
Abstract
Keywords
In a study of Australian general practitioners (GPs), threat of litigation was perceived as the most severe work-related stress [1]. As a group, doctors overestimate the likelihood of being sued [2, 3], while the majority of patients entitled to make a formal complaint or claim compensation do not [4, 5].
A complaint or lawsuit against a doctor causes emotional and physical stress [6, 7]. This has been observed ≥2 years after being sued, regardless of outcome [8]. Issues influencing the doctor's response include personality, professional or personal supports, and the medical culture of infallibility [9–15]. More generally, the fear of litigation impacts on the practice of medicine in both a negative and a positive way. Although it may increase awareness of risk, it may also discourage open discussion and introduction of measures to reduce error, and even increase health-care costs, such as through unnecessary tests or referrals.
The frequency of medico-legal matters varies by gender, age, specialty, hours worked and country of practice, such that men aged 40–60 years working in high-intervention specialties are more likely to be the subject of a medico-legal matter [16–19]. In Australia, during the year 2005–2006, 4% of members of the largest Australian medical defence organization, United Medical Protection (United), incurred a claim for compensation [20]. In the state of New South Wales (NSW), 5% of doctors have a complaint made about them to the NSW Health Care Complaints Commission (HCCC) per year [21–23]. In the USA, 86% of high-risk specialist doctors had been named in a malpractice suit at least once [17].
Predictors of psychiatric illness in doctors include family history of mental illness, personality type (particularly neuroticism), and contextual factors such as perceived work conditions and stress outside of work [24–26, 26].
The relevance of this research to psychiatrists is threefold: first, in the treatment of a colleague who is involved in a medico-legal matter, second, as doctors who have (or may have) a complaint or suit against them, and third, as teachers of students and trainees about this aspect of professional life.
The aim of the present study was to explore the differences in psychological morbidity between GPs who have and have not had experience of medico-legal matters using several psychological health measures, with consideration to demographic and personality variables. Stress experienced by patients has been addressed elsewhere [27].
Methods
A descriptive comparative design was used. In May 2006 a cross-sectional self-report survey was administered to GPs.
Sample
A total of 1499 GPs was selected from a listing of all GPs who were currently insured with United. The sample included all 530 GPs classified by United as proceduralists (those who perform procedures of a more invasive or high-risk nature, such as obstetrics, general or regional anaesthesia, i.v. sedation, minor orthopaedic surgery, tonsillectomy), and a random selection of 970 non-procedural GPs from a total of 6479. One subject survey pack was sent back with the code removed, and 10 were returned unopened due to change of address.
Because we were seeking to use existing data within United's database (to reduce data burden) and to collect additional information via survey, a two-stage approach was used to ensure protection of United members’ confidential data. All selected GPs were informed about the study, including the use of historical data relating to medico-legal matters held by United, and were asked to complete a form noting if they wished not to participate in the study. Two hundred and sixty GPs (17%) requested not to participate and were therefore not included. The remaining 1239 GPs were sent the survey, with ultimately 566 respondents (45.7% survey response rate).
Data and procedure
Psychological morbidity was the outcome of interest (measured by psychiatric symptoms, disability and potentially hazardous alcohol use).
Data for analysis was obtained from two sources. First, survey data (the major data source) included demographic information (birth, gender, year and country of graduation, type of general practice, marital status, hours worked per week, weeks worked per year, attendance at peer review and hours at formal education), current and past medico-legal matters, personality assessment, and psychological morbidity measures.
Second, data were extracted from the United Oracle database on medico-legal matters for those GPs who agreed to participate. This included all medico-legal matters, or matters arising from members’ medical practice that had given rise to legal action such as a claim for compensation, a complaint before a medical registration board or complaints body, coronial inquiry, or allegation of Medicare fraud and other billing irregularities (Table 1). A unique study code was used to combine the extracted United data with the survey data received. A listing of the study codes was obtained from the survey data returned and only United data relating to members representing these study codes were issued to the team.
Subject characteristics
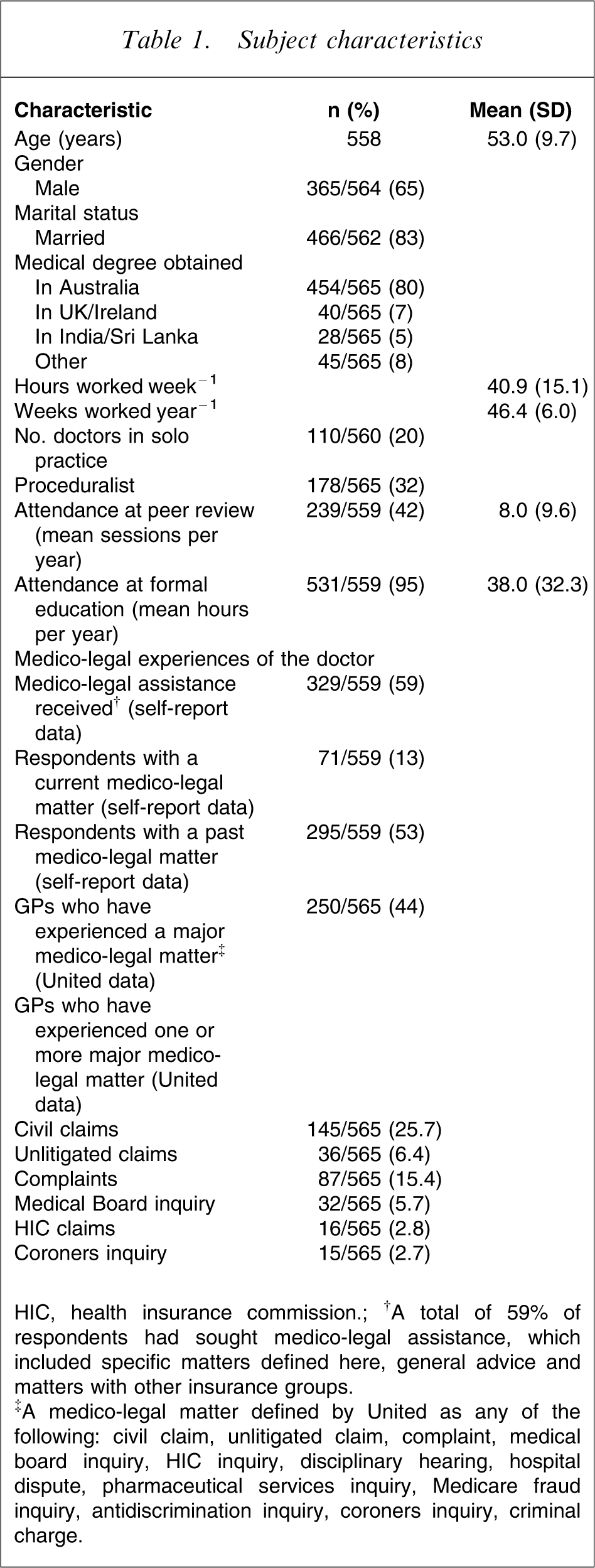
HIC, health insurance commission.;†A total of 59% of respondents had sought medico-legal assistance, which included specific matters defined here, general advice and matters with other insurance groups.
‡A medico-legal matter defined by United as any of the following: civil claim, unlitigated claim, complaint, medical board inquiry, HIC inquiry, disciplinary hearing, hospital dispute, pharmaceutical services inquiry, Medicare fraud inquiry, antidiscrimination inquiry, coroners inquiry, criminal charge.
The self-administered survey was posted to GPs and included a reply paid envelope. Four weeks later, a reminder letter was issued, again requesting participation and return of the survey.
Measures of psychological morbidity
Psychiatric morbidity was assessed using the General Health Questionnaire-28 (GHQ) [28], a sensitive and well-validated screening tool to detect common non-psychotic psychiatric morbidity that considers symptoms over the past 2 weeks. It has four subscales: somatic symptoms; anxiety and insomnia; social dysfunction; and depression. There are two scoring systems used: a summation of scores (scores from 0 to 3 per item, with higher number for increasing symptom severity) giving a total score, and a ‘case identification’ for psychiatric morbidity using binary scoring (0011) per item, with a score >4 meeting case definition.
Impairment in work, social and family life was measured using the Sheehan Disability Scale (SDS) [29], a self-report questionnaire that assesses functional impairment in work, social/leisure activities and family life. It is a sensitive tool for identifying (primary care) patients with mental health-related impairment. In the present study it was used to identify individuals with impaired role functioning in the three domains using a modified 4-point Likert scale for each domain (1 = not impaired to 4 = severely impaired), with summation of scores for a global SDS score.
Alcohol use was assessed using the World Health Organization Alcohol Use Disorders Identification Test (AUDIT) [30], which is sensitive to detecting hazardous and harmful drinking. The AUDIT questions are scored from 0 to 4, with subjects who score a total of ≥8 classified as potentially hazardous drinkers (AUDIT case identification).
Personality measure
The Eysenck Personality Questionnaire (EPQ)– Revised Short Scale version [31] was used. The EPQ is a valid and reliable self-report questionnaire that measures three major dimensions of personality: extraversion (E), neuroticism (N) and psychoticism (P), representing personality traits not diagnoses. Neuroticism is sometimes referred to as ‘emotionality’ and measures emotional stability or sensitivity; psychoticism measures ‘tough-mindedness’ and at the extreme a lack of empathy. The extroversion (E) scale determines if the subject is outgoing and talkative, and a low score represents introversion.
Definition of medico-legal matter
Respondents were asked, ‘Have you ever received assistance from any medical defence organization in a medico-legal matter?’. These matters included a claim for compensation for damages, complaint to an HCC body, medical board inquiry, disciplinary hearing, health insurance commission inquiry, hospital dispute, pharmaceutical services inquiry, Medicare fraud inquiry, anti-discrimination board inquiry, coronial inquiry and criminal charge. These matters were identified as either ‘current’ or ‘past’ (the latter referring to medico-legal matters that were closed or finalized). Respondents were also asked the type of their most recent medico-legal matter.
Statistical analysis
Statistical analysis was undertaken using SPSS Version 12.0 (SPSS Version 15, Chicago, IL, USA). Differences between groups were assessed using independent samples t-tests for continuous variables, and χ2 tests for categorical variables. Bivariate relationships between continuous variables were performed using Pearson product-moment or Spearman's rank order correlation coefficients. Binary logistic regression analyses were performed to determine if medico-legal matters were associated with psychiatric morbidity and potentially hazardous drinking after controlling for relevant confounding variables.
Ethical considerations
Approval for the study was granted through Northern Sydney Central Coast Area Health Service and the University of Sydney Ethics Committees, and United Board. Anonymity and confidentiality of survey responses, and United membership and data, were protected at all times. The survey contained a covering letter indicating that de-identified data relating to medico-legal matters held by United would be issued to the study team if the survey data were returned. The study was funded by a research grant from Northern Sydney Health.
Results
Characteristics of respondents
Demographic and medico-legal history of the sample is reported in Table 1.
Characteristics of those who had experienced a medico-legal matter (self-report data)
Respondents who had ever experienced medico-legal matters were significantly older (mean = 53.96 years, SD = 9.25) than those who had never experienced a medico-legal matter (mean = 51.26 years, SD = 9.84; t(549)=3.28, p < 0.001).
Respondents who had ever experienced medico-legal matters worked significantly longer hours per week (mean = 43.08 hours, SD = 14.91) than those who had never experienced a medico-legal matter (mean = 37.64 hours, SD = 14.29; t(535)=4.16 p < 0.001), and respondents who had a current medico-legal matter worked significantly longer hours per week (mean = 46.03 hours, SD = 14.84) than those without a current matter (mean = 39.96 hours, SD = 14.99; t(529)=3.14, p < 0.01).
A significantly higher proportion of proceduralists had ever experienced a medico-legal matter (69.3%) than non-proceduralists (53.9%; χ2=11.78, df = 1, p < 0.001), and a significantly higher proportion of male (65.7%) than female respondents (46.5%) reported experiencing a medico-legal matter (χ2=19.44, df = 1, p < 0.001). However, there was no difference in the proportion of male and female respondents who worked more than 48 h per week in terms of number of medico-legal matters (p > 0.05).
Hours of work was significantly and positively correlated with number of medico-legal matters according to self-report data for both female (r = 0.25, p < 001) and male respondents (r = 0.15, p < 0.01), and according to data provided by United for both female (r = 0.25, p < 0.001) and male respondents (r = 0.16, p < 0.01).
Australian doctors versus those trained in other countries did not differ in number of medico-legal matters, nor did doctors who attended peer review or formal education differ from those who did not attend (p > 0.05).
Type of medico-legal matter
Considering respondents’ most recent medico-legal matter, according to self-report data 44.5% were claims for compensation, 22.9% were a complaint to an HCC body, 6.1% was general advice, 6.1% was classified as ‘other’, 4.6% were coronial inquiries, 4.3% medical board inquiries and 4.3% were complaints to the doctor.
Differences between study respondents and non-respondents (United Data)
United staff examined differences in demographic factors and medico-legal matters between survey respondents (n = 566) and non-respondents (n = 673). Respondents were older (mean = 52.80 years, SD = 9.46) than non-respondents (mean = 51.68 years, SD = 9.87; t(1191)=1.99, p < 0.05).
The proportion of females to males who responded (35.8%) was higher than the proportion of females to males who did not respond (28.3%; χ2=7.85, df = 1, p < 0.01).
Of the doctors who were sent the survey, there was a smaller proportion of proceduralist respondents (31.5%) compared to non-proceduralist non-respondents (38.6%; χ2=7.72, df = 1, p < 0.01).
There were no significant differences in the proportion of survey respondents experiencing the key medico-legal events (claims, complaints or inquiries) compared to non-respondents (p > 0.05).
Level of agreement between self-report data and United data on medico-legal matters
Ninety per cent of GPs who had a current or past medico-legal matter recorded by United recorded a current or past matter in self-report data. Pearson's product–moment correlations showed that there was a significant relationship between total number of current and past medico-legal matters recorded by United, and total number of current and past matters reported by the GPs (r = 0.36, p < 0.001). However, 34% of GPs who did not have a medico-legal matter recorded by United, did record a matter in self-report data. This was likely due to the fact that respondents were asked to include all matters, either with United or other organizations, and possible over-inclusion referring to a process as a medico-legal matter that United did not regard as such.
Psychological measures
Psychiatric morbidity (General Health Questionnaire)
Those doctors who had ever experienced a medico-legal matter had significantly higher psychiatric morbidity case identification rates than doctors who had never experienced medico-legal matters (χ2=5.90, df = 1, p < 0.005). Further GHQ results are given in Table 2.
Mean total instrument scores
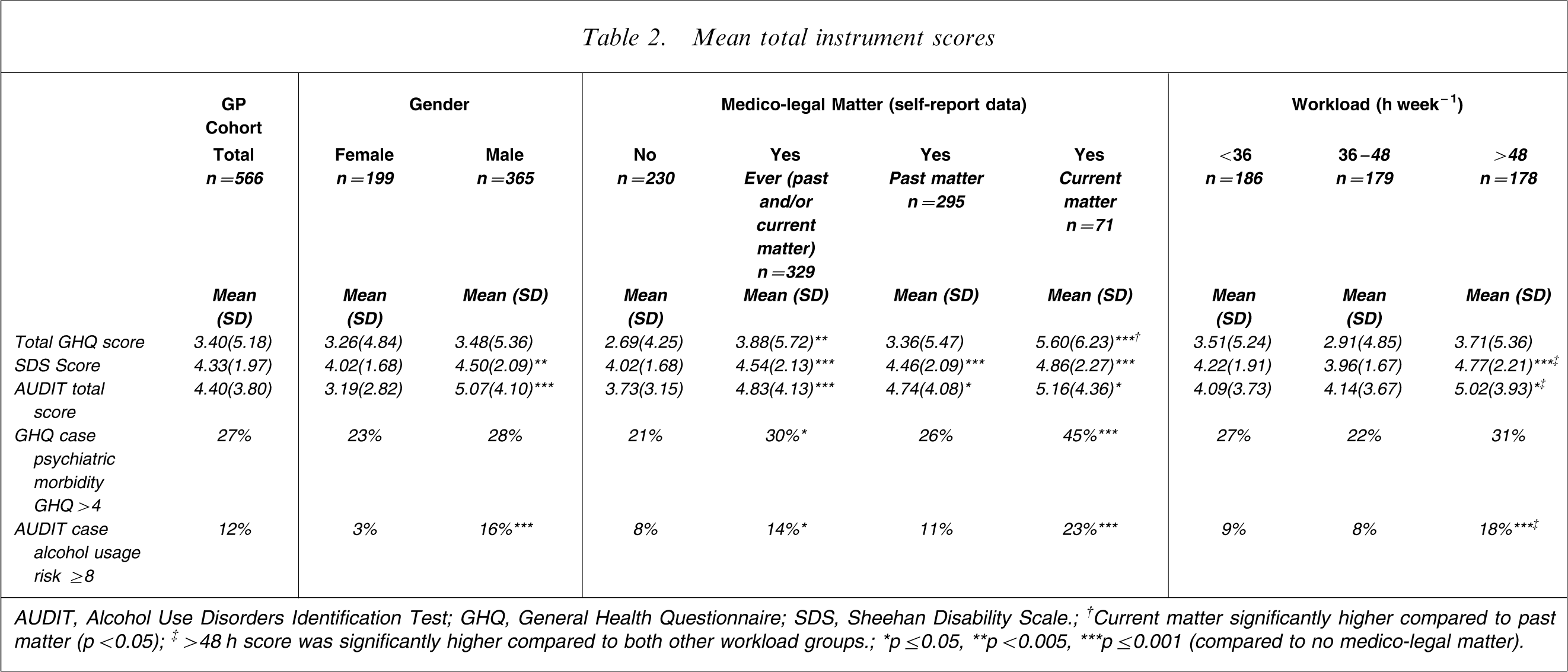
AUDIT, Alcohol Use Disorders Identification Test; GHQ, General Health Questionnaire; SDS, Sheehan Disability Scale.; †Current matter significantly higher compared to past matter (p < 0.05); ‡>48 h score was significantly higher compared to both other workload groups.; ∗p ≤ 0.05, ∗∗p < 0.005, ∗∗∗p ≤ 0.001 (compared to no medico-legal matter).
Compared to doctors who had never experienced a medico-legal matter, those who had ever experienced a medico-legal matter reported higher anxiety (t(542)=3.24, p < 0.005), greater social dysfunction (t(551)=3.17, p < 0.005), and a higher level of depression (t(549)=3.21, p < 0.001), and doctors with finalized past matters maintained a higher level of depression than those who had never experienced a medico-legal matter (t(472)=2.86, p < 0.005). Table 2 shows further comparisons for past matter only and current matters versus the group who had never sought assistance for a medico-legal matter.
Impairment (Sheehan Disability Scale)
Those doctors who had ever experienced a medico-legal matter had significantly higher disability scores than those who had never experienced a medico-legal matter (t(542)=3.24, p < 0.005). As seen in Table 2, male respondents had significantly higher disability scores than female respondents (t(475)=2.91, p < 0.005). Those who worked >48 h week–1 had significantly higher disability scores than those who worked <36 h week−1 (t(345)=2.48, p < 0.05) and those who worked 36–48 h week–1 (t(326)=3.86, p < 0.001).
Alcohol use (AUDIT)
As shown in Table 2, of those who met AUDIT criteria for being a potentially hazardous drinker (AUDIT > 8), a significantly higher proportion were male
Age differences were also examined but not found to be significant (p > 0.05).
There was a significant positive correlation between total AUDIT scores and SDS scores (r = 0.19, p < 0.001).
Difference between peer review attendance and proceduralists on morbidity measures
There was no difference in psychiatric morbidity (GHQ) or disability (SDS) or AUDIT scores between those who did or did not attend peer review, and between proceduralists and non-proceduralists (p > 0.05).
Personality (EPQ) and measures of psychological morbidity (GHQ, SDS, AUDIT)
Total GHQ scores were significantly correlated with EPQ neuroticism subscale scores (r = 0.47, p < 0.001), and EPQ introversion subscale scores (r = 0.21 p < 0.001).
Total SDS scores were significantly correlated with EPQ neuroticism subscale scores (r = 0.45, p < 0.001), and EPQ introversion subscale scores (r = 0.24, p < 0.001).
Potentially hazardous drinking scores were significantly correlated with EPQ psychoticism subscale scores (r = 0.12, p < 0.01), and EPQ neuroticism subscale scores (r = 0.10, p < 0.05)
Predictors of psychiatric morbidity and potentially hazardous drinking
Psychiatric morbidity (General Health Questionnaire)
Age, years of practice as a GP, and EPQ neuroticism and extraversion/introversion subscale scores were significant confounds and were therefore treated as covariates. These were significant predictors of psychiatric morbidity (χ2=80.68, df = 4, p < 0.001, Nagelkerke R2=0.22). Correct classification rates were 28.8% for GPs with psychiatric morbidity and 93.4% for GPs without psychiatric morbidity (the overall correct classification rate was 76.3%).
As shown in Table 3, a higher proportion of GPs with a current medico-legal matter had psychiatric morbidity than GPs without a current medico-legal matter. Current medico-legal matter significantly predicted psychiatric morbidity. There was improvement in classification of GPs with psychiatric morbidity when adding current medico-legal matter as a predictor of psychiatric morbidity. Furthermore, the exponential beta (odds ratios) statistics in Table 3 indicate that GPs who had a current medico-legal matter were more likely to have psychiatric morbidity than those without a current medico-legal matter.
Binary logistic regressions: current medico-legal matters as predictors of psychiatric morbidity (GHQ case identification) and potentially hazardous drinking (AUDIT case identification)
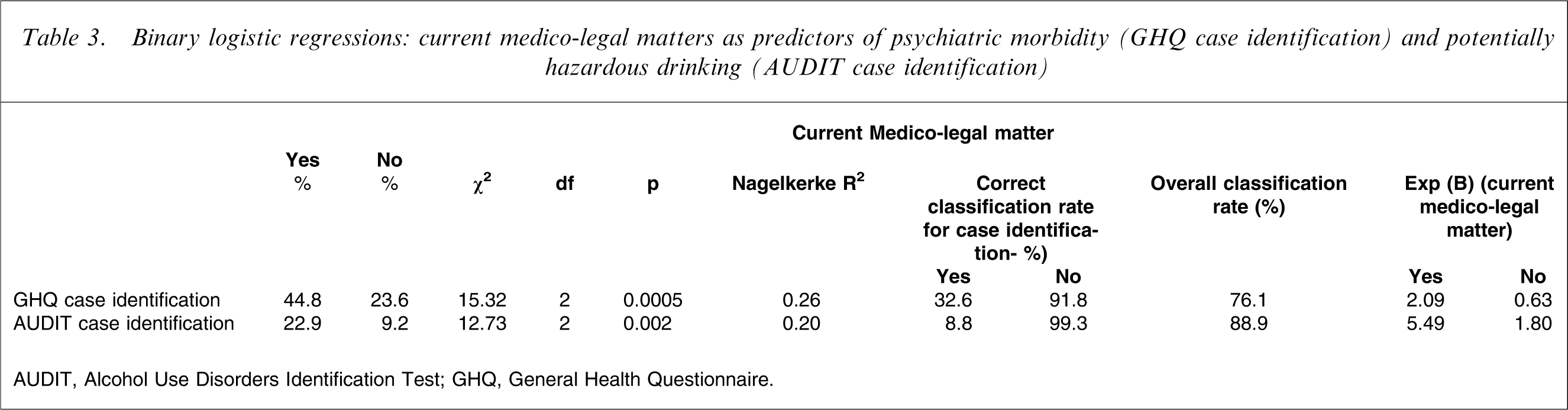
AUDIT, Alcohol Use Disorders Identification Test; GHQ, General Health Questionnaire.
Potentially hazardous drinking (AUDIT)
Gender, years of practice as a GP, hours worked per week, and EPQ psychoticism and neuroticism subscale scores were significant confounds and were therefore treated as covariates. These were significant predictors of potentially hazardous drinking (χ2=41.17, df = 5, p < 0.001, Nagelkerke R2=0.16). Correct classification rates were 1.8% for GPs with potentially hazardous drinking and 99.8% for GPs without potentially hazardous drinking (the overall classification rate was 88.5%).
As shown in Table 3, a higher proportion of GPs with a current medico-legal matter demonstrated potentially hazardous drinking than GPs without a current medico-legal matter. Current medico-legal matter significantly predicted potentially hazardous drinking. There was improvement in classification of GPs with potentially hazardous drinking when adding current medico-legal matter as a predictor of potentially hazardous drinking. Furthermore, the exponential beta (odds ratios) statistics shown in Table 3 indicate that GPs who had a current medico-legal matter were more likely to have potentially hazardous drinking than those without a current medico-legal matter.
Discussion
We have explored differences in psychological morbidity in Australian GPs, comparing those who have and have not experienced medico-legal matters, and found that there is an increase in psychiatric morbidity (GHQ), impairment in function (SDS) and alcohol use in men (AUDIT), for doctors who currently have a medico-legal matter. As in other studies [10–14], procedural doctors and those who work more hours per week are more likely to have had a medico-legal matter.
Female general practitioners in the present study had lower levels of psychological morbidity even after considering hours of work. This is contrary to previous Australian studies, which have found female doctors to have higher GHQ case identification rates (Table 4) [24, 32]. However, the present sample of GPs in general had lower psychiatric morbidity as compared to interns and hospital consultants.
Prevalence of psychiatric morbidity in Australian doctors
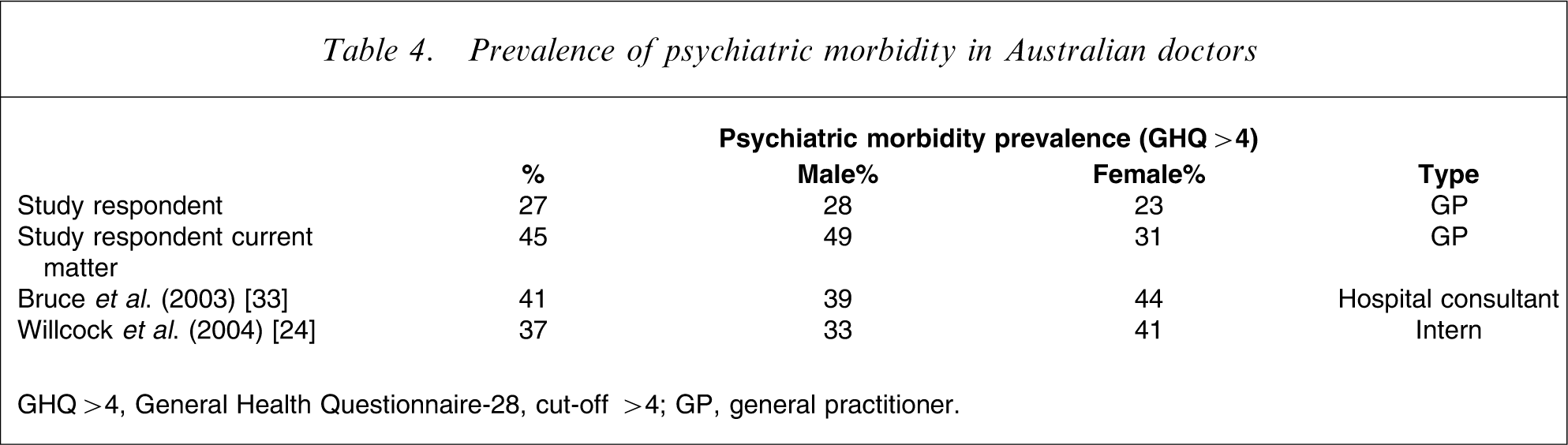
GHQ > 4, General Health Questionnaire-28, cut-off >4; GP, general practitioner.
In view of the high prevalence (45%) of GPs experiencing psychiatric morbidity with a current medico-legal matter, there is an urgent need to investigate avenues to assist doctors. This may have benefits for the practitioner, the patient, the health system and the insurer. Interventions to consider include the provision of appropriate services and education of the workforce regarding the different medico-legal processes, psychological reactions, negative coping strategies such as overuse of alcohol, and the availability of supports and positive coping strategies.
It was hypothesized that peer review and formal education [14] would identify doctors who are better engaged with their peers and less prone to adverse outcomes. However, comparisons of doctors who attended peer review or formal education with those who did not, found no difference in the occurrence of medico-legal matters or in the presence of psychiatric morbidity, disability or potentially hazardous alcohol drinking.
Limitations
The study is not without limitations. First, the 566 respondents represent only 1% of Australian GPs (2003 workforce data) [33] and they differ in demographic and work practice measures from the 2003 workforce in which mean age of GPs was 45.7 years (present sample, mean age = 53 years), 32.6% were female in 2003 (present sample, 35%) and GPs worked an average 44.2 h week−1 (present respondent sample, 40.9 h).
Second, the response rate of 45.7% to the survey is comparable to many doctor studies, but does leave room for responder bias. We considered this in our comparison of responders and non-responders from the United data, and although there were some statistical demographic differences, these were not deemed major, and importantly there were no differences in the major groups of medico-legal matters between responders and non-responders.
Third, two data sets for medico-legal matters were utilized, and each had their strengths and weaknesses. Self-report data may have been more inclusive than United data, in that it would include matters with other insurers, but relying on responders to classify the type of medico-legal matter was difficult. At times, matters were included in self-report data that would not have been considered a medico-legal matter by United definition, and thus the self-report data was over-inclusive.
Fourth, seriousness of matters was not classified in the present paper because the number of each type of matter was small when broken down. The seriousness of a complaint from the point of view of regulators (HCC body and Medical Board) is from the patient's perspective rather than the outcome for the doctor. The present study considered the impact on the doctor, which varies depending on many factors in the doctor, for example personality, supports, the doctor's perception of the seriousness of the matter, and the actual legal process (e.g. the disciplinary process can be prolonged and uncertain, whereas the resolution process can be relatively brief and unencumbered by complex legal intervention). The mere fact of a complaint, however, can be sufficient to generate anxiety.
Fifth, as a cross-sectional study we are unable to comment on the direction of causality. A longitudinal study is planned to resolve the chicken-and-egg aspect and longitudinal effects, and address the causality of psychological morbidity.
Conclusions
The present study shows that Australian GPs who have a current medico-legal matter, have increased psychiatric morbidity, disability, and in male GPs increased potentially hazardous alcohol use.
Education of medical students as well as pre-vocational and vocational training about the nature and impact of medico-legal matters is important in improving doctors’ health and thereby patient care. Enhancing individual coping strategies and the encouragement of systemic change are hypothesized as measures to further improve the outcome for the doctor and patient.