies made no mention of adherence. Studies such as the Helsinki Psychotherapy Study, which did not use a manualized method, used the Working Alliance Inventory and Psychotherapy Process Assessment to measure details of the process in order to determine if these were psychodynamic in nature. In a similar fashion other studies used the Comparative Psychotherapy Process Scale.
In summary this review has identified 18 studies that have been produced during the past decade. There is an emerging evidence base that supports the use of STPP as a treatment of patients with depression. During the last decade STPP as a treatment for anxiety disorders in particular has been subject to extensive investigation. Although not yet conclusive, this accumulating evidence for STPP as a treatment of anxiety disorders does support further investigation. Generally speaking, methodological limitations continue to make firm conclusions about the effectiveness of STPP for specific disorders difficult to draw. Although there are an increasing number of studies that are increasingly sophisticated, further high-quality studies are required of STTP focused on specific clinical problems.
Footnotes
Acknowledgements
The current paper is based on the Master's dissertation of Michelle Dennerstein submitted in the School of Behavioural and Social Science and Humanities, University of Ballarat. Thanks are also due to Dr Jarrad Lum, Dr Megan Galbally, Dr Louise Hayes and two anonymous reviewers for their helpful advice and assistance.