
Abstract
Numerous studies have shown that patterns of alcohol use and misuse in adolescence and adulthood are associated with age of initiation to alcohol use. Longitudinal data from the Christchurch Health and Development Study suggest that commencement of alcohol use in childhood and early adolescence increases the likelihood of regular and high-risk alcohol use in adolescence, independent of other influences [1], [2]. There is also evidence that early initiation to drinking increases the risk for more severe alcohol problems. For example, data from the National Longitudinal Epidemiologic Survey of 27 616 young people in the USA indicate that the lifetime alcohol dependence rates of people who initiate alcohol use by age 14 are fourfold higher than those who start at age 20 years or older [3]. Collectively, these studies suggest that early initiation to drinking increases the risk for problematic patterns of alcohol use in later life.
Knowledge of risk factors for early initiation to alcohol use is important for the development of effective education and preventative interventions to reduce problematic drinking and its related harms. One factor that has been implicated in the development of adolescent alcohol use and misuse is the quality of the parent–adolescent relationship. Researchers have suggested that a healthy parent–adolescent relationship fosters open communication between parents and adolescents, providing a foundation for better parental monitoring and the setting of appropriate boundaries relating to alcohol use [4], [5]. Consistent with this notion, a study of 493 secondary students, with an average age of 16.2 years, found that adolescents who misused alcohol were significantly more likely to report lower levels of parental care [6]. Similarly, a 3 year longitudinal study of 7540 adolescents in the USA found that good-quality parent–adolescent relationships were associated with lower drinking [7]. Conversely, adolescents who reported increasing across-time levels of alcohol use more frequently experienced parent–adolescent relationship difficulties, including emotional difficulties, separation and detachment, and greater family stress and conflict.
Child development theorists suggest that the foundation for the establishment of a good-quality relationship between parent and adolescent is laid early in life. According to the Bowlby attachment theory the quality of the relationship between parent or primary caregiver and child is typically established between birth and 12 months of age [8]. The notion of antenatal attachment has also received increasing attention, with theorists postulating that the mother bonds to her unborn baby in a way analogous to the formation of the mother–infant attachment after birth [9]. It has been argued that the nature of the relationship that an expectant mother develops during pregnancy with her unborn baby may be predictive of future maternal–infant attachment [10]. While there is debate about the capacity for such early experiences to shape later child and adolescent development [11], longitudinal studies of mother–infant attachment show that early patterns of relating in infancy tend to remain moderately stable during the preschool and elementary school years, through to late adolescence [12]. Moreover, numerous studies in the field of infant psychology have established that early attachment patterns predict later psychological and behavioural outcomes in adolescence [13–16].
Studies of maternal psychological states during pregnancy and the postnatal period have also identified long-term effects on child cognition and behaviour. Most notably, researchers have focused on the effects of maternal depression and anxiety during pregnancy and the postnatal period [17–21]. For example, O'Conner et al. prospectively examined the effects of antenatal stress and anxiety in 7448 mothers on child behavioural and emotional outcomes [20]. Mothers who scored in the top 15% of the sample on anxiety symptoms at 18 and 32 weeks gestation were 2–3-fold more likely to have a child with behavioural and emotional problems at age 4 years.
Within the context of the mother–child relationship, a number of authors have emphasized the significance of maternal attitudes during both pregnancy and early infancy [22]. Broadly defined, an attitude refers to ‘a psychological tendency that is expressed by evaluating a particular entity with some degree of favour or disfavour’ [23]. There is a small body of research that suggests that negative maternal attitudes to pregnancy and infant caregiving are associated with problems in child health and development [24–26]. For example, Bor et al. prospectively examined a community sample of women and children from 6 months post-partum to child age 5 years [24]. After controlling for a range of confounding variables, the study found that negative maternal attitudes towards caregiving at 6 months predicted internalizing behaviours in girls and externalizing behaviours in boys at 5 years. In another prospective study, Wilkins et al. assessed whether maternal attitudes to both pregnancy and infant caregiving were associated with children's health-related quality of life in adolescence [26]. The study found that mothers’ negative attitudes toward the pregnancy and infant caregiving independently predicted poorer psychosocial health-related quality of life in adolescents at 13 years, after controlling for a number of important confounding variables.
Taken together, a growing body of research suggests that maternal mental health status during the perinatal period can influence a range of cognitive, behavioural and health-related outcomes in offspring during childhood and early adolescence. To date, however, no studies of which we are aware have examined whether maternal attitudes during this period contribute to the prediction of adolescent drinking initiation. The aim of the present study was therefore to draw together research on adolescent alcohol use and early child development, in order to examine whether maternal attitudes to (i) pregnancy, and (ii) infant caregiving at birth and 6 months, predict early drinking initiation at age 14. Specifically, it is hypothesized that negative maternal attitudes toward pregnancy and infant caregiving would independently predict drinking initiation at age 14, after controlling for a range of potential confounding sociodemographic, maternal, obstetric and infant risk factors.
Methods
Design
This study used data from the Mater University study of pregnancy (MUSP), a birth cohort study of women and their babies conducted in Brisbane, Australia. Baseline data were collected on 7223 consecutive public patients presenting for the first antenatal visit between 1981 and 1984 at the Mater Misericordiae Hospital. The Mater Misericordiae Hospital is based in the southside urban area of Brisbane and services both private and public patients. As reported in an early paper describing the cohort demographics, the sample overrepresented women from lower socioeconomic background [27]. Mothers were first interviewed in hospital at their first antenatal visit (approximately 16 weeks into gestation). They were re-interviewed in hospital 3–5 days after the birth and contacted face to face or via telephone interviews at the 6 month follow up. Mothers and children were followed up again when the children were 5 and 14 years old. At 14 years both mothers and children filled in individual questionnaires at home or in hospital. The sample for this study consists of a cohort of 4258 mothers and children for whom complete data were available at baseline, birth, 6 months and at 14 year follow up. Written informed consent from the mother was obtained at each data collection phase. Each phase of the study received full ethical clearance from the Mater Misericordiae Hospital and the institutional University of Queensland Ethics Committee. All predictor and outcome variables were selected a priori.
Outcome measure
At the 14 year phase children were asked ‘how often do you drink alcohol’ (daily, a few times a week, a few times a month, a few times a year, rarely, never) and ‘how much do you drink on those occasions’ (seven or more glasses, five or six glasses, three or four glasses, one or two glasses, less than one glass, never drink). The two variables were used to obtain a dichotomous variable indicating those who had never consumed alcohol by age 14 and those who had. There were 65.2% of adolescents (n = 3358) who reported never consuming alcohol and 34.9% (n = 1796) who reported having consumed alcohol by age 14. In sensitivity analyses, we varied the cut-offs of this variable to determine whether a looser definition of initiation would substantively vary our findings. In one analysis we excluded 947 adolescents who had reported consuming ‘less than one glass’. In another analysis, we excluded those who reported drinking ‘rarely’ (n = 1130).
Predictors at the antenatal visit
Attitudes towards pregnancy were assessed at the first antenatal visit. Women were asked to recall retrospectively their initial reactions to becoming pregnant and whether they had planned or wanted their pregnancy.
Feelings on becoming pregnant
At the first antenatal visit, mothers reported their feelings about becoming pregnant by rating the following four items: (1) ‘I felt overjoyed’; (2) ‘I would have preferred not to become pregnant’; (3) ‘I felt unhappy’; and (4) ‘I felt it was the worst thing that could have happened to me’ (prompts: strongly agree, agree, unsure–mixed feelings, disagree, and strongly disagree). After Item 1 was reversed, we constructed the scale from the four items, responses were averaged and multiplied by 10, with higher scores representing positive feelings towards becoming pregnant. The scale Feelings on becoming pregnant had an optimum reliability coefficient (Cronbach α) of 0.85. The scores were recoded into a dichotomous variable (‘positive’, ‘negative’).
Pregnancy planned/wanted
The following items enquired into the degree to which pregnancy was planned (1, ‘I planned to get pregnant at this time’), unplanned (2, ‘It just happened’; 3, ‘I meant to avoid pregnancy at this time’), wanted (4, ‘I wanted to get pregnant at this time’) or the result of failed family planning (5, ‘My method of family planning failed’). Women could choose between the following prompts: no, unsure, yes. Items 3 and 5 were reversed so that high scores reflected a planned/wanted pregnancy. The scores were recoded into a three-value variable (‘planned/wanted’, ‘unsure’ and ‘not planned/wanted’). The scale achieved optimal reliability (Cronbach α = 0.89).
Predictors at birth
Maternal attitudes to physical contact with the baby
At 3–5 days after the birth, mothers indicated how they felt about physical contact using the following five statements: (1) ‘Relieved when the baby is taken to the nursery’; (2) ‘Prefer not to have the baby at night’; (3) ‘Can't resist nursing the baby’; (4) ‘Love to play with the baby’; and (5) ‘Wish I could have the baby all the time’ (prompts: strongly agree, agree, neutral, disagree, strongly disagree). After items 3, 4 and 5 were reversed so that high scores represented positive attitudes toward physical contact with the baby, all items were combined and the scale produced a good reliability coefficient (Cronbach α = 0.74).
Predictors at 6 months follow up
Maternal attitudes to caring for the baby
The following statements described how mothers felt about their babies at the 6 month follow up: (1) ‘Caring for my baby is very satisfying’; (2) ‘Feel so angry that sometimes I could smack my baby’; (3) ‘My baby makes me too tired’; (4) ‘My baby is so good I hardly know he/she is there’; (5) ‘Sometimes I feel like hitting my baby’; and (6) ‘I feel fed up looking after my baby all day’ (prompts: strongly agree, agree, neutral, disagree, strongly disagree). Items 1 and 4 were reversed and the scores for all items summed. Higher scores represented a more positive attitude (range 10–50). The scale was recoded into three categories (10–29.9 = 1, ‘always ready to care for the baby’; 30–42 = 2, ‘most times’; 42.1–50 = 3, ‘not always’) and produced a good reliability coefficient (Cronbach α = 0.75).
Maternal attitudes to teaching the baby
Women reported how well the following statements described how they felt about coaching their 6-month-old infant: (1) ‘Try to encourage baby to be interested in what's going on’; (2) ‘My baby likes me talking to him/her’; (3) ‘I spend a lot of time teaching my baby to recognize things’; and (4) ‘Love to play with my baby’ (prompts: strongly agree, agree, neutral, disagree, strongly disagree). All items were reversed, so that high scores represented greater commitment to teaching the baby. The scale showed acceptable reliability (Cronbach α = 0.65).
Potential confounders
Demographics
The following characteristics were also included from the first antenatal visit: maternal sociodemographic position, including maternal age (13–19 years; 20–34 years; ≥35 years), mothers’ education (did not complete secondary school, completed secondary school, completed further/higher education) and marital status (married, cohabiting, single).
Maternal alcohol and tobacco use
Maternal alcohol consumption was measured at the antenatal visit with two items assessing frequency (from never to daily) and quantity (from 0 to 7+ standard drinks) of alcohol consumption. These data were used to categorize women into three categories (0 = abstainers, 1 = at least one drink per week, 3 = 1+ drinks per day). Women reported whether they smoked and, if so, how many cigarettes they smoked over a 7 day period. Smoking status was categorized into non-smoker, 1–19 cigarettes per day and ≥20 cigarettes per day.
Maternal mental health
Maternal depression and anxiety were assessed at the first antenatal visit using the Delusions–Symptoms–States Inventory (DSSI) [28]. The DSSI contains two seven-item subscales measuring depression and anxiety, which have been found to correlate strongly with other scales of depression, including the Beck Depression Inventory [29]. In the present study maternal symptoms of depression and anxiety were defined as reporting four or more of the seven symptoms in the DSSI depression and anxiety subscales.
Obstetric factors and early temperament
Biological predictors were taken from obstetric records at birth and included gestational age, child gender and birthweight. At 6 months the child's temperament was assessed through a seven-item index developed for this study. Women reported how often their baby had the following problems: colic, sleeplessness, vomiting, diarrhoea or constipation, feeding problems, skin problems and overactivity. Each item was scored on a 5-point scale (0–3 symptoms = ‘easy behaviour’; ≥4 symptoms = difficult behaviour’). The internal consistency of the scale was acceptable (Cronbach's alpha = 0.65).
Data analysis
χ2 tests were used to examine univariate associations between alcohol initiation, the main predictors (maternal attitude towards pregnancy at baseline and towards the baby at the 6 months follow up) and potential confounders. χ2 tests were also used to examine univariate associations between maternal attitudes in pregnancy, at birth, and at the 6 month follow up. Next, multivariate associations were assessed using progressive logistic regression models. Model 1 was adjusted by child age; model 2 was adjusted by child gender, birthweight, gestational age and temperament at 6 months, and maternal education, age, marital status, alcohol use, tobacco use, and anxiety and depression in pregnancy. Model 3 included all previous adjustments and all predictors of maternal attitudes described in the measures section. Data analyses were conducted on a selected sample of 4258 for whom complete data on all the aforementioned measures were available. χ2 tests of association between the main predictors were conducted on a larger sample (n = 6576), due to fewer missing data. A confirmatory data check in the smaller sample found that the overall patterns of results did not vary from the pattern identified in the larger sample.
We conducted a range of sensitivity analyses. We repeated the aforedescribed analysis changing the cut-off of the two scales that yielded a significant relationship with drinking initiation in adolescence. For the Feeling on becoming pregnant scale, we repeated the analysis using 5% and 11% cut-offs to define the ‘positive’ group. For the Family planning/child wanted scale we repeated the analysis changing the definition of the ‘not planned/wanted’ group to 14% participants with the lowest scores. We also repeated all analyses on each of the items of the scales predicting initiation at child age 14, to better understand whether specific items included in the scale had a stronger effect. Finally, in order to ensure that the results were not driven by the choice of cut-off for defining alcohol initiation, we repeated all analyses using different definitions of alcohol initiation. First we excluded those who had reported drinking ‘rarely’, then those who reported consuming ‘half a glass’ of alcohol. Finally, we repeated the multivariate analyses using measures of maternal mental health and tobacco and alcohol use administered at other time periods (14 year follow up for tobacco and alcohol and 6 month follow up for the mental health assessment), to explore whether exposure to maternal postnatal depression and concurrent exposure to maternal substance use in adolescence modified the results presented here. All analyses yielded the same results as those reported in this paper.
Attrition
In the fully adjusted model complete data were available for approximately 61% of children. Inverse probability weighting was used (with bootstrapping robust methods to correct for standard errors estimates) to account for attrition. We first used an exploratory logistic regression model to identify predictors of attrition. There were no significant differences between those lost to follow up and those still in the study on the main predictors of interest. But those lost to follow up were significantly more likely to be born to mothers who drank regularly (p = 0.001) and smoked during pregnancy (p = 0.002). The mothers of those lost to follow up were also more likely to report symptoms of depression (p = 0.008) and anxiety (p = 0.03) and to be cohabiting with their partners (p = 0.001) or single (p = 0.001) at baseline. These measures were fitted in a logistic regression model (response vs non-response as outcome) to determine weights for each individual using the inverse probability of response [30]. We then repeated all multivariate analyses including the weighting adjustments. The results did not differ substantively from those presented in this paper.
Results
Table 1 shows the frequency responses for the main maternal variables. The group reporting negative feeling towards pregnancy accounted for approximately 7% of respondents, whereas almost 20% of mothers reported an unplanned or unwanted pregnancy. Six months after the birth, some mothers reported not wanting contact with their baby (7.9%) or not always feeling ready to care for their baby (6%). Approximately 15% of mothers did not always want to teach their baby.
Maternal predictors of alcohol initiation
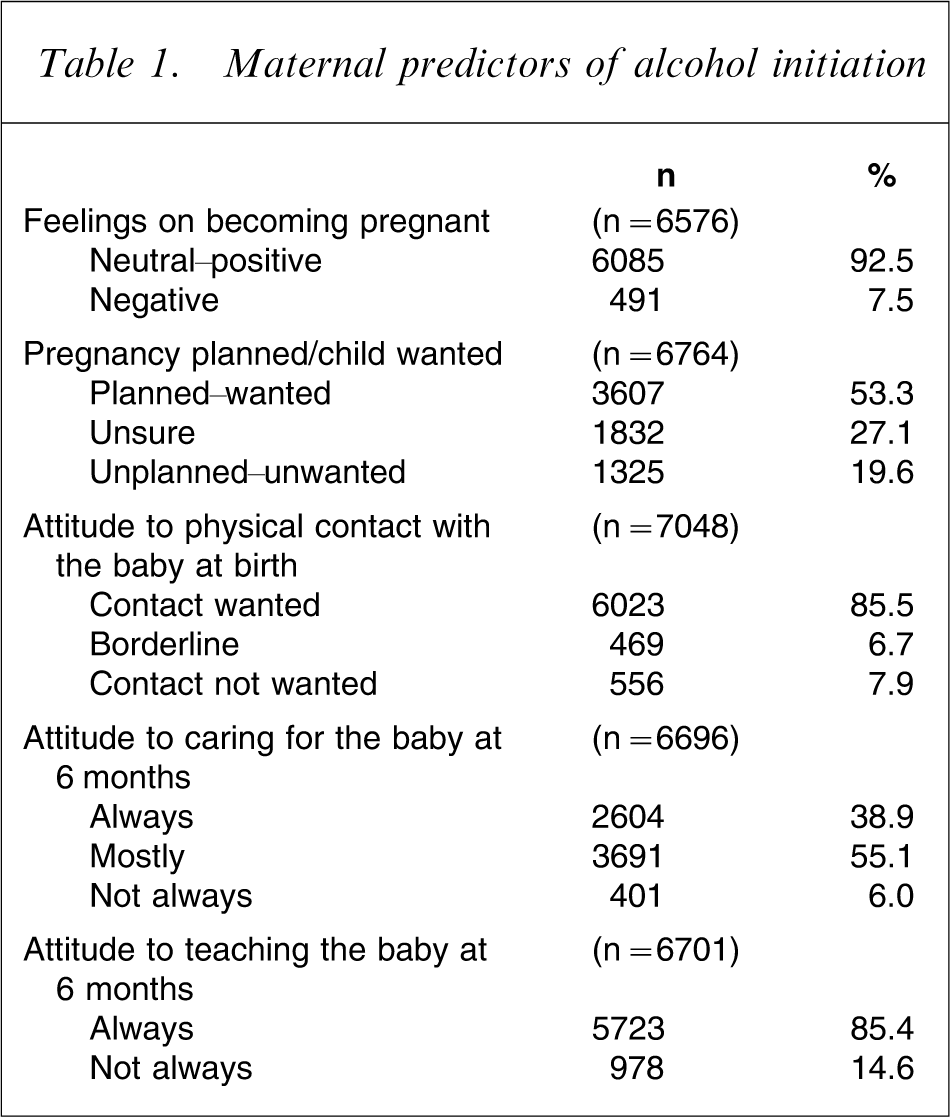
Table 2 shows univariate associations between maternal attitudes towards pregnancy at the first antenatal visit, towards the baby at birth and the 6 month follow up, and drinking initiation at child age 14. Those born to mothers who reported negative feelings about being pregnant at the first antenatal visit, were more likely to have consumed alcohol at the 14 year follow up, as were children of mothers who reported not having planned/wanted the pregnancy. Maternal attitudes to physical contact with and caring for the baby at birth and 6 months were not significantly associated with alcohol initiation, whereas there was a weak but significant association between not wanting to teach the baby and having consumed alcohol at age 14.
Univariate associations between maternal attitudes and drinking initiation (total n = 4258)
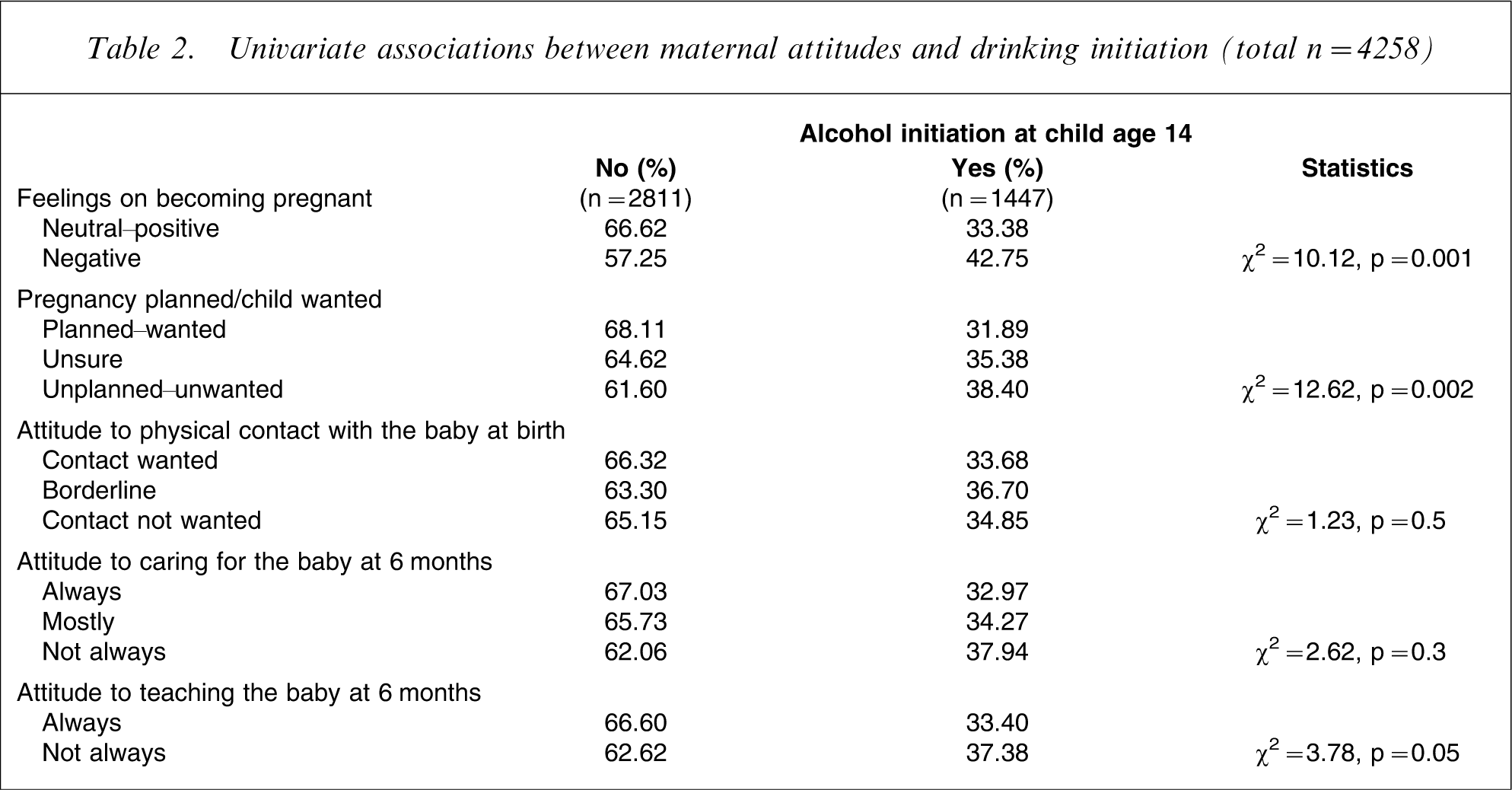
Table 3 presents univariate associations between maternal attitudes to pregnancy at the first antenatal visit and attitudes to the baby at birth and 6 months. Results indicated that in general, mothers who reported negative feelings and attitudes to pregnancy also reported negative attitudes toward infant caregiving in the postnatal period. Specifically, strong positive associations were identified between negative maternal feelings about being pregnant and negative attitudes to physical contact, caring for and teaching the baby. Significant associations were also identified between not planning/wanting the baby and mother's negative attitudes to caring for and teaching the baby at 6 months. There was one exception to this trend: pregnancy planned/child wanted was not significantly associated with maternal attitudes to teaching the infant at 6 months.
Univariate associations between maternal attitudes in pregnancy, at birth and at 6 months (total n = 6576)
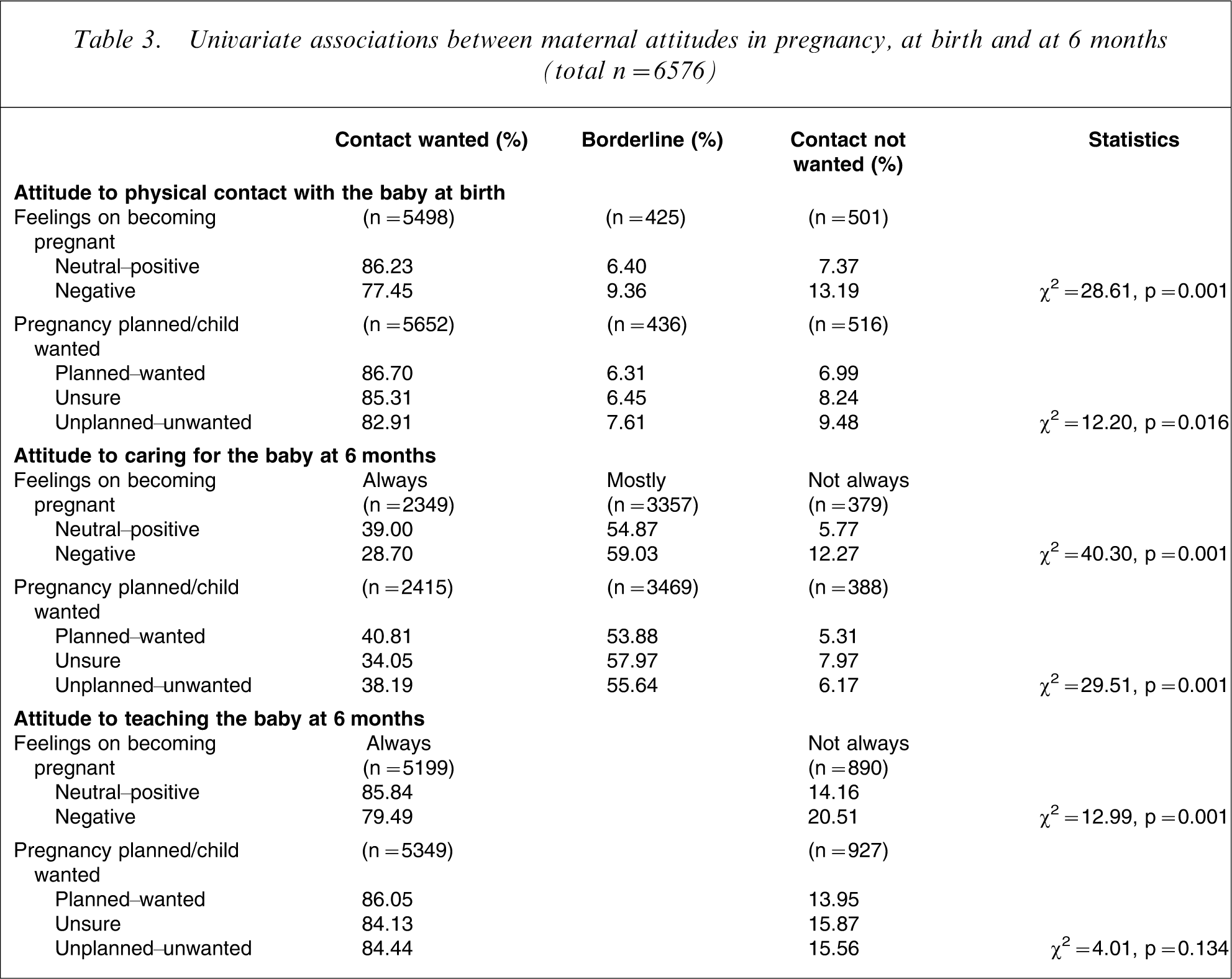
Table 4 presents associations between drinking initiation in early adolescence and potential confounding factors in pregnancy and at 6 months, including child characteristics and maternal demographics, mental health and substance use. Children of mothers who were cohabiting or single at the first antenatal visit were more likely to have started drinking at age 14, as were children whose mothers consumed alcohol and smoked cigarettes during pregnancy. There were no significant differences in early adolescent drinking initiation on any of the other potential confounding factors.
Univariate associations between potential confounders and drinking initiation (total n = 4258)
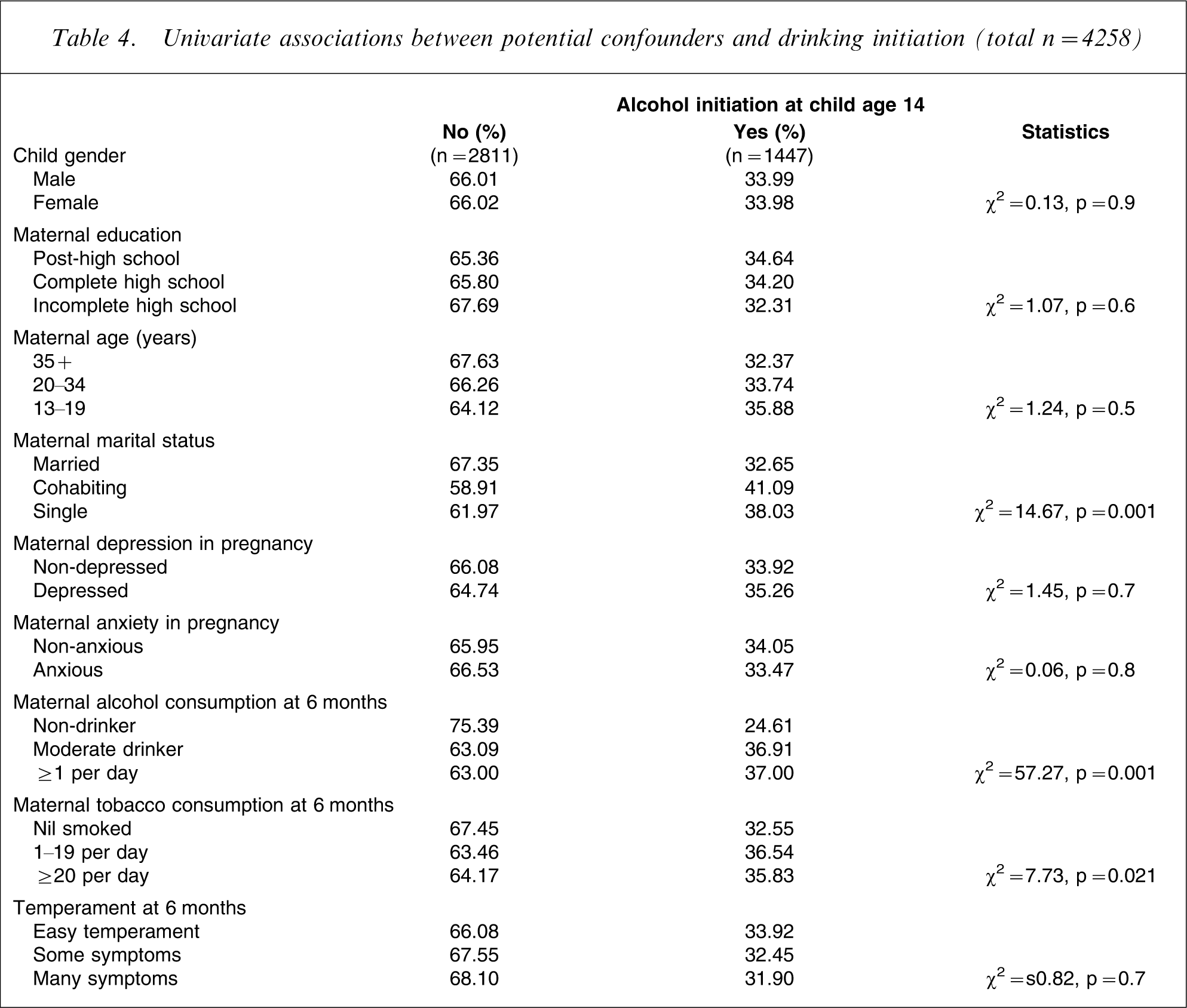
Table 5 shows multivariate associations between maternal perception of pregnancy and attitude towards the infant at birth and 6 months and initiation of alcohol use at age 14. Adolescents born to mothers who reported negative perceptions about their pregnancy were more likely to have consumed alcohol at the 14 year follow up, compared with those who reported positive perceptions. This was also true for those whose mothers reported not having planned or wanted the pregnancy. There were no significant relationships between attitudes to physical contact, caring for and teaching the baby and drinking initiation at age 14.
Multivariate associations between maternal attitude and initiation of alcohol use at age 14 (total n = 4258)
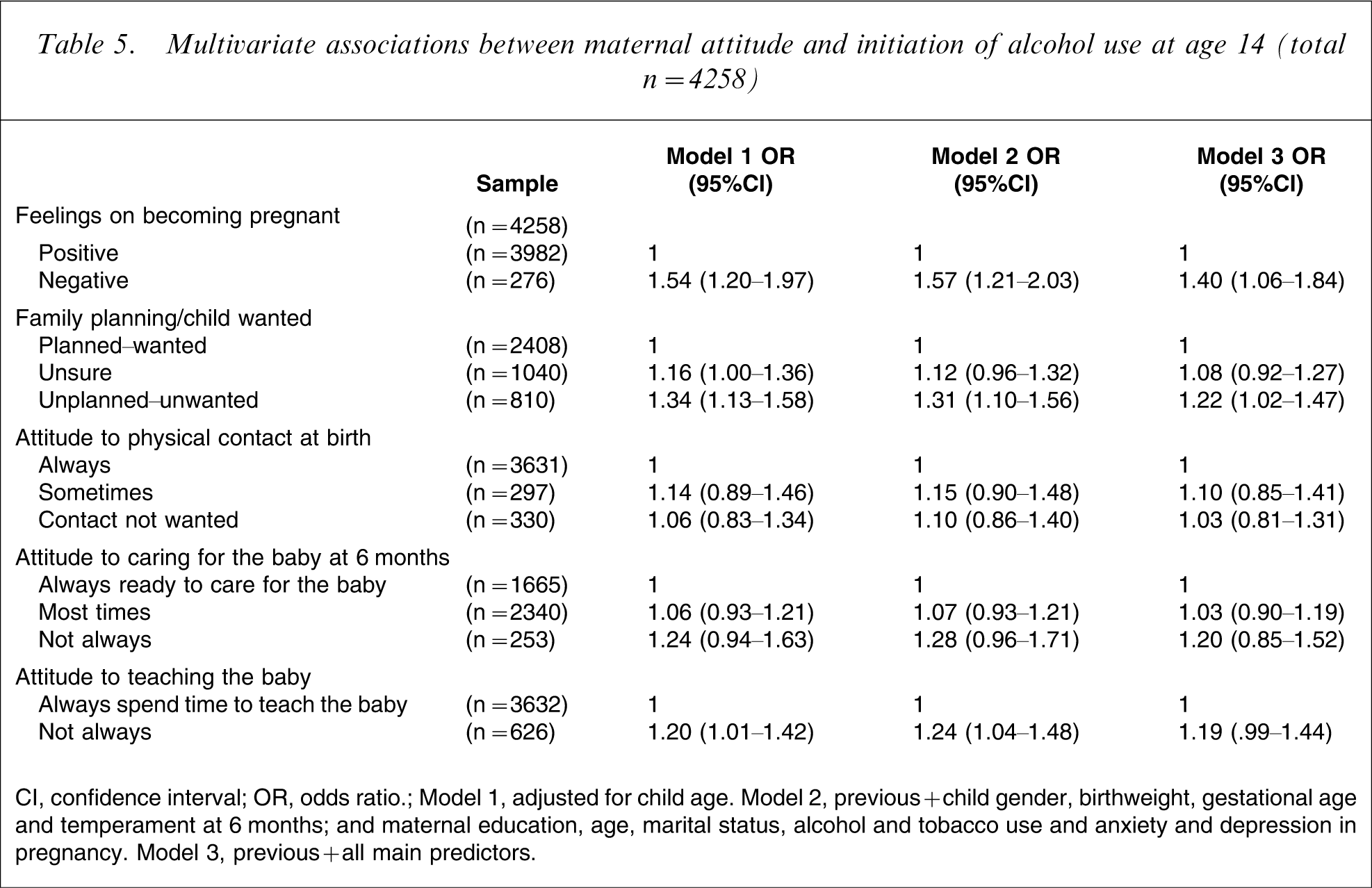
CI, confidence interval; OR, odds ratio.
Model 1, adjusted for child age. Model 2, previous + child gender, birthweight, gestational age and temperament at 6 months; and maternal education, age, marital status, alcohol and tobacco use and anxiety and depression in pregnancy. Model 3, previous + all main predictors.
In sensitivity analyses in which we used a less conservative definition of drinking initiation (by excluding those who reported drinking ‘rarely’ and ‘less than one full glass’), the results were virtually the same as those presented in Table 4. Similar results were also obtained when we reduced the percentage of the ‘negative’ group to 5% (odds ratio (OR) = 1.40, 95% confidence interval (CI) = 1.01–1.92) and when we increased it to 12% (OR = 1.35, 95%CI = 1.09–1.67). For the Family planning/child wanted scale, repeating the analysis using a more stringent 14% cut-off for the ‘not planned/wanted’ group produced similar results to those presented in Table 4 (OR = 1.26, 95%CI = 1.05–1.51).
When analyses were repeated for each of the items forming the Family planning/child wanted scale, we found that most of the effect was accounted for by mothers not wanting to be pregnant and/or having failed a family planning method (data not presented). For those whose mothers admitted not wanting to be pregnant at the baseline interview the OR for drinking initiation in offspring was 1.22 (95%CI = 1.00–1.49) whereas failure in family planning methods accounted for a 30% increased risk (OR = 1.29, 95%CI = 1.04–1.59) of drinking initiation at child age 14.
Finally, we repeated all multivariate analyses using the inverse probability weighting procedure to examine the possible impact of loss to follow up on the results. When we included the weighting adjustments in the final model, results remained virtually the same as those presented in this paper.
Discussion
This study has identified a number of early predictors of alcohol initiation in adolescence. Specifically, mother's negative feelings about being pregnant and not planning/wanting the pregnancy predicted alcohol initiation in offspring at the 14 year follow up. Maternal socioeconomic indicators such as marital status and lifestyle characteristics such as alcohol and tobacco use were also significantly associated with drinking initiation. But maternal attitudes to infant caregiving at birth and at 6 months were not significantly associated with adolescent alcohol initiation in multivariate analysis. Several important issues arise from these findings. First, the results suggest a need for greater awareness of the importance of maternal attitudes in pregnancy. Second, there needs to be consideration of how maternal attitudes to pregnancy can have an effect on offspring alcohol use 14 years later. We also need to account for the differential outcomes associated with mothers’ attitudes in pregnancy and early infancy. Finally, the implications of these findings need to be considered in terms of public health and preventative interventions.
While numerous studies have focused on aspects of the mother–infant relationship in the context of child development [13], [16], this is the first prospective study that we are aware of to have examined the role of maternal attitudes during pregnancy and early infancy in predicting drinking initiation in adolescence. Consistent with our hypotheses, children born to mothers who reported negative feelings about being pregnant or not having planned or wanted their pregnancy at their first antenatal visit were more likely to have consumed alcohol at the 14 year follow up. Our findings are consistent with limited existing evidence that has identified associations between maternal mental health status in pregnancy and outcomes in children's health and development [20], [26]. The present study adds to the existing evidence by suggesting that maternal negative attitudes towards pregnancy are associated with early use of alcohol more than 14 years later and supports the view that a mother's relationship with her child commences prior to birth [22]. The present results are also consistent with the theoretical notion that positive maternal attitudes to pregnancy and the developing fetus are related to the establishment of a healthy mother–infant relationship in the postnatal period [9], [10]. Similar evidence has been gathered on research looking at behavioural and emotional domains of child development, but this is the first study that has replicated these findings in relation to substance use, specifically alcohol initiation. Taken together with past studies, it appears that these positive attitudes may promote healthy child and adolescent development in a range of domains, including the use of alcohol.
Contrary to our hypotheses, mother's negative attitudes to physical contact, caring for and teaching the baby at birth and 6 months were not significantly associated with an increased risk for early initiation to alcohol at age 14. There are several possible explanations for the lack of consistency in these results. The relationship we found between antenatal attitudes and alcohol initiation may be a chance finding, and the present results may be due to measurement errors. This is possible, although point estimates remained mostly unchanged after multiple adjustments. There may have been errors in the measurements administered at birth and 6 months. It is notable, for instance, that the antenatal measures had higher reliability than those used at follow up. It may therefore be the case that poorer reliability in the follow up measures obscured an effect that was present yet small. Alternatively, mothers may not easily admit to having no desire to care for, or be close to their own baby, whereas they may be more prone to admitting negative attitudes towards pregnancy status. But the finding that maternal attitudes (i.e. positive, mixed or negative) remained fairly consistent from pregnancy through to follow up suggests that this is unlikely to have been the case for the majority of participants.
Literature in the field of developmental psychology has established that early attachment patterns predict later psychological and behavioural outcomes in adolescence [13–16]. The present findings partly concur with the view that maternal attitudes, a central aspect of the mother–child relationship [22], are also important in the prediction of later outcomes. The present results indicate that maternal attitudes formed in pregnancy tend to remain relatively consistent during the perinatal period. With respect to determining early onset drinking, however, it would appear that negative maternal attitudes and feelings toward pregnancy in the antenatal period are most important in the prediction of early drinking behaviour. Significant negativity toward pregnancy may serve as an indicator of maternal behavioural or physiological pathways that exert an influence on the developing fetus in ways that are not yet fully understood. Although further research is needed to identify these pathways of influence, the present findings draw attention to the antenatal period as a significant opportunity for early intervention with pregnant women.
Finally, it is notable that the association identified between maternal attitudes to pregnancy and drinking initiation in adolescence was partly confounded by socioeconomic position, expressed by maternal marital status, and by maternal alcohol and tobacco use in pregnancy. This suggests that the relationship between negative maternal attitudes in pregnancy and future drinking in adolescence may be mediated by parental modelling of drinking and smoking behaviour, familial factors (i.e. conflict and stress associated with parental drinking) and/or physiological influences (i.e. increased sensitivity to alcohol due to in utero exposure of the fetus), in addition to family circumstances (single parent status and cohabitation). While some of these factors are likely to exert their influence through biological or environmental modelling mechanisms [5], it seems plausible to suggest that such factors would also place additional strain on the mother–infant relationship, increasing the likelihood of negative outcomes in adolescence such as early onset drinking behaviour [6], [7].
Limitations
The present results should be interpreted within the context of some limitations. First, the sample was drawn from a low socioeconomic region of Brisbane, as a result middle- and high-income groups were underrepresented. Attrition was differential, with most of the loss occurring in the young, low-income, poorly educated mothers who were also more likely to smoke, drink and report more symptoms of anxiety and depression. But because many of the risk factors relevant to the present study often occur in mothers with the aforementioned characteristics, the findings are likely to be a conservative estimate of the relationship between maternal attitudes and later adolescent drinking initiation. When we explored further whether the findings were affected by attrition by attaching inverse probability weighting to subjects included in the analyses, we found no differences between the weighted and non-weighted results. This further suggests that attrition is unlikely to have biased the results.
Despite the fact that the study included a range of demographic and psychosocial measures prospectively assessed from early life through to age 14, we were unable to consider a number of other potentially important factors. These include genetic heritability, adverse childhood experiences, and other environmental influences such as paternal substance use, mental health and involvement in infant care. Because data were collected via self-reports, the present results are largely dependent on the subjective reports of mothers and their adolescent children. Future research would benefit from the inclusion of more objective assessments. In particular, observational measures of maternal caregiving behaviour, infant temperament and mother–child attachment style are recommended in future studies because maternal self-reported perceptions and attitudes may not necessarily reflect actual infant or maternal behaviour.
Implications
If replicated, the present results may have a number of implications for public health policy and clinical practice. Although concern for the effects of maternal postnatal psychological disturbances on children's health and development is warranted, the present results suggest that maternal mental states in the antenatal period may be important in determining childhood outcomes. But, because the effects found in the present study were small, these findings should be seen as preliminary evidence and will need replication using other longitudinal data with more robust assessments of both maternal attitudes and alcohol initiation. If these findings are replicated in other large prospective studies, greater attention should be devoted to the psychological and practical support needs of pregnant women early in the antenatal period.
Footnotes
Acknowledgements
The authors thank the MUSP Team, MUSP participants, the Mater Misericordiae Hospital and the Schools of Social Science, Population Health, and Medicine, (University of Queensland) for their support. The study has been primarily funded by the National Health and Medical Research Council (NHMRC) and Queensland Health. Rosa Alati is funded by NHMRC Public Health Fellowship grants (ID 301298).