
Abstract
It has been acknowledged that social relationships significantly influence perinatal mental health outcomes [1], [2]. Evidence supports the notion that, in the transition to parenthood, higher levels of social support are associated with better maternal mental heath status and lower levels of depressive symptoms [3], [4], resulting in improved infant cognitive and emotional development.
The significance of a deficiency in perinatal social support is evident in both the quantity and quality of personal relationships. Women who were depressed following childbirth rated the support of husbands as unsatisfactory and they perceived their spouses deficient in providing practical and emotional support [5]. A lack of marital closeness has been found to predict postnatal depressive symptoms [6]. Others have reported that couple mental health morbidity was greatest at 12 months after childbirth, and for mothers this was linked to partner relationship variables [7]. We have previously shown that depressed mothers have fewer social supports than non-depressed mothers and of the supports they did have, they generally viewed more negatively [Milgrom J, Ericksen J: personal communication]. In contrast, mothers with supportive marital relationships have been reported less likely to develop depressive symptoms during the postnatal period [6], [8–11].
The ability of social relationships to mediate the onset of depression is thought to act though two mechanisms: reduction of depressive symptoms themselves and/or as a buffer against the negative consequences of life stress. In the perinatal setting the effects of how spousal support (overall, communication and practical help) separated depressed from non-depressed women following childbirth has been examined [12] and has shown that each support factor was different between depressed and non-depressed women but only after one or more negative life events had occurred. This suggests that a buffering effect [11] is important in alleviating feelings of distress following stressful situations in the postnatal period.
This finding is also evident antenatally, with support received during pregnancy having positive outcomes postnatally and making adjustment to the new parenting role easier [13]. The converse also holds true: a negative reaction to a pregnancy by a partner has been shown to be predictive of depressive symptoms in women [14], [15]. Similarly, the life event of becoming pregnant is considered threatening if the pregnancy is unplanned or if the woman does not have a stable partner relationship with the father of the child [15]. This suggests that antenatally, partner support reduces maternal vulnerability to, or mediates onset of, depressive symptoms.
Thus, pregnancy and the early postnatal period are times when partner support and being in a trusting relationship may be particularly beneficial for maternal psychological health. Because women may feel more physically vulnerable and emotionally dependent on their partner after birth, the presence of a supportive partner act as a buffer against the difficulties and stresses experienced during the transition to parenthood and thereby protects maternal mental health. This being the case, it raises the question of what happens to women who embark on the maternal journey as a single parent?.
The continuing rise of single motherhood – in Australia the rate of lone-mother families with a child under 15 years rose from 16.6% in 1985 to 18.7% in 2005; in comparison lone-father families rose 1.9% to 2.7% for the same period [16] – has resulted in an increasing interest in the health and social conditions associated with this family structure. Studies have demonstrated a significant disadvantage for single mothers compared to two-parent families. Single mothers have higher rates of psychological/emotional distress, for example major depression, dysthymia, suicide and low self-esteem, than married/partnered mothers [17], [18]. This has been attributed to four key factors [19]: financial hardship, unemployment, lack of social support and sole responsibility for care of the child [20–22]. Co-factors thought to impact on the emotional health of unpartnered mothers include increased rates of smoking, problem drinking and long-term medical illness [23], [24].
The biopsychosocial model that has been proposed provides a model to understand the diversity of factors considered to play a role in maternal mental health [25]. The vulnerabilities of the individual, including personality and cognitive styles, life experiences, poor marital relationships and a previous history of mental illness all increase susceptibility to depressive symptoms. Factors that may trigger a depressive episode are stress levels and how well these can be moderated by variable of socials support and coping resources. This model would predict that a poor marital relationship increases a woman's susceptibility and that inadequate social and emotional support from the partner can serve as a precipitating factor. Thus, a women's cognitive appraisal of her support is of more importance than the objective reality of how much support she receives.
It is clear that being in a relationship with significant discord, or lack of emotional/practical support, impacts on a pregnant woman's or mother's mental health status. Likewise, evidence shows that single-mother status is also a significant risk factor for development of a mood disorder [15], [26], [27]. Thus, while the absence of a partner is certainly instrumental in the risk stratification of a mother for a mood disorder, it is equally important to consider the quality of a partnered relationship. This paper compares the impact of single-mother status and level of partner support in partnered women, as well as the influence of other known risk factors, on antenatal emotional health.
Methods
Participants and procedure
This study was a prospective, non-randomized, naturalistic design. Data were collected from women recruited to the beyondblue National Postnatal Depression Program [28]. The aim of the beyondblue Program was to gather perinatal mental health and psychosocial data from pregnant and postnatal women in five states and territories of Australia over the period 2002–2004. The present data (n=1578) represent a subset of the total Victorian cohort collected during this time.
Recruitment took place at the public antenatal clinics of the Werribee Mercy Hospital, Northern Hospital and the Angliss Hospital. These hospitals are located in metropolitan Melbourne, Victoria and serve predominately low-to-middle class areas. Data were also collected from Hamilton Base Hospital. This hospital is situated approximately 290 km from Melbourne. According to the Rural, Remote and Metropolitan Index [29], which uses population size and an index of remoteness related to distance from an urban centre, Hamilton is considered a ‘rural centre with a population of <10 000 people’. Ethics approval was granted by the respective hospital Human Research Ethics Committees before commencement of the study.
Women were first approached at their antenatal booking-in visit where the study was explained to them verbally and they were given a plain language statement and consent form. If the women agreed to participate, they completed the consent form and were given a 34-item, self-report Psychosocial Risk Factor Questionnaire (PSRFQ). An Edinburgh Postnatal Depression Scale (EPDS) was also administered at the time of recruitment. Both questionnaires were completed in 5–10 min in the clinic and once returned, data were entered on a central database.
Assessments
Psychosocial Risk Factor Questionnaire
The PSRFQ is a 34-item demographics questionnaire that was developed specifically for the present study following consensus review of the perinatal depression risk factor literature and from clinical experience. Its purpose was to obtain a psychosocial risk factor profile of the women recruited. The information collected included participant name, contact details, general practitioner details, marital status, country of birth, language spoken at home, socioeconomic status, occupation, highest level of education completed, current physical and mental health status, past history of mental illness, major life events in the past 12 months, availability of emotional/practical supports, relationship with mother and partner, baby gender desired, current level of daily hassles and history of abuse (sexual, physical and emotional).
Single-mother status was defined as any women who reported being unpartnered through non-union, divorce, separation or loss of partner through death, at time of recruitment. Any women reporting they were in a married or de facto relationship were considered partnered.
Edinburgh Postnatal Depression Scale
The EPDS was administered as a screening tool for current depression [30]. This scale is a widely used 10-item questionnaire developed for screening for postnatal depression in the community and it has good reliability and validity. A threshold score >12 was used to indicate likely major depression. This cut-off point has been shown to have 89–90% sensitivity and 82–84% specificity for detection of distressed/depressed cases in an Australian sample [31]. The EPDS has also been validated for antenatal use [32].
Statistical analysis
All statistical analysis was carried out using SPSS 14 for Windows (SPSS, Chicago, IL, USA). Three separate analyses were performed.
A binomial logistic regression of the total cohort (n = 1578) was done to ascertain the most important factors associated with single-mother status and elevated EPDS scores. The first dependent variable was dichotomized as to whether or not the women had a partner and the second was dichotomized as to whether EPDS scores exceeded 12. Seventeen independent variables were entered individually into the logistic regression analyses. Variables showing a significant association with single-mother status and/or elevated EPDS scores were entered into a backward logistic regression analysis in order to investigate mediation effects.
Antenatal EPDS scores were analysed in a one-way ANOVA for between-group differences with post-hoc pair-wise comparisons after taking a square root transformation. The ANOVA was performed on three groups of women: (i) women with no partner; (ii) partnered women who received little or no partner-derived emotional support; or (iii) partnered women who received very good or excellent partner-derived emotional support. Variance homogeneity was confirmed using a Levene's test. The assumption of normality was checked graphically using the Kolmogorov–Smirnov goodness-of-fit tests. The results of the ANOVA were validated using a non-parametric Kruskal–Wallis test.
A final sample of 62 non-partnered woman was delimited to perform further analysis. The dependent variable was the EPDS score, which was dichotomized to above or below a threshold of 12. A univariate analysis to ascertain the most significant of the 17 variables associated with a high EPDS score was performed. Multiple logistic regression was then performed on these variables.
Results
Demographic characteristics
The demographic composition of the total cohort (n = 1578), the single/unpartnered cohort (n = 62) and the elevated EPDS score cohort (n = 240) are summarized in Tables 1 and 2.
Participant demographic characteristics
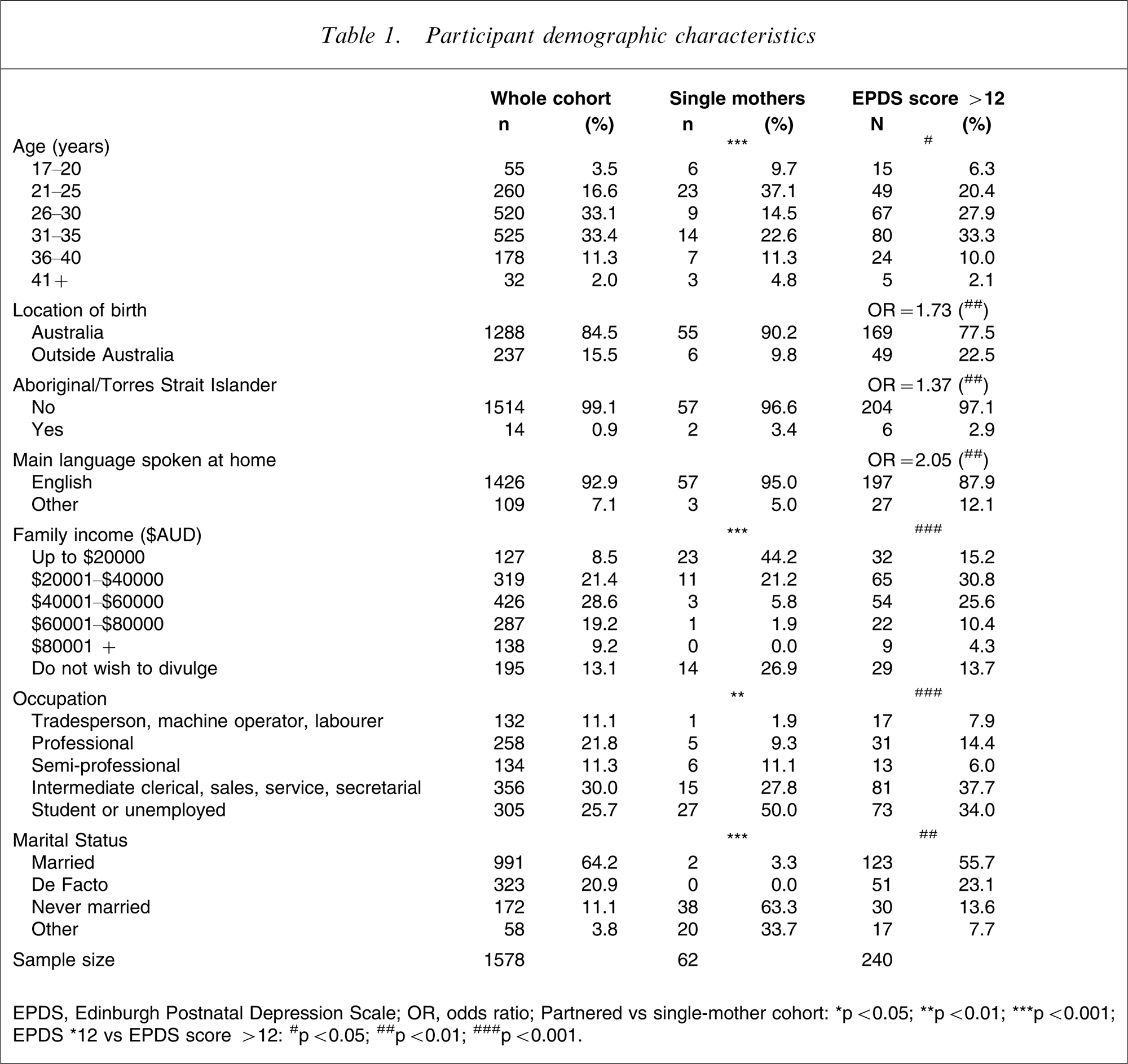
EPDS, Edinburgh Postnatal Depression Scale; OR, odds ratio; Partnered vs single-mother cohort: ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.; EPDS∗12 vs EPDS score > 12.: #p < 0.05; ##p < 0.01; ###p < 0.001.
Participant psychosocial factors
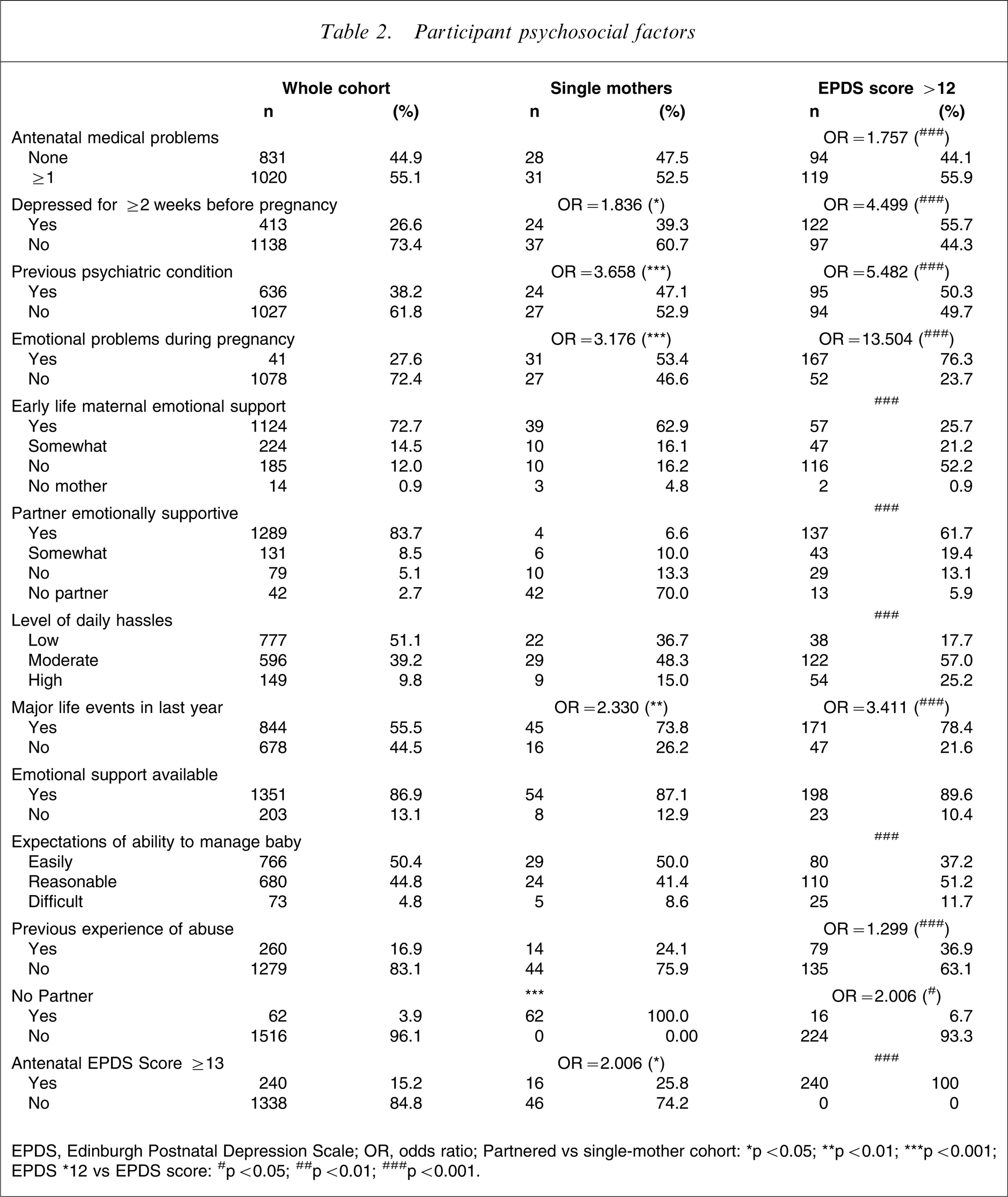
EPDS, Edinburgh Postnatal Depression Scale; OR, odds ratio; Partnered vs single-mother cohort: ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001; EPDS ∗12 sv EPDS score: #p < 0.05; ##p < 0.01; ###p < 0.001.
Total cohort
The average participant age was 30 years (range 17–48 years), with the majority (84.5%) born in Australia and in a partnered relationship (85.1%). Teenage pregnancies (mothers aged 17–20 years inclusive) accounted for 3.5% (n = 55) of the total cohort.
Single/unpartnered cohort
Of the total cohort, 62 women reported ‘no partner’ on the PSRFQ. The average age of this cohort was 27.7 years (range 17–43 years), with the largest group being those aged 21–25 years (37.1%). Women younger than 21 years of age represented 9.7% of this sample. Compared to the total cohort, the single/unpartnered sample tended to be younger (p < 0.001), with lower incomes (p < 0.001) and was more likely to be students or unemployed (p < 0.01).
Prevalence of antenatal depression
The total sample (n = 1578) of women was screened antenatally with the EPDS. Antenatal depression, classified by an EPDS score >12, was identified in 240 women, giving a point prevalence of 15.2%. The average age of these women was 29.4 years (range 17–43 years). Mothers younger than 21 years represented 6.3% (15/1578) of this sample. Women with elevated EPDS scores (Tables 1 and 2) tended to be slightly younger than the total cohort (p = 0.050) and were less likely to have Australia as their place of birth (odds ratio (OR) = 1.73, p < 0.01). They were more likely to be of Aboriginal or Torres Strait Islander descent (OR = 1.37, p < 0.01) and less likely to speak English as their main language at home (OR = 2.054, p < 0.01). In addition, they tended to be poorer (p < 0.001), less likely to have a professional job (p < 0.01) and were less likely to be in a partnered relationship (p < 0.01).
Sixty-two women were delimited from the total sample as ‘single’. Of this group, 16 scored >12 on the EPDS, giving a point prevalence of 25.8%. In comparison, 1516 women were partnered and of this group 224 scored >12 on the EPDS, resulting in a point prevalence of 14.8%. OR calculations (Tables 1 and 2) indicate that having no partner doubles the odds of a high antenatal EPDS score (OR = 2.006, 95% confidence interval (CI) = 1.12–3.61, p < 0.05).
Psychosocial and mental health status
The psychosocial and mental health status of the total cohort (n = 1578), the single/unpartnered cohort (n = 62) and the elevated EPDS score cohort (n = 240) are summarized in Tables 1 and 2.
Total cohort
More than half (55.1%) of the total cohort had experienced one or more medical problems during their pregnancy while 26.6% self-reported feelings of depression for ≥2 weeks. More than one-third (38.2%) reported a previous psychiatric condition (major/minor depression, anxiety or other) while 27.6% reported emotional problems (depression, anxiety, eating disorder, adjustment disorder or other) during the current pregnancy.
Single/unpartnered cohort
Of the single/unpartnered women, 52.5% had experienced one or more medical problems during their pregnancy while 39.3% had self-reported feelings of depression for ≥2 weeks before their pregnancy. Nearly half (47.1%) reported a previous psychiatric condition while 53.4% had experienced emotional problems during pregnancy. Compared to the partnered cohort, single/unpartnered women were more likely to have experienced ≥2 weeks of depression before the current pregnancy (OR = 1.836, p < 0.05), have had a previous psychiatric condition (OR = 3.658, p < 0.001), emotional problems during the current pregnancy (OR = 3.176, p < 0.01) and experienced major life events in the last year (OR = 2.330, p < 0.01).
A large number of psychosocial variables were strongly related to EPDS scores. In particular, the expected odds of EPDS scores >12 are significantly increased if women reported one or more medical problems during the current pregnancy (OR = 1.757, p < 0.001); feeling depressed for ≥2 weeks before pregnancy (OR = 4.499, p < 0.001); a previous psychiatric history (OR = 5.482, p < 0.001); emotional problems during the current pregnancy (OR = 13.504, p < 0.001); one or more major life events in the past 12 months (OR = 3.411, p < 0.001); or a previous history of abuse (OR = 1.299, p < 0.001).
Prediction of antenatal EPDS score in single/unpartnered women
Table 3 shows the results for the backward binary logistic regression to predict antenatal EPDS scores >12, considering all eighteen demographic and psychosocial factors, which have a significant relationship with EPDS score. This includes the ‘no partner’ variable.
Binary logistic regression with backward variable selection for antenatal EDPS > 12
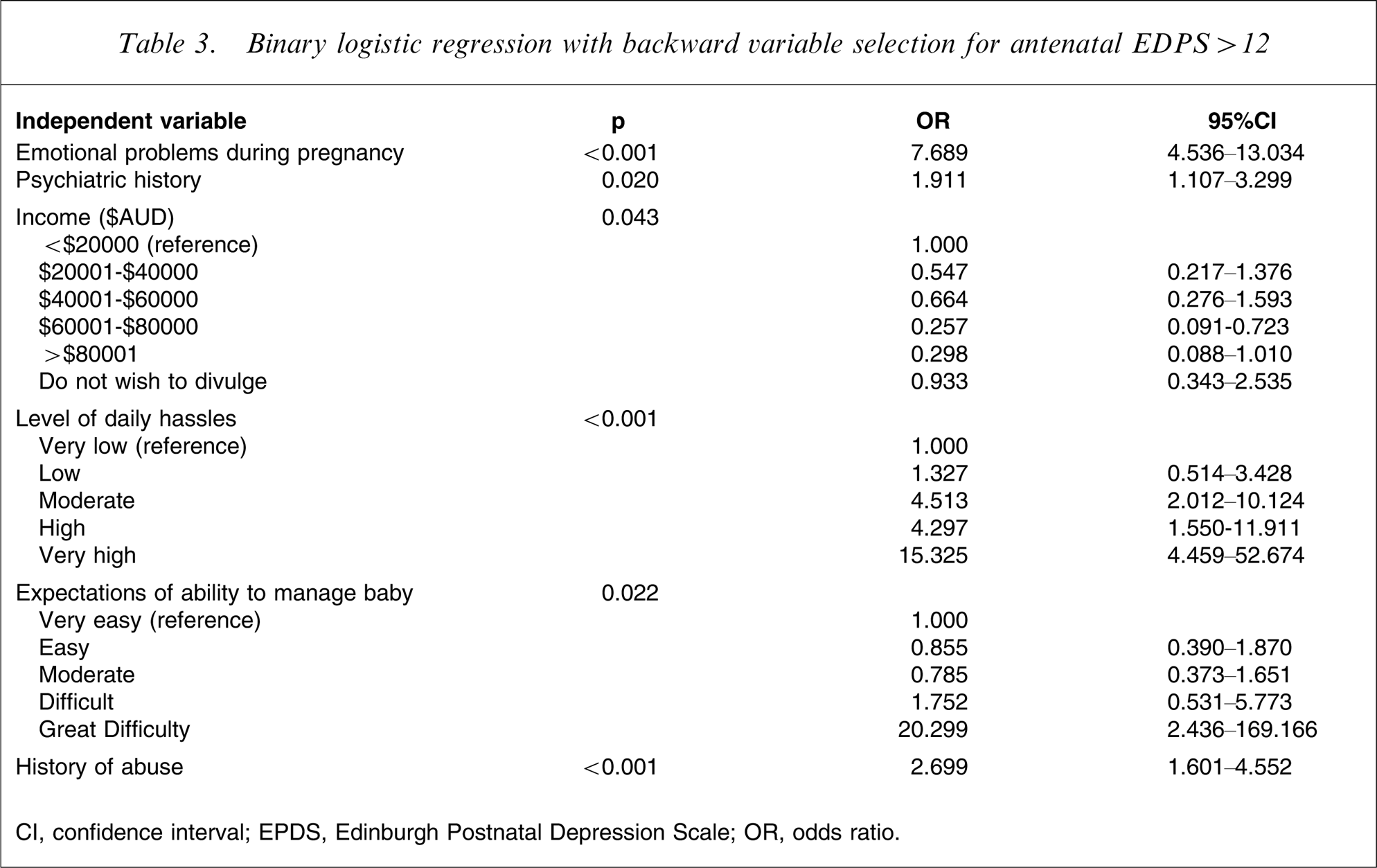
CI, confidence interval; EPDS, Edinburgh Postnatal Depression Scale; OR, odds ratio.
The effect of the ‘no partner’ variable is not significant in the backward binary logistic model, suggesting that the effect of this variable is mediated by previous psychiatric history (OR = 1.911, 95%CI = 1.107–3.299, p < 0.001) and the occurrence of emotional problems during pregnancy (OR = 7.689, 95%CI = 4.536–13.034, p = 0.02). A history of previous abuse (sexual, physical or emotional) is also strongly associated with a high EPDS (OR = 2.699, 95%CI = 1.601–4.552, p < 0.001) when the other items in the regression are statistically controlled. Level of daily hassles and maternal perceptions of baby management are suggestive of an increased likelihood of a high EPDS score, but the very wide 95%CI means that these results should be considered with caution. Income status is also important, with the lowest odds of a high EPDS score being for incomes of AuD$60 001–$80 000 (OR = 0.257, 95%CI = 0.097–0.723)
These findings suggest that the relatively high prevalence of high antenatal EPDS scores among single/unpartnered women can be attributed to their psychiatric history, emotional problems, previous abuse and, possibly, level of daily hassles, maternal perceptions of infant and/or income level, rather than single/unpartnered status itself.
The mean and median antenatal EPDS scores for each of the three groups (women with no partner, group 1; women with partners and poor support, group 2; and women with partner and good support, group 3) are shown in Table 4 (F(2,1415) = 40.706, p < 0.001). Differences between the groups were analysed on ANOVA following Levene's test to confirm equal variances in the population (F(2,1415) = 40.706, p < 0.001). This result was confirmed using a non-parametric Kruskal–Wallis test (χ2=70.985, df = 2, p < 0.001). A conservative Scheffe post-hoc test showed that antenatal EPDS scores were significantly lower for women with supportive partners than for single/unpartnered women (6.2±4.6 vs 8.9±5.3, p < 0.001). But antenatal EPDS scores were significantly lower for single/unpartnered women than for women with unsupportive partners (8.9±5.3 vs 11.9±6.5, p < 0.001), confirming that partner support is a crucial predictor for antenatal EPDS score.
Level of partner support and antenatal EPDS score
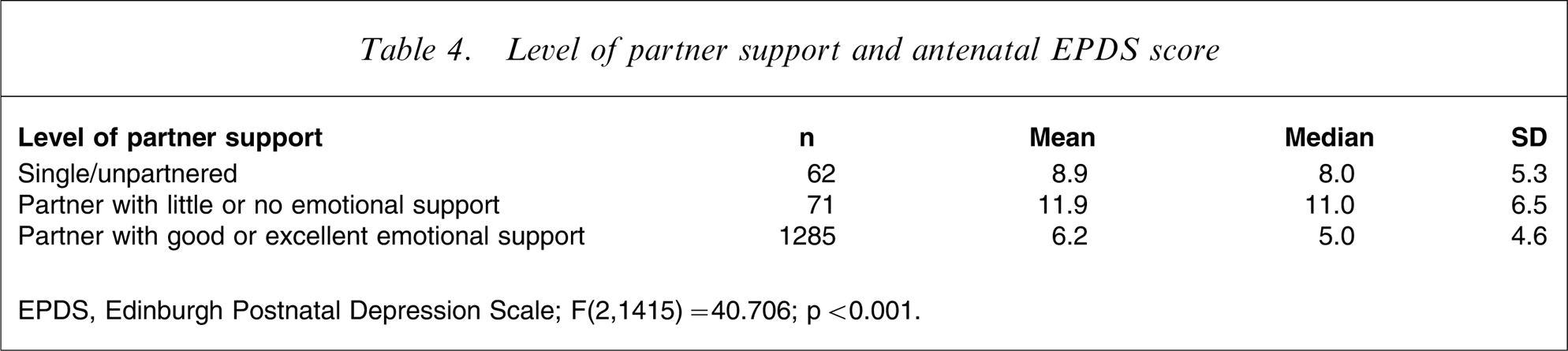
EPDS, Edinburgh Postnatal Depression Scale.
F(2,1415) = 40.706; p < 0.001.
Table 5 shows the binary logistic regression results when antenatal EPDS scores >12 are modelled for women without partners, separately for each independent variable. There are only two significant predictors in this model: having experienced at least 2 weeks of depression before pregnancy (OR = 4.571, 95%CI = 1.318–15.856); and a previous history of abuse (OR = 3.964, 95%CI = 1.047–15.012). When the depression variable is statistically controlled (Table 5), the effect of abuse becomes non-significant. This suggests that the effect of abuse, on antenatal EPDS score, is mediated through an increased likelihood of having experienced a previous depressive episode. The risk of experiencing a depression for ≥2 weeks before pregnancy is significantly increased by a past history of abuse (OR = 3.576, p < 0.001), suggesting that it is depressive episodes rather than abuse itself that is associated with high elevated EPDS score for women with partners.
Logistic regression for antenatal EDPS > 12 for mothers with no partner
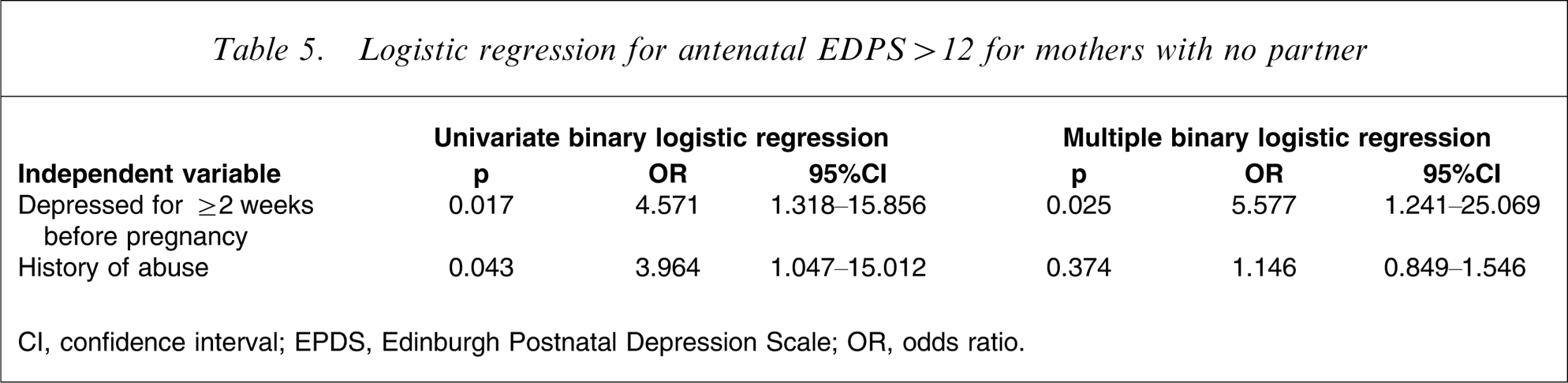
CI, confidence interval; EPDS, Edinburgh Postnatal Depression Scale; OR, odds ratio.
Discussion
Mood disorders during pregnancy and early parenthood have a multifactorial aetiology; epidemiological and meta-analysis studies have consistently demonstrated a complex interaction between experiential/environmental factors, social factors and maternal perceptions/personality [33–35]. It is clear, from studies conducted in diverse settings with various measurements and assessment periods, that a woman's relationship with her partner, in particular, is significantly associated with mental health outcomes during the perinatal period. Given this recurring link, greater understanding of the influence of partner support on maternal mental health may assist health professionals in the development of early intervention and treatment strategies.
This study is the first to directly compare marital status, levels of partner-derived support and mental health status in pregnant women. It found that women in a partnered relationship with poor partner-derived support had higher mean EPDS score in the antenatal period than single, non-partnered women. It also found that for single women, a previous history of depression and current emotional problems, rather than single mother status itself is a significant risk for elevated EPDS scores antenatally.
Several authors have found the prevalence of antenatal depression similar to that of postnatal depression [36–38] and results from the present study for the total cohort (15.2%) confirm this. However, the prevalence of elevated antenatal EPDS scores in the single cohort was extremely high, with just over 25% having a score >12, compared to only 14.8% in the partnered cohort. This finding is in keeping with the observation that single mothers have a poorer mental health status than partnered women [17], [18], [39]. The reasons for this may be varied; for example, single mothers are much more likely to have been exposed to childhood sexual and/or partner violence [22], [40] and are more likely to have an unsettled domestic situation [22], and the correlation of these events with a range of psychiatric disorders may explain the finding that a previous psychopathology and/or stressful life events, rather than being just simply unpartnered, is associated with an antenatal mood disorder.
Despite the higher prevalence of elevated EPDS score in the single-mother cohort, this study confirms that partner support is a crucial mediator for antenatal mental health. This is highlighted in the finding that unpartnered mothers had lower mean EPDS scores than partnered mothers with poor partner-derived support. This suggests that at least antenatally, being single results in better mental health than being in a poor relationship, and that lacking a partner may not be as important as during the postnatal period. Unfortunately, because postnatal EPDS scores were not collected in the present study, it is not possible to verify this latter hypothesis. However, the stereotype that a two-parent family results in better mental health outcomes is challenged by these findings, which suggest that a single-parent family is a better influence on maternal health than a poor mother–father interpersonal relationship.
One of the factors often associated with the mental health status of single mothers is their poor socioeconomic status. Backward binary logistic regression confirms that in the current model, income is a significant predictor of elevated antenatal EPDS scores. Postnatally, Beck found only a small relationship between financial resources and postnatal depression [34]. The reason for this may be related to perceptions of financial adequacy rather than income level. Similarly, perceived financial stress may be a better measure of the impact of socioeconomic factors on maternal mental health. However, lack of socioeconomic resources has been implicated in increased risk for postnatal depression [41], and rates of depression range from 23% to 38% among women with limited economic resources [42], [43]. It is also worth considering that the impact of financial stress may become more evident in the postnatal period, when the significant financial costs associated with caring for an infant, and the stress caused when financial resources are tight, is increased. It is at this time, when a new single mother is likely to be unable to work, when maternity benefits cease and savings are eroded, that this becomes an important factor in maternal mental health outcomes. Limited finances also impact on a new mother's ability to be involved in a range of community activities and socialization, known to improve maternal well-being.
The present findings add weight to calls for the introduction of routine procedures to screen/assess women for psychosocial risk factors in the antenatal period [44], [45] and highlight the need not only to ask pregnant women whether they have a partner, but also about levels of available support. We have previously shown that woman find screening of psychosocial factors an acceptable part of routine perinatal care [28]. It is clear that consideration of maternal mental health is an important part of holistic antenatal care. This is particularly important because poor maternal mental health will impact on the quality of parenting provided and mother–infant relationships and attachment, two factors crucial for optimal infant development [46]. Identification of psychosocial and socioeconomic risk factors may help facilitate early intervention in these women through treatment of current distress, preventing development of postnatal mood disorders or limiting their long-term consequences. Any screening procedures should include an assessment of the quality of the partner relationship. This is important because a poor partner relationship is a significant risk factor for depression chronicity [47], and a decline in the marital relationship during pregnancy is a significant risk factor for chronic mental illness problems [48]. Without appropriate and timely intervention and support, transgenerational patterns of mental illness may continue to be repeated.
The limitations of the present study provide the basis for further work in this area. As discussed, postnatal EPDS scores were not collected, so it is not possible to determine whether the antenatal risk factors described here impacted on postnatal mental health outcomes. It is important to note that use of the EPDS in the present study was to determine current (i.e. antenatal) mental health, rather than as a predictive tool. This study did not discriminate or compare between the different types of support – emotional, physical and financial – that a partner provides; it focuses on perceived support. Evidence suggests that affective support, or lack thereof, is strongly associated with a poor maternal response to stressful situations rather than functional support [48]. Investigation of the women's perceptions of the type of support provided may help to clarify this. Likewise it has been shown that even though a woman many feel supported by her partner, if this support is provided in the presence of persistent conflict with the infant's father, adverse outcomes are more likely [49], [50]. Clarifying the quality of the relationship as well as the type and quantity of support, may be important delineators of the importance of the partner on maternal health outcomes and the transition to parenthood.
Conclusion
The present results suggest that although single mothers have a higher incidence of depressive symptoms in the antenatal period than partnered women, this is not related to their single marital status per se, but is due to underlying psychosocial risk factors: previous psychopathology, current emotional health problems and past history of abuse. Results also suggest that being in a relationship with poor partner-derived support is a greater risk for antenatal mental health than being a single mother. Because of the known impact of poor antenatal mental health on parenting efficacy and infant attachment postnatally, identification of psychosocial and socioeconomic risk factors, including the quality of partner support, is strongly advocated.
Footnotes
Acknowledgements
This study was funded as part of the beyondblue National Postnatal Depression Program 2001–2005. We thank the hospitals and obstetric staff involved for allowing collection of the antenatal data, and the women who participated for sharing this information with us.