
Abstract
Patient aggression in mental health inpatient settings poses a significant problem for both staff and patients [1]. Aggressive behaviour threatens the physical and psychological health of psychiatric nursing staff and patients and compromises the therapeutic environment of the unit. Further repercussions of patient aggression for staff and psychiatric services include increased absenteeism and sick leave, property damage, security costs, workers’ compensation, reduced job satisfaction, along with recruitment and retention issues [2]. Reducing patient aggression is a primary concern for psychiatric inpatient services.
Being admitted to a psychiatric inpatient unit is frequently associated with a high degree of stress and anxiety due to the controlled and confined nature of hospitalization and acute psychiatric symptoms, which can in turn exacerbate aggression. Pro re nata (PRN), or ‘as needed’ medications are prescribed for approximately 75% and administered to approximately 50% of psychiatric inpatients to reduce agitation and aggression [3–5]. These medications, usually benzodiazepines or antipsychotics, may be administered orally or by i.m. or i.v. injection. Some of the disadvantages of PRN medication regimens, however, include medication-related morbidity, polypharmacy, development of tolerance and/or withdrawal effects with prolonged use and potentially harmful drug interactions [4], [6].
Previous studies have shown relaxation massage therapy to be effective in reducing stress, anxiety and depression in a variety of psychiatric conditions, including bulimia [7], adjustment disorder and depression [8], [9]. In addition, in a group of aggressive adolescents a 20 min massage therapy session twice weekly for 5 weeks significantly reduced self-reported hostility and anxiety levels as well as level of aggression as perceived by the parents [10]. Other beneficial effects of massage therapy include enhanced immune function, increased mental alertness [11] and an improvement in sleep patterns [9].
This pilot study was conducted to evaluate the effect of massage therapy on measures of stress, anxiety, depression, irritability and hostility in young adult psychiatric inpatients and the impact of introducing a massage therapy programme on the incidence of violence and aggression on the unit.
Method
Setting
The present study was conducted at the ORYGEN Youth Health Inpatient Unit in Melbourne, Australia. ORYGEN Youth Health is the mental health service for young people aged 15–25 years living in the western region of Melbourne and incorporates the Early Psychosis Prevention and Intervention Centre (EPPIC). The 16-bed inpatient unit receives approximately 450 admissions per year. From July 2004 to June 2007 the average length of stay on the Unit was 11.06 days (median = 7.5 days, mode = 2 days). At any one time young people on the Unit have a range of diagnoses including schizophrenia, mania, depression and personality disorders. Four or five nursing staff are present on the unit at all times, giving a staff: client ratio of approximately 1:4. Management of patient aggression on the Unit includes behavioural approaches (e.g. time-out, distraction, limit setting and engaging with staff), administration of PRN medication and the use of seclusion and/or restraint where necessary.
Participants
Participants were all aged 15–25 years and were recruited from the ORYGEN Inpatient Unit. All young people recently admitted to the Unit were eligible for entry into the study except those patients who were highly agitated and aggressive and remained in an aggressive state for a prolonged period (>24 h) after admission to the Unit (as determined by treating staff). Patients admitted to the Unit for respite purposes were also excluded. To allow for a settling-in period, patients were invited to participate in the study after a minimum of 24 h following admission.
This study was approved by the North Western Mental Health Research and Ethics Committee. After complete description of the study, written informed consent was obtained from young people who met intake criteria and who were judged fully competent to give consent. For participants under 16 years of age, written consent was also obtained from a parent or guardian. Participants were able to withdraw from the study at any time and this decision did not influence the possibility of receiving treatment at ORYGEN Youth Health, or other services provided by the Victorian public health system.
Design
This was a single-site, non-blinded, non-randomized intervention study. Treatment as usual (TAU) and massage therapy intervention (MT) occurred over consecutive 7 week blocks and therefore inclusion to the treatment groups was determined by when an individual was admitted to the Unit. The TAU phase commenced on 22 May 2006 and ceased on 9 July 2006, while the MT phase commenced on 10 July 2006 and ceased on 27 August 2006. All young people who met study inclusion criteria were given information about the study and were invited to participate. Participants were assessed at baseline and prior to discharge from the Unit on a range of self-report and staff-rated measures as well as saliva cortisol levels, as outlined here. For MT participants a subset of these measures was also collected at the end of the initial and final massage therapy session. Unit data including the number of times PRN medication was administered, number of seclusions and number of days spent in intensive care assessment (ICA), were monitored during the study period. Aggressive incidents on the Unit were monitored using the Staff Observation Aggressive Scale–Revised (SOAS-R). Diagnoses according to the International Classification of Diseases (ICD-10) of all patients on the Unit during the TAU and MT phase were obtained from statistics routinely collected on the Unit.
Interventions
TAU included medication as appropriate, involvement in group-based activities on the Unit, individual counselling and therapy and educational activities if appropriate. Young people who agreed to inclusion in the MT intervention received TAU plus relaxation massage therapy daily during their period of hospitalization.
Massage therapy procedure
A qualified female massage therapist administered a 20 min standard massage procedure with the client sitting fully clothed in a special massage chair. The massage therapy session was based on a previously described method [10] and consisted of the following: (i) long, broad stroking with moderate pressure to the back, compression to the back (parallel to spine) from the shoulders to base of spine, gentle kneading to upper trapezius, gentle circular pressure with fingertips and heel of hand over shoulder area, light kneading to area of cervical vertebrae and circular pressure to occipital points at the base of the scalp; (ii) arms dropped to the side with arms kneaded from shoulder to lower arm and pressing down on upper and lower arms and deep stroking to anterior and posterior forearm; (iii) entire hands massaged and pulling of fingers, pressing down on trapezius with finger pressure, squeezing continuing down the arms. Natural Massage Balm (Pure Nature, Collingwood, Vic., Australia), containing no essential oils or scent, was applied to forearms and hands. All massage therapy sessions were performed by the same therapist and took place between 13.00 and 16.00 hours. As much as possible, for each patient, the massage therapy session occurred at the same time each day.
Outcome measures
All assessments were conducted between 13.00 and 17.00 hours at baseline and prior to discharge from the Unit. For participants in the MT group, assessments were performed immediately prior to the first and final massage therapy sessions. The Kennedy Nurses’ Observational Scale for Inpatient Evaluation (NOSIE) was used to assess patient irritability [12]. Nurses completed the irritability factor of the NOSIE, which consists of five items (e.g. gets angry or annoyed easily) followed by five choices regarding severity (0 = never to 5 = always). The time period assessed was the previous 48–72 h. Nurses were trained using Guide to the Kennedy NOSIE prior to rating participants. Participants then completed the hostility and depression items of the Symptom Checklist-90–Revised (SCL-90-R) [13] (participants were asked to indicate on a 5-point Likert scale their level of distress in response to simple statements such as ‘Having urges to break or smash things’) and the state component of the State-Trait Anxiety Inventory scale (STAI-S) [14] (20 items that measure transitory anxiety levels). Saliva cortisol samples were obtained by having participants chew on a cotton salivette over a period of 30–60 s (Sarstedt, Nümbrecht, Germany). The saliva samples were frozen and assayed for cortisol levels at a commercial laboratory (ARL Pathology, Melbourne, Victoria, Australia).
The immediate effect of massage therapy on anxiety, resting heart rate (HR) and saliva cortisol levels was also assessed following the initial and final massage therapy session. The STAI-S and HR were collected prior to and immediately after the first and final massage therapy sessions. HR was measured using the palpation method at the wrist (radial artery). The number of beats was counted over a 30 s period and multiplied by 2 to give the HR per min. Due to the 20 min lag time of cortisol, saliva was collected prior to and 20 min after the massage session in order to assess cortisol levels at the end of the session.
The nature, frequency and severity of aggressive incidents on the unit were monitored using the Staff Observation Aggression Scale–Revised (SOAS-R) [15]. The SOAS-R is a widely used instrument that has demonstrated good reliability and validity [16]. The SOAS-R was completed each time a staff member witnessed an aggressive behaviour by any patient on the Unit (not only those participating in the study). Aggression was defined as any verbal, non-verbal or physical behaviour that is threatening to the self, others, or property or physical behaviour that causes harm to self, others or property. The SOAS-R consists of five columns; column 1 provides information on the provocation that led to the aggressive incident; column 2 reports the means used by the patient during the incident (e.g. verbal, fist, chair, knife); column 3 records the target of the aggression (e.g. nothing, object, patient self, other patient, staff etc); column 4 records the consequences for the victims, ranging from no consequences to physical consequences requiring treatment by a physician; and column 5 records the measures taken to stop/control the aggressive behaviour (e.g. talking to patient, physical restraint etc.). The severity of the aggressive incident is calculated by summing the severity scores in each column (determined by a scoring system).
Statistical analysis
Data were analysed using statistical software SPSS for Windows 14.0 (SPSS, Chicago, IL, USA). Due to a significant proportion of participants lost to follow up, complete-case analysis was conducted. Independent sample t-tests and χ2 tests were used to compare demographic and baseline variables between groups. The effect of MT was compared with TAU using repeated measures ANCOVA with ‘days of hospitalization’ (as an index of illness severity) and ‘number of days between assessments’ as covariates. For analysis of saliva cortisol, ‘time of day (24 h) of saliva collection’ was included as an additional covariate. Participants in the MT group who missed more than 30% of their daily massage therapy sessions were excluded from the aforementioned analysis. Paired sample t-tests were used to compare differences between pre- and post-massage therapy variables in the entire sample of MT participants. Pearson's correlation was used to examine relationships between variables. All tests were two-tailed and significance was set at 0.05.
Results
Study sample
In total, 97 young people were admitted to the inpatient unit over the recruitment period; 47 met inclusion criteria and agreed to involvement in the study (48% of young people admitted to the unit over this period; Figure 1). Eighteen people agreed to inclusion during the TAU phase (22 May–9 July 2006) and 29 during the MT phase (10 July–27 August 2006). Three people were admitted to the unit twice during the MT phase and thus were included in the MT group twice. One person was admitted to the unit during both intervention periods and therefore was included in both the TAU and MT groups. Fourteen TAU participants (77.8%) and 22 MT participants (76.0%) completed the follow-up assessments. Four MT participants missed more than 30% of their daily massage therapy sessions and were therefore excluded from analyses. One of these participants spent a total of 13 days in ICA. The other three participants either declined or were on day leave and therefore did not receive a portion of their massage therapy sessions.
Study flow and dropout.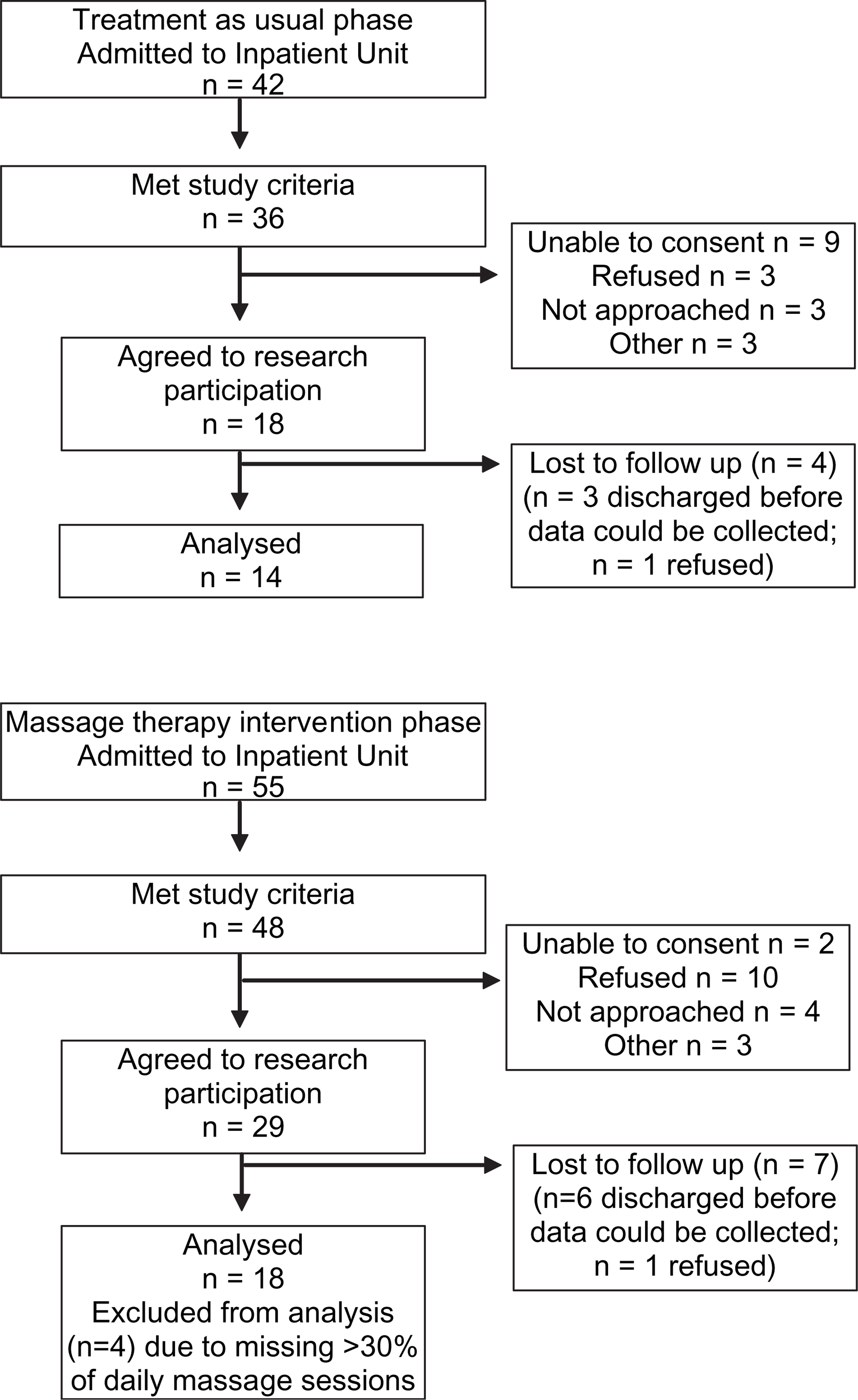
Baseline demographic and admission characteristics for the participants are shown in Table 1. There were no differences in gender or age between the two groups. A significantly higher proportion of the MT participants had been admitted to the unit involuntarily (61.4% vs 21.4%; p = 0.025). There was also a trend for differences between groups in the proportion of primary diagnosis at admission (p = 0.086). From observation, a greater percentage of MT participants had a diagnosis of bipolar disorder and borderline personality disorder. In contrast, the TAU group had a higher percentage of participants with non-affective and affective psychosis. There were also some differences in levels of substance use in the month prior to admission, in that there were significantly higher levels of amphetamine use (p = 0.015) and non-prescription use of sedatives such as benzodiazepines in the MT group (p = 0.027).
Participant sociodemographic and admission characteristics
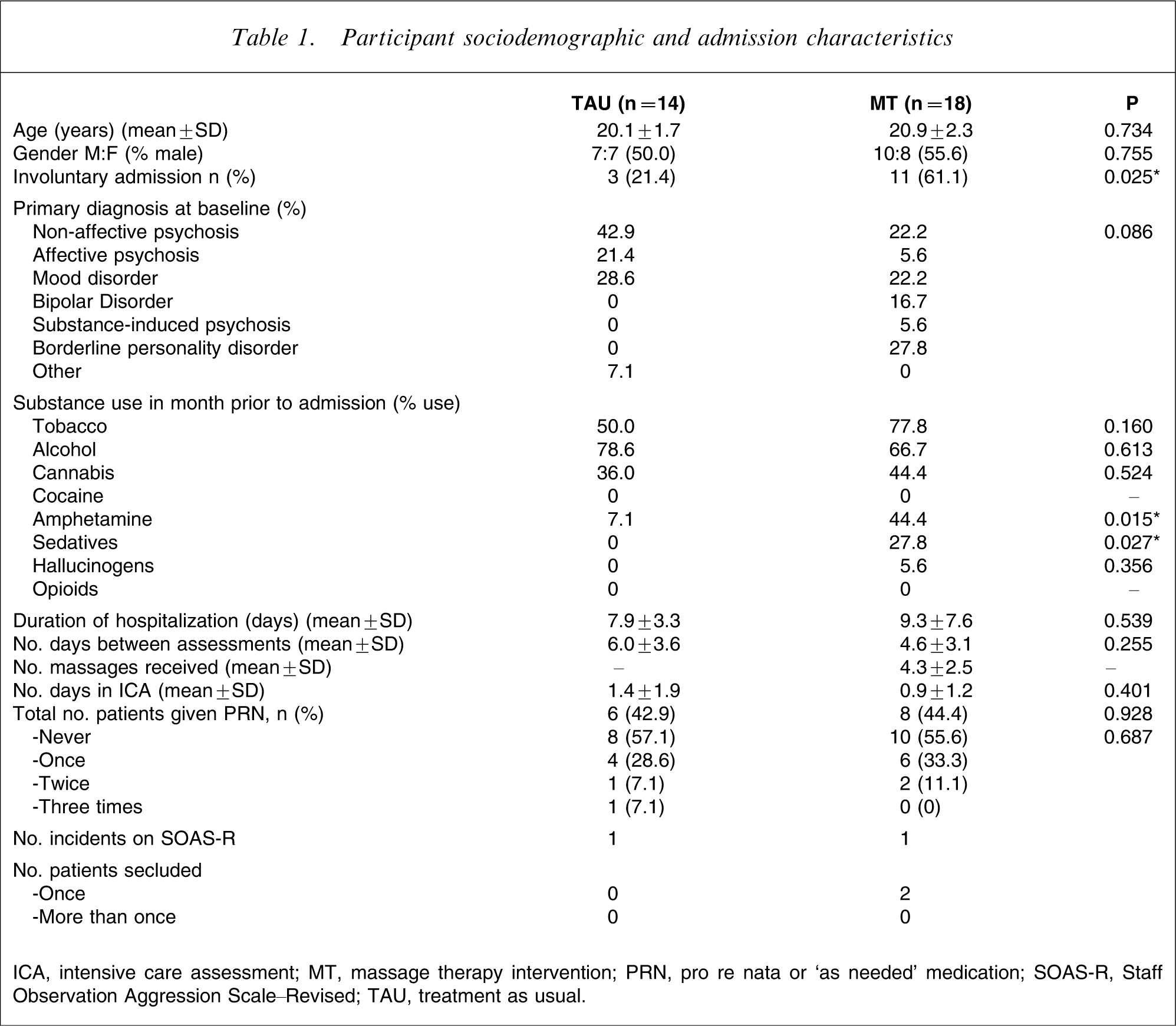
ICA, intensive care assessment; MT, massage therapy intervention; PRN, pro re nata or ‘as needed’ medication; SOAS-R, Staff Observation Aggression Scale–Revised; TAU, treatment as usual.
There were no differences between groups in the duration of hospitalization or the number of days between baseline and follow-up assessments. MT participants received on average 4.3 massage therapy sessions (range = 2–12; SD = 2.5) between assessments. There were no differences between groups in the number of days spent in ICA or the amount of PRN medication administered. One participant in each treatment group had an aggressive incident that was recorded on the SOAS-R. Two MT participants were placed in seclusion on one occasion during the study period. No TAU participants were placed in seclusion (Table 1).
Patient outcome data
Baseline and follow-up responses to the NOSIE, SCL-hostility and depression subscales, STAI-S and saliva cortisol levels in TAU and MT participants are shown in Table 2. There was no group×time interaction on any of the measures (p > 0.3). There was no main effect of time on the NOSIE scores (F(1,26) = 1.62, p = 0.22), but there was a trend for a main effect of group (F(1,26) = 4.01, p = 0.056). MT participants tended to have higher NOSIE scores than TAU participants. There was a significant reduction in the SCL-hostility and depression subscales scores over time in both groups, as shown by a main effect of time on SCL-hostility (F(1,28) = 8.56, p = 0.007) and SCL-depression scores (F(1,28) = 25.90, p < 0.001). There was no main effect of group on either SCL-hostility (F(1,28) = 1.61, p = 0.22) or SCL-depression scores (F(1,28) = 0.07, p = 0.80). In the MT group there was no correlation between number of massage therapy sessions received and the change in SCL-hostility or depression scores between assessments, indicating no treatment dose effect. There was no main effect of time (F(1,28) = 1.44, p = 0.24) or group on STAI-S scores (F(1,28) = 0.02, p = 0.90). Finally, analysis of saliva cortisol levels revealed no main effect of time (F(1,23) = 0.14, p = 0.71) or group (F(1,23) = 0.39, p = 0.54).
Clinical measures at baseline and follow up (mean±SD)
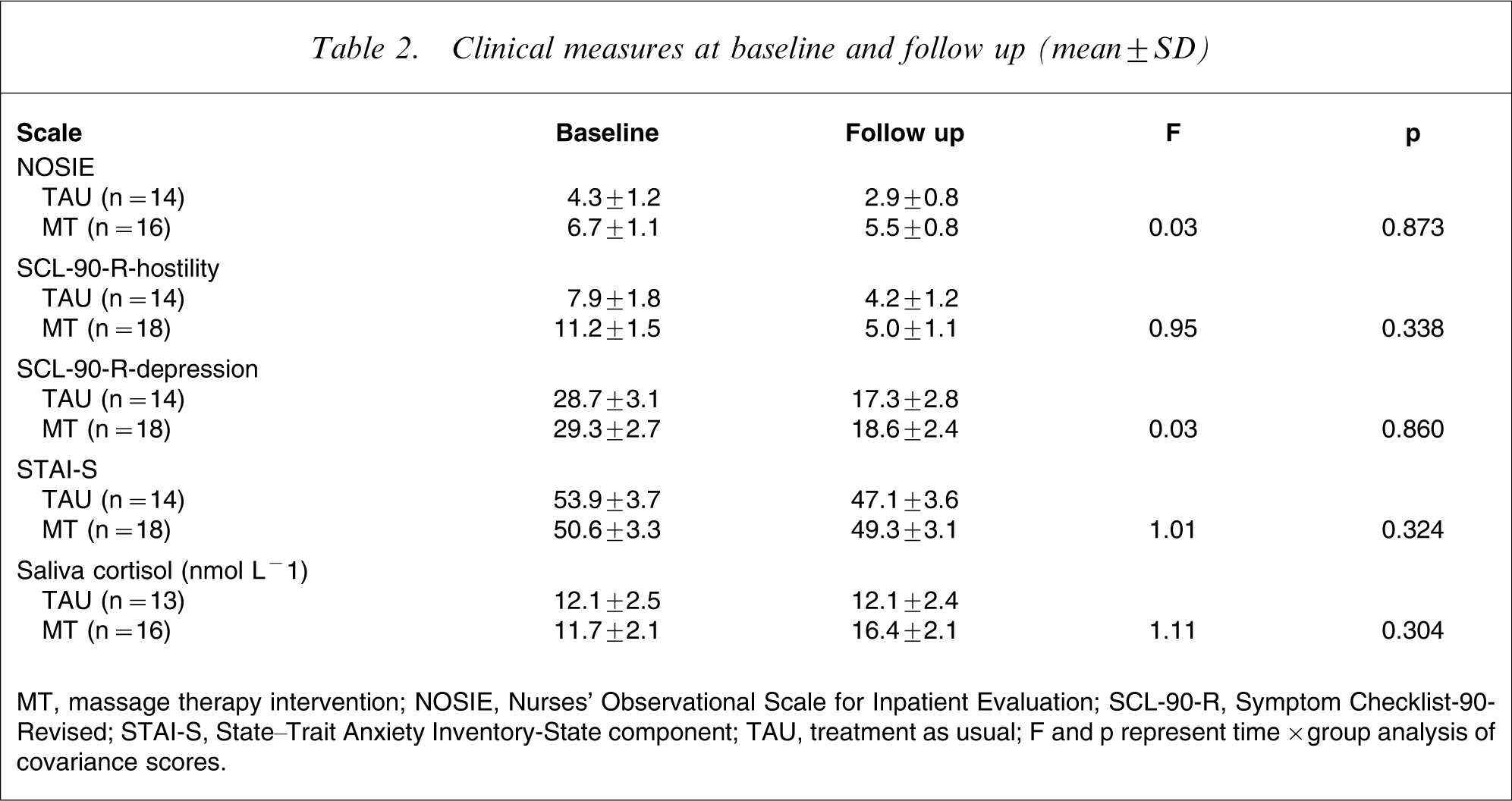
MT, massage therapy intervention; NOSIE, Nurses’ Observational Scale for Inpatient Evaluation; SCL-90-R, Symptom Checklist-90-Revised; STAI-S, State–Trait Anxiety Inventory-State component; TAU, treatment as usual;. F and p represent time×group analysis of covariance scores.
As expected, the SCL-depression and STAI-S scores were positively correlated at baseline (r = 0.625; p < 0.001) and follow up (r = 0.773; p < 0.001) in the entire sample. Likewise, the SCL-depression and hostility scores were positively correlated at baseline (r = 0.439; p = 0.002) and follow up (r = 0.564; p = 0.001). The staff-rated NOSIE scores were positively correlated with the SCL-hostility scores at baseline (r = 0.423; p = 0.003) and follow up (r = 0.330; p = 0.075), although the latter failed to reach significance.
The immediate effects of massage therapy are shown in Table 3. Following the 20 min massage therapy session there was a significant reduction in STAI-S scores (p < 0.001), resting heart rate (p < 0.05) and saliva cortisol levels (p < 0.05) at both the initial and final massage therapy session.
Immediate effects of massage therapy (mean±SD)
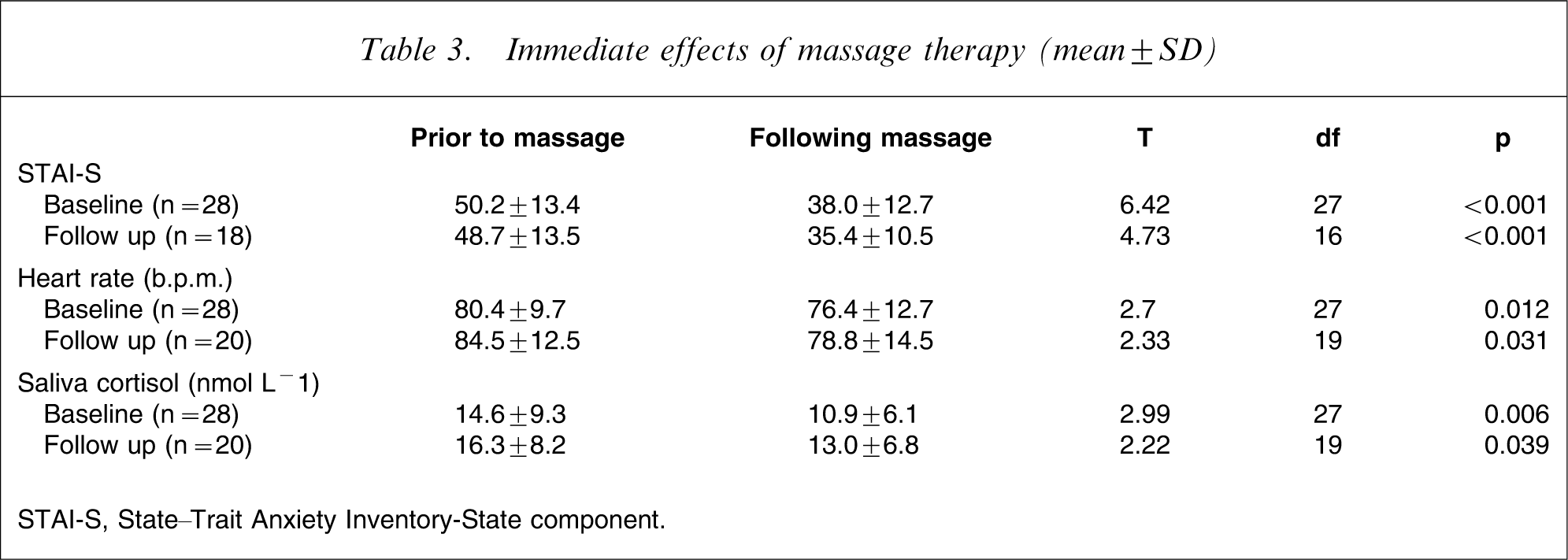
STAI-S, State–Trait Anxiety Inventory-State component.
Critical incident data
Unit characteristics during the TAU and MT phase are shown in Table 4. There were no differences in the proportion of male patients, involuntary admissions or main diagnostic categories during the two treatment phases. On average, 27% of patients on the unit received a massage therapy session each day during the MT phase.
Unit characteristics
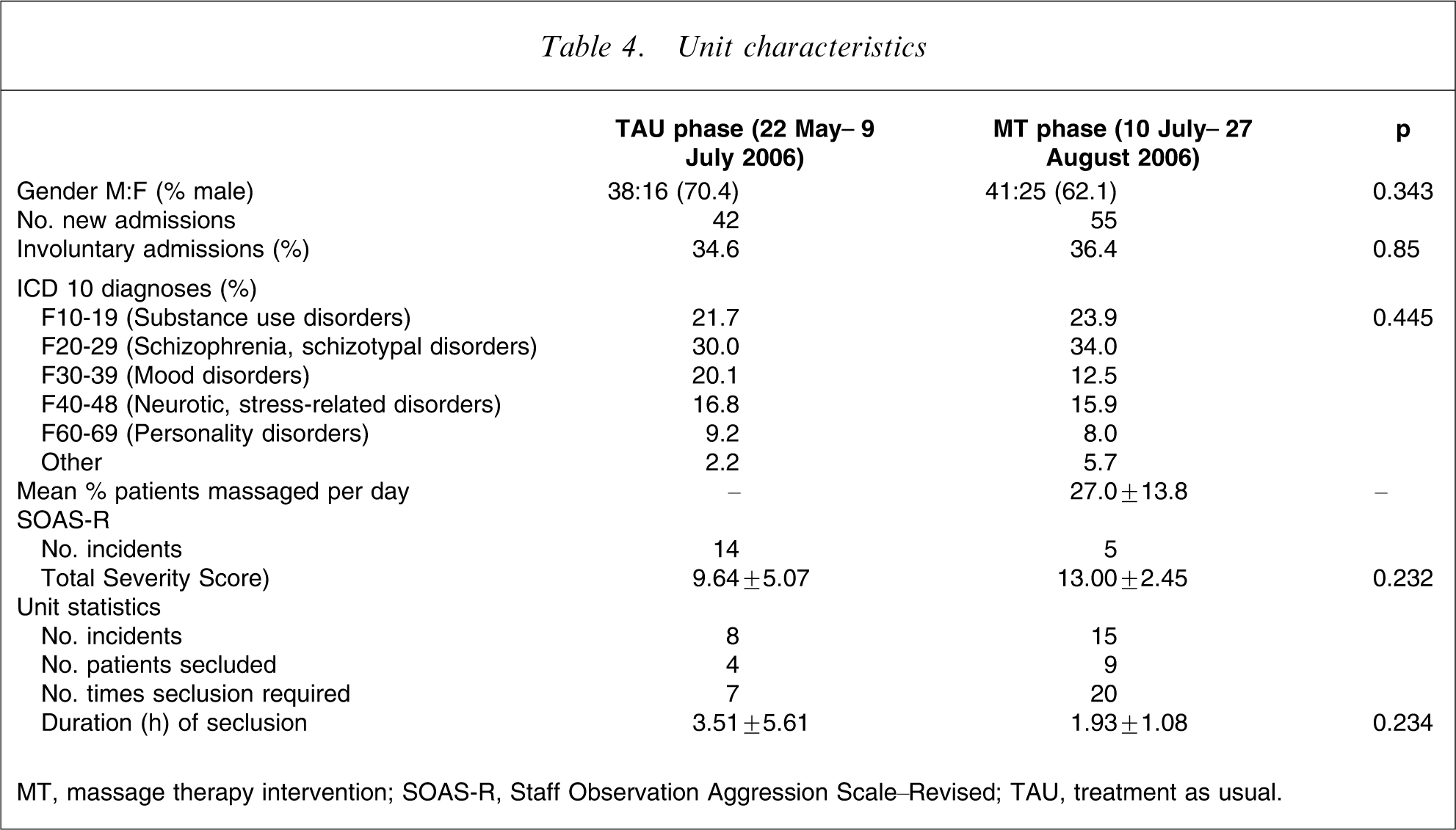
MT, massage therapy intervention; SOAS-R, Staff Observation Aggression Scale–Revised; TAU, treatment as usual.
Information relating to critical incidents on the unit over the course of the study was collected. Any incident that occurred on the unit over that time period was rated, irrespective of whether a study participant was involved or not. In total, 19 incidents were rated by staff on the SOAS-R during the course of the study: 14 during the TAU and five during the MT phase (Table 4). There was no difference in the total severity scores of the incidents (p = 0.23), but according to the statistics routinely collected on the Unit there were 23 critical incidents involving any patients on the unit over the course of the study: eight during the TAU and 15 during the MT phase. These incidents ranged from low risk (e.g. patient grabbed door from nurses’ hand and pushed him/her out of the way when attempting to abscond) to high risk (e.g. patient was physically threatening with toilet seat to nursing staff; stole staff keys and swipe-card and attempted to open exit doors unsuccessfully). During the TAU phase two low-risk, five medium-risk and one high-risk incident were recorded. During the MT phase two low-risk, 12 medium-risk and one high-risk incident were recorded. A total of seven patients contributed to the eight incidents during TAU and 15 patients contributed to the 15 incidents during the MT phase.
Discussion
The aim of the present pilot study was to determine whether the introduction of a relaxation massage therapy programme would lead to a reduction in anxiety, stress and aggression among inpatients on a young adult psychiatric unit. The present findings show that seated relaxation massage therapy was well received by a large proportion of patients. Approximately 60% (29/48) of patients who met the study inclusion criteria agreed to participate in the massage therapy arm of the study. A further five patients volunteered to receive the massage therapy but refused participation in the study measures. Main diagnoses of MT participants included non-affective psychosis, borderline personality disorder, mood disorder and bipolar disorder. To date, two previous studies have reported beneficial effects of massage therapy in adolescent female inpatients with bulimia [7] and hospitalized patients with depression [9], [17]. The current study shows for the first time that massage therapy is also readily accepted by a significant proportion of adolescent/young adult psychiatric inpatients with a range of disorders including psychotic disorders, personality disorders and affective disorders.
Effect of massage therapy on patient variables
The preliminary findings suggest that a single 20 min massage therapy session is effective in reducing transient anxiety and stress levels in psychiatric inpatients. Following the initial and final massage therapy session there was a significant reduction in self-reported anxiety, resting heart rate and cortisol levels. This is consistent with previous studies demonstrating a reduction in anxiety and cortisol levels following a short 20–30 min massage session [7], [8]. But due to the lack of a specific control therapy in the present study, such as one-on-one relaxation breathing techniques with a therapist, we cannot definitively conclude that these effects were due to the massage therapy itself.
All participants, regardless of treatment group, experienced a substantial decrease in symptoms of depression (approx. 38% mean decrease in SCL scores) and hostility (approx. 52% mean decrease in SCL scores) during admission on the unit. Contrary to expectation, however, massage therapy did not result in a significant further reduction of these symptoms in addition to the standard treatment. MT participants received on average 4.3 massage therapy sessions (range = 2–12, SD = 2.5) over an average of 4.6 days (range = 2–14, SD = 3.1). It is possible that longer term effects of massage therapy on symptoms of depression or hostility may only a greater number of massage therapy sessions administered over a longer time span. Indeed, previous studies that reported a reduction in hostility or depression over time with massage therapy administered a total of 10 massage therapy sessions (2×20 min massages per week over a period of 5 weeks) [7], [10]. Given the substantial decrease in hostility and depression symptoms observed with standard treatment in the present study, there may have also been a floor effect, minimizing the ability to detect an additional effect of the massage therapy.
Patient irritability (as rated by staff on the NOSIE) also tended to decrease during admission in both treatment groups, although this failed to reach significance (p = 0.22). Similarly, there was no significant change over time in transient anxiety levels (STAI-S) or cortisol levels of participants in either treatment group, suggesting neither standard treatment nor massage therapy intervention treatment was effective in reducing these factors. Alternatively, transient anxiety or cortisol levels may have temporarily increased at the follow-up assessment in anticipation of being discharged from the unit, therefore masking any reduction in these variables that may have occurred during the treatment period.
Use of PRN medication was similar between treatment groups, suggesting the massage therapy treatment did not reduce the need for PRN medication. But there were significant differences in the characteristics of the treatment groups at baseline that may have confounded these results. First, significantly more participants in the MT group were admitted to the unit involuntarily and tended to be rated by staff as more irritable compared to participants in the TAU group, indicating that the MT group may have been a more acutely unwell population. Second, MT participants had higher levels of non-prescription use of sedatives such as benzodiazepines in the month prior to admission and therefore may have been more likely to request PRN medication while on the unit. Third, there tended to be differences in the proportion of primary diagnoses of the two treatment groups. More MT participants had a diagnosis of bipolar disorder and borderline personality disorder. Some of the symptoms of mania include disruptiveness and disinhibition and these patients reportedly receive more PRN medication than psychiatric inpatients with other diagnoses [4].
The number of aggressive incidents and/or seclusion rates among participants was too low to meaningfully examine the effect of massage therapy on these variables (Table 1). In future, having a minimum cut-off criterion for moderate levels of aggression in the inclusion criteria would help to more accurately determine the effect of massage therapy on aggression in these patients. Because non-participant patients carried out the majority of aggressive incidents on the Unit during both treatment phases, this suggests that those patients more likely to be aggressive were also less likely to participate in research, potentially resulting in a biased sample. Cluster randomized trials may therefore be more useful, in which the intervention treatment is offered to all patients and non-participant based, naturalistic outcomes (such as unit statistics of PRN medication use or frequency of incidents) are assessed.
Effect of massage therapy intervention on the incidence of aggression on the Unit
On average 27% of patients per day received a massage therapy session during the MT phase. Fewer aggressive incidents were reported by staff on the SOAS-R during the MT phase (n = 5) compared to the TAU phase (n = 14), but upon analysis of statistics routinely collected on the Unit, more aggressive incidents occurred during the MT phase (n = 15) than the TAU phase (n = 8). Given the large discrepancy between these two methods of incident reporting, we unfortunately cannot reliably conclude on the effect of the massage therapy programme on overall levels of aggression on the unit.
Study limitations
There are several limitations of the present study. First, the TAU and MT phases were not randomized and occurred over a relatively short time period. Patient and unit characteristics can fluctuate from week to week and throughout the year and therefore the treatment may not have been assessed during an accurate representation of the unit. Although both treatments were primarily conducted during the winter months, the MT phase occurred very close to spring, during which previous studies have reported an increase in the presentation of bipolar disorder [18]. Aggressive behaviour in both men and women with bipolar disorder has also been shown to peak in the spring [18]. A second limitation of the present study was the lack of a specific control relaxation therapy to compare with relaxation massage therapy, making it difficult to accurately determine whether the effects of massage were due to therapeutic touch or other associated factors such as one-on-one time with a therapist. Finally, due to the lack of reliability of aggressive incidents reported by staff during the study we were unable to adequately assess the effect of massage therapy on levels of aggression.
Implications and future directions
These preliminary findings suggest that a short 20 min massage therapy session has immediate beneficial effects on anxiety and stress-related measures in acute psychiatric inpatients. PRN medications are frequently used for patients in mental health settings in order to calm patients and manage agitation, distress or difficult behaviour. As previously discussed, these medications are widely prescribed and administered but are often associated with adverse side-effects. We propose that relaxation massage therapy may be a useful treatment when used on an as-needed basis to calm patients and reduce levels of stress, anxiety and agitation, which could potentially reduce and in some cases eliminate the need for PRN medication in certain patients. Massage therapy is a safe and benign treatment, offering significant advantages over other methods such as medication to reduce stress or agitation. Furthermore, this type of basic relaxation massage does not require intensive therapeutic training and could be administered by nurses on the unit. Massage therapy as an additional tool for behavioural management in psychiatric inpatient units would also likely result in greater patient satisfaction, improvement of the staff–patient relationship and the therapeutic milieu of the unit. Controlled, randomized studies examining the effect of massage therapy on patient agitation, anxiety and PRN medication use are warranted.
Footnotes
Acknowledgements
This work was supported by National Health and Medical Research Council (NHMRC) Programme Grant 350241. Dr Belinda Garner is supported by an NARSAD Young Investigator Award. The massage chair was donated by Melbourne Health. The authors would like to thank the patients and staff of the ORYGEN Inpatient Unit at ORYGEN Youth Health and Ms Annemaree Gibson for her assistance in administering the massage therapy sessions.