
Abstract
Bipolar disorder is the sixth leading cause of disability in the world and, in Australia, the burden of disability is fourfold greater than that of the general Australian population [1]. Rates of substance misuse, anxiety disorders, criminal behaviour, impaired social and occupational functioning, and relationship difficulties are overrepresented in people with bipolar disorder. Of further concern, 10–20% commit suicide, which represents 12% (one in eight) of all Australian suicides and 15-fold that of the general Australian population [2, 3].
Currently, nearly 100 000 Australian adults have bipolar disorder [3]. The average duration from onset to correct diagnosis is 10 years [4, 5]. A significant proportion do not receive treatment (in the 2004 National Survey of Mental Health and Wellbeing, 32% had not received any treatment in the previous 12 months [6]), and among those who do, poor treatment adherence and inadequate self-management are common [7, 8]. Recurrent episodes of mania and depression contribute to the disease burden.
Many of those with bipolar disorder report that a turning point in their illness trajectory is a shift from feeling controlled by their condition, to taking control of it [9]. Education, self-management training and support assist individuals to self-manage their illness and to take control of it. This, in turn, has been shown to enhance medication adherence and reduce hospitalizations [10]. The challenge for health professionals lies in making the education and support available in an accessible, convenient, non-stigmatizing and timely manner, so that patients can access it as soon as possible after diagnosis and when they are ready for the information, in order to commence their journey towards gaining control of the illness.
The Internet makes available a wealth of information (although not all of it is high quality, evidence based or accurate) and health consumers are accessing it in increasing numbers. In the USA, for example, 80% of Web users have looked for health information online: this translates to 95 million adults [11]. The proportion is similar in Australia, where 66% of households have a computer at home, half of the population have access to the Internet and four out of five Internet users look for health or medical information [12]. Specifically in terms of depression, a 2000 survey in the UK found that more than one in four people would rather use the Internet for health advice and counselling about depression than visit the family doctor [13]. Two-thirds of those cited their reasons as being the ease and rapidity with which they can access advice and help on the Internet, reduced stigma/embarrassment, and not wanting a mental health record.
Computer-based therapy and educational programs have also been shown to be clinically and cost-effective [14–17] and acceptable to patients [17, 18]. However, because the use of e-mental health applications is at the discretion of the user who has the option of discontinuing easily, drop-out rates are often high in contrast with face-to-face consultations [19]. Better outcomes are associated with more exposure to Web-based education and treatment programs [20]. There is also evidence that with use of online education programs, patients take less time to absorb important information from their clinicians [21], which frees time to deal with other issues. However, debate exists about whether human support is needed to maximize the effects of online programs [22].
Despite the importance of self-management in bipolar disorder, a simple, informative online psychoeducation program offering essential evidence-based information for people with the condition has not been available. To fill the gap, health professionals, community representatives and health consumers at the Black Dog Institute developed an Internet-based bipolar education program.
This paper has two objectives. The first is to report usage data on the Online Bipolar Education Program for its first 6 months of operation, as well as user characteristics and the attrition rates for the constituent modules. The second is to provide an overview of the aims and methodology of a randomized controlled trial currently underway to evaluate the impact of the program.
Method
Online Bipolar Education Program
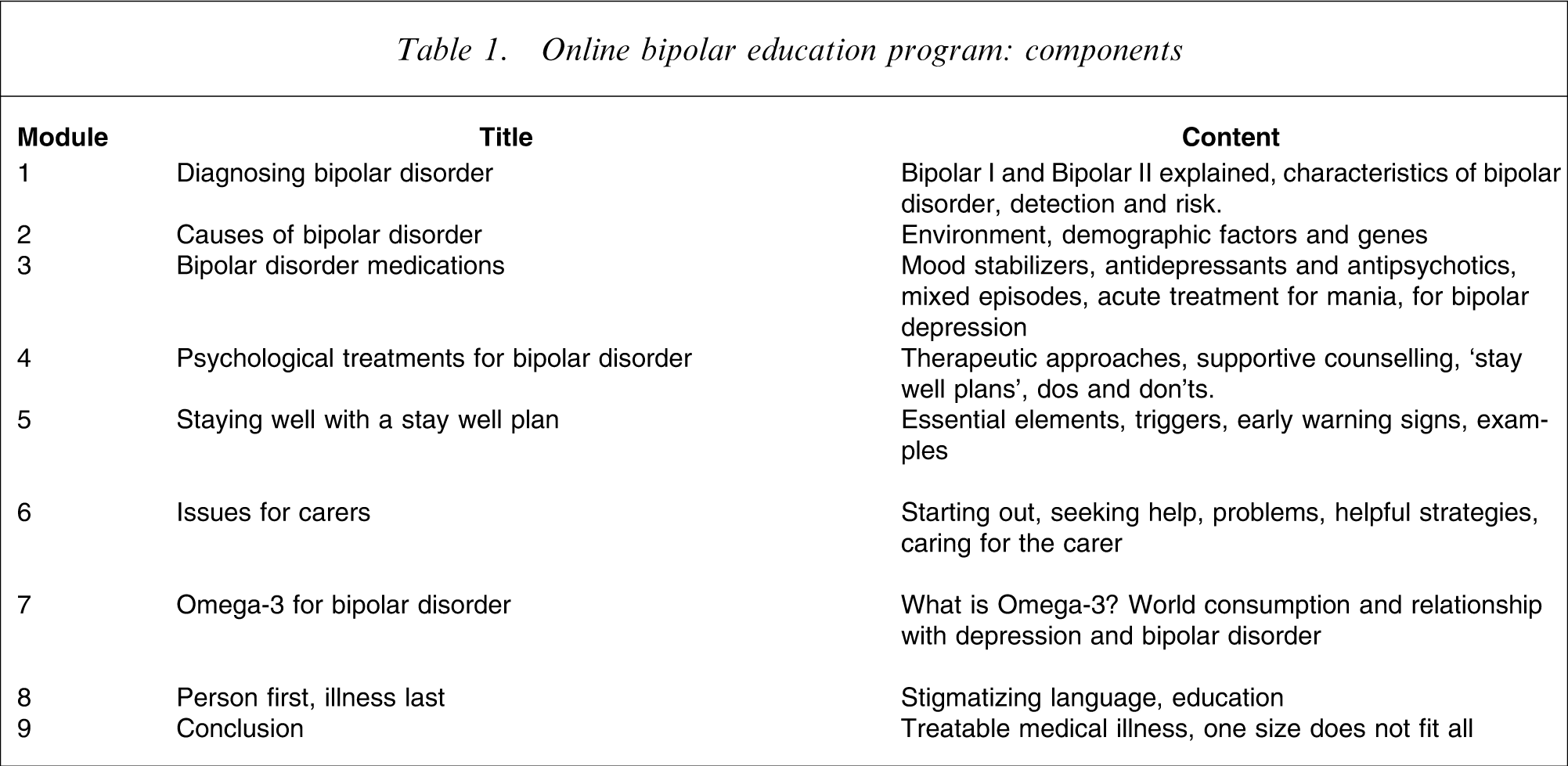
Completed in May 2006, the Online Bipolar Education Program aims to help people with bipolar disorder and their families to better understand the condition, develop effective coping strategies and enhance treatment compliance. The philosophy and intent of the program is to provide high-quality, evidence-based information about bipolar disorder, supplemented by practical advice and testimonies from people with the condition, via an accessible medium (the Web), using a clear and simple format. Designed for adults and adolescents, the material is presented in nine Web-based modules, consisting of 149 screens in total. The psychoeducational content was derived from a face-to-face program conducted at the Black Dog Institute. It is comparable to programs such as Colom et al. [23], with adaptation to online delivery (Table 1). Each module involves an audiovisual presentation from an expert in the field, an interview with the expert, a personal perspective with advice from a well-known person with bipolar disorder, and printouts (http://www.blackdoginstitute.org.au/bipolar/bep/index.cfm.). Modules vary in length from approximately 5 to 25 min, and users can access them in any order. The primary purpose of the program is information provision with some skills building; it is not designed as a psychotherapeutic intervention. It is available free of charge on the Web and in its public health usage, users are not required to log on or enter data, nor is there any screening or restriction on use.
Online bipolar education program: components
Evaluation of the Web-based bipolar education program
Consultations
We beta-tested the bipolar education program with individuals and groups of people with bipolar disorder, eliciting their structured feedback about the program in general, its online features, user interactivity, format, sequencing and potential utility. Adjustments to the program were made on the basis of the series of consultations.
Site usage
Next we developed customized Web reports on the program for the first 6 months of its operation, in order to gain an indication of site usage and utility. Data included number of visits, page views, and sessions commenced. A visit is a sequence of requests from a uniquely identified client that expires after a certain amount of inactivity, usually 30 min, while a page view is a request made to a Web server for a particular page. Both are an approximate estimate of the volume of Web traffic on the site [20]. We have also collected data on the ‘traction’ of each module, that is, the percentage of users who complete a module having started it [24]. To gain a more detailed profile of the program's users, we collected additional demographic data from new visitors to the site from 2 months after the program launch. No identifying information was sought, in order to preserve anonymity.
Randomized controlled trial
We are currently conducting a randomized controlled trial to evaluate the effect of the online bipolar education program in people diagnosed with bipolar disorder within the last 12 months. For the purposes of the trial, the program has been removed from its open Web access to a restricted access site to enhance control and prevent contamination across conditions. Inclusion criteria are age ≥18 years; diagnosis of bipolar disorder by a psychiatrist or GP within the last 12 months; access to the Internet, email and printer, and computer-literacy; residence in Australia; and ability to read and write English. Importantly for safety, individuals must have a managing health professional who is responsible for the treatment of their bipolar disorder and whom they see regularly. Potential participants are geographically screened, the Mood Swings Survey [25] is administered to ratify diagnosis and their informed consent is obtained. To prevent repeated registrations in the trial, a participant's email address is blocked after the first registration.
We are comparing two versions of the online bipolar education program: (i) on its own, and (ii) with email support from informed supporters to establish and implement a wellbeing self-management plan. Informed supporters are people with bipolar disorder who are effectively managing their condition and who are trained to provide online support for the education program under supervision of the clinical team. Research participants are randomly allocated to one of three conditions: the two psychoeducation conditions or to an attention control condition consisting of minimal online education. All online programs are delivered over 8 weeks. The bipolar education program includes tasks for participants to complete between the online sessions, to assist them to apply the information to their daily lives. Those allocated to the education program plus informed support condition receive, in addition, up to two personalized weekly emails per week from their informed supporter (max 300 words per email). Informed supporters copy all emails to JP for adherence and safety checks. An email account has also been set up to enable participants to contact the researchers if they have any questions. Participants are provided with crisis service information if issues arise. The study has been approved by the Human Research Ethics Committee of the University of New South Wales.
Primary outcome measure
The Brief Illness Perception Questionnaire [26] is a nine-item measure of individuals’ representations of their illness, each item measuring a separate subscale: Self-Control, Understanding, Treatment Control, Impact on Life, Timeline, Identity, Concern about Illness, Emotional Affect, and Causes.
Secondary outcome measures
The Work and Social Adjustment Scale [27] is a five-item Likert scale measuring the degree to which the patient's problems interfere with ability to work, home management, social life, private leisure and relationships. The possible range of scores is 0–40, with higher scores representing more functional impairment.
The Mood and Functioning Chart [28] is completed daily. This measure has the advantage of capturing mood patterns and functional impairment fluctuations across the two polar extremes. Scores are calculated to provide an index of overall mood and functioning during the previous month.
The Goldberg Anxiety and Depression Questionnaire [29] is used widely in community and medical settings; these scales consist of nine items each (possible range of scores 0–9, with higher scores representing more anxiety/depression).
A specifically-designed instrument has been developed for the present study in order to measure bipolar disorder literacy. It consists of 32 questions based on the bipolar education program and measures participants’ knowledge of the causes, diagnosis and treatments of bipolar disorder, as well as how to develop a wellbeing plan. Higher scores represent greater bipolar literacy.
The Rosenberg Self-Esteem Inventory [30] is a 10-item scale designed to measure global feelings of self-worth. The possible range of scores is 10–40, with higher scores representing higher self-esteem.
The Multi-dimensional Health Locus of Control Scale [31] is an 18-item scale consisting of three subscales: internality, powerful others and chance. The possible range of scores is 18–108.
Satisfaction with Life Scale [32]: this is a five-item questionnaire measured on a 1–7 scale from strongly disagree to strongly agree. The possible range of scores is from 5 (low satisfaction) to 35 (high satisfaction).
Measures are administered online at baseline, 9 weeks (after intervention), and at 3 and 6 months follow up. Demographic information is also collected at baseline (gender, age, country of residence, date of first diagnosis of bipolar disorder, age of first depressive episode and first high, an estimation of the pattern of their mania/hypomania and depression episodes, type of practitioner who made the diagnosis of bipolar disorder and number of previous hospitalizations for problems associated with bipolar disorder). Power calculations based on the primary outcome measure show that to detect an effect size of 0.5 between the online education program and the control group, and 0.4 between the two online programs, with a power of 80% (α = 0.05), a sample of 100 participants per group is needed. To allow for attrition, we are recruiting 125 in each group. Data are collected using enhanced confidentiality protection features, transferred via a secure virtual private network and stored on a secure firewalled server in password-protected databases. Analysis of covariance will be used with intervention as a between-subject factor, time as within-subject factor, pre-intervention symptoms and compliance with medication as covariates, and, as dependent variables, illness representations (control and understanding), illness trajectory, symptoms, bipolar disorder literacy, functional impairment, self-esteem, life satisfaction at post-intervention and follow-up assessments to analyse the data. All analyses will be on an intention-to-treat basis. Results of the randomized controlled trial will be available at the end of 2008.
Results
In the 6 months from May to October 2006, the bipolar education program recorded over 8000 visitors to the site. During this period, pages on the website were accessed 16 444 times, ranging from 29 to 661 page views per day across users (mean = 89.4). Traction across the nine modules ranged from 59% (at the beginning of May) to 98% (on the shorter modules) within months, and ranged from 64% to 94% when averaged across months, resulting in an overall rate of 76% (corresponding to an attrition rate of 24%). Data about the traction of each module are presented in Table 2.
Site usage data: May–October 2006
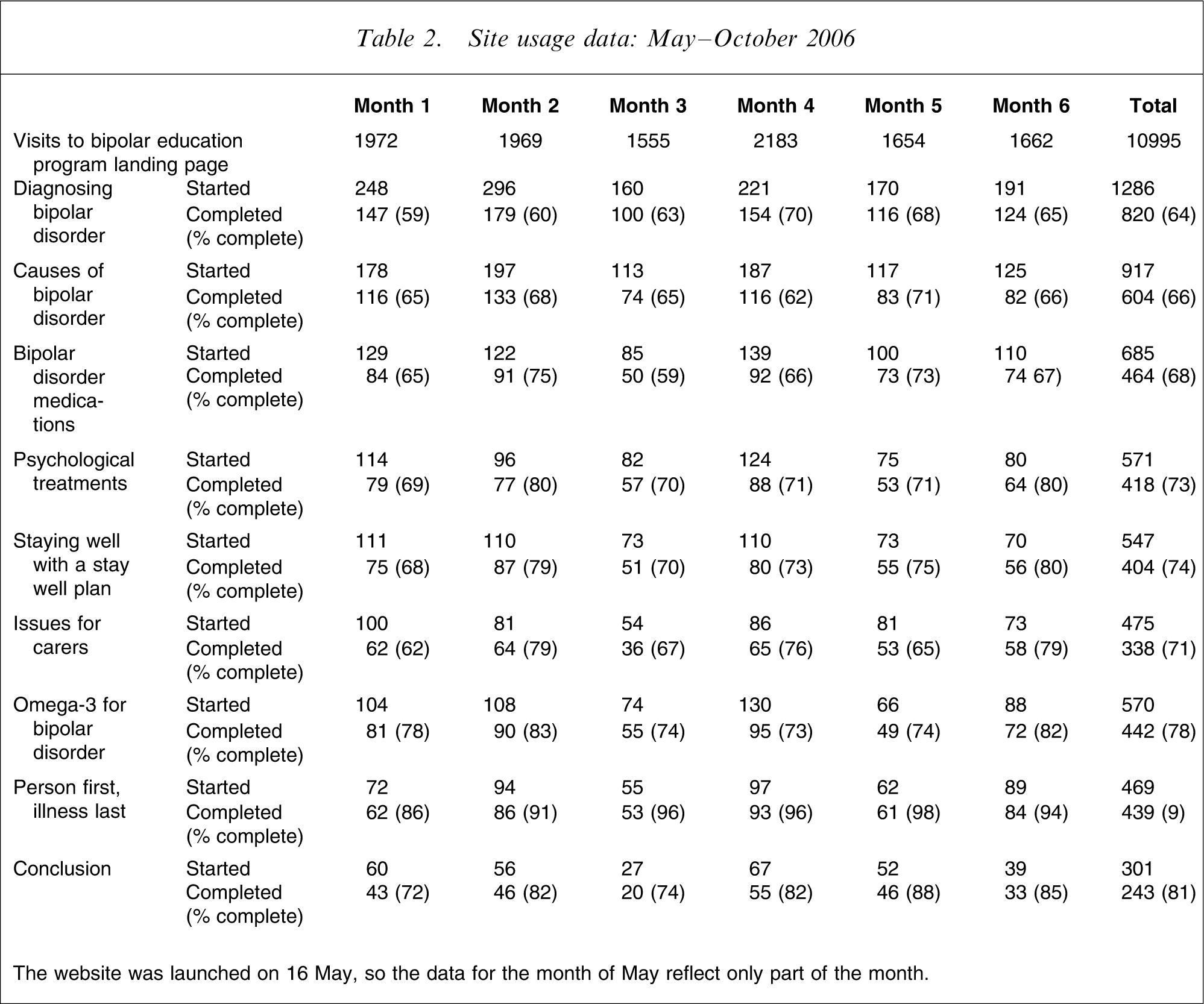
The website was launched on 16 May, so the data for the month of May reflect only part of the month.
While the majority of program visitors were from Australia (1770 page visits/month), an average of 725 page visits/month were from USA-based servers. An average of 83.15% of the bipolar education program visitors accessed the site via links from other Black Dog Institute webpages (e.g. http://www.blackdoginstitute.org.au), with the remainder accessed the site through the direct address or bookmarks, and a small percentage (0.1%) via Internet search engines. Table 2 also shows the number of sessions undertaken per module, which is an indication of the number of visitors to the module (although it must be borne in mind that visitors can go though a module more than once).
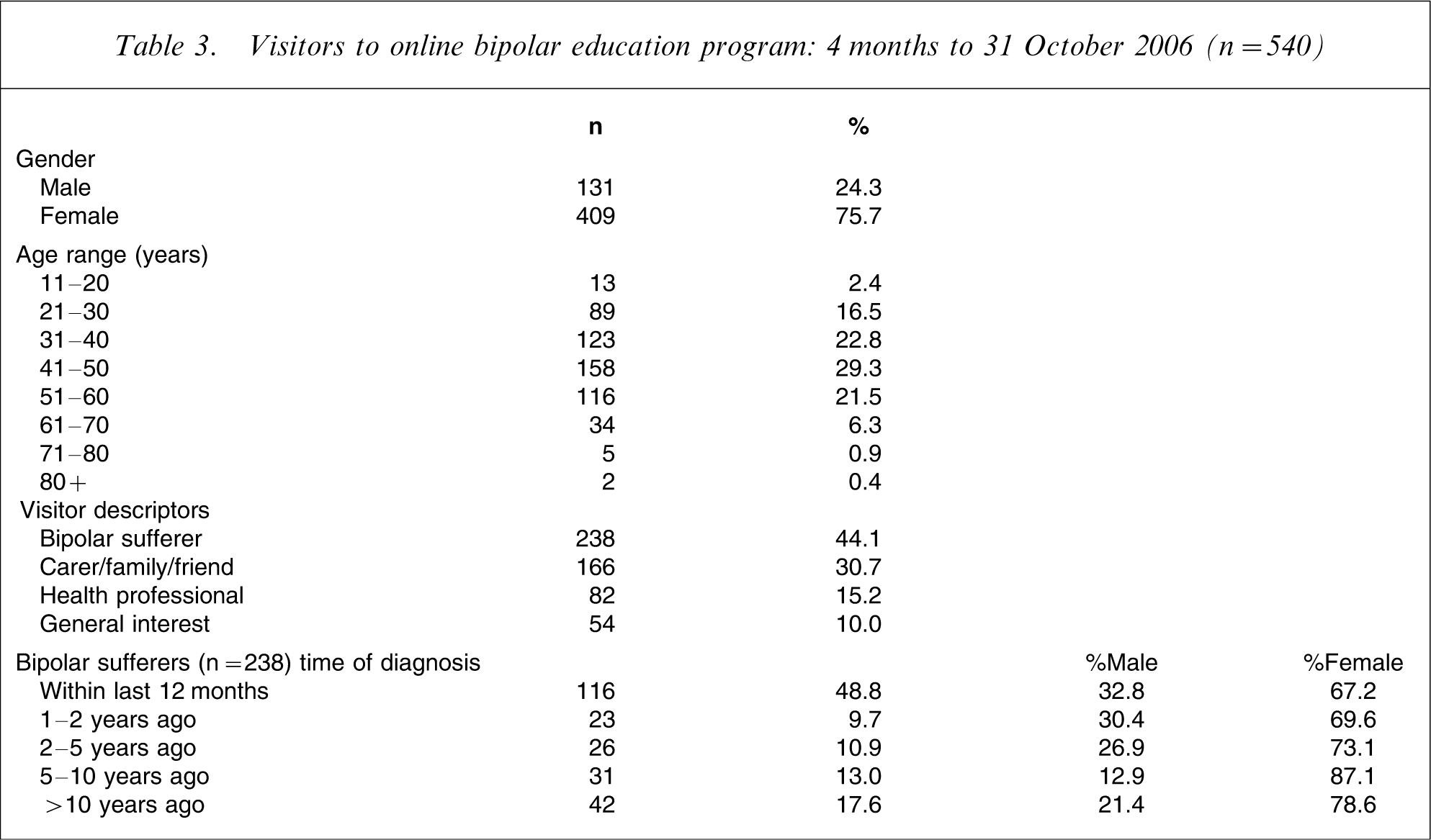
Table 3 shows a breakdown of new visitors to the online program, by gender, age, personal description (person with bipolar disorder, carer/family/friend, health professional, general public). For those with bipolar disorder, we report the length of time since diagnosis. In total, 540 users (approximately five per day) registered as new visitors to the site in 3 months. It should be noted that registration is not a condition of accessing the website, so not all new visitors will have registered. Of those who did, however, 75.7% were female, ages varied from 11 years to >80 years, with the majority (>70%) in the 31–60 range, and 44.1% reported that they had bipolar disorder. Of those with bipolar disorder, 48.8% were diagnosed with the condition within the previous 12 months (ranging to 17.6% diagnosed >10 years ago); 48.8% were aged ≤40 and 72.7% were female.
Visitors to online bipolar education program: 4 months to 31 October 2006 (n = 540)
Discussion
Site usage data indicate that the bipolar education program is attracting a substantial volume of visitors, consisting primarily of people with bipolar disorder, but also health professionals, carers/family/friends of individuals with the condition and the general public. Women are generally more likely to seek health information on the Internet [21], and the preliminary usage data on the bipolar education program support this trend, with 76% of all visitors and 73% of visitors with bipolar disorder being women. Within the group with bipolar disorder (n = 238), approximately 50% were aged ≤40. In Australia, 90% of the burden of bipolar disorder is borne within this age range [3] and people in this age group are also regular users of the Internet. Provision of high-quality evidence-based information and education material via this medium is therefore critical because earlier education will lead to better management.
While the online bipolar education program has not been presented as a package containing a set number of modules, in its free-choice modularized format, session data show that users are generally completing the modules they commence. The data compare very well with other e-mental health applications and are a preliminary indication of the utility of the program. But, because the online application is new, the data reported here are introductory and results are needed from our randomized controlled trial for definite conclusions to be drawn.
The use of online self-management education allows people to proceed at their own pace, dealing with information in a graduated manner and as the need arises, rather than in one or two face-to-face consultations. This paper, highlighting initial take-up and completion rates of the Web-based bipolar education program, offers promise for its wider use. Should the results of our randomized controlled trial demonstrate that the program improves patients’ self-management, illness trajectory and psychosocial outcomes, the widespread accessibility of the program, particularly for people in rural areas, has implications both for individual users and at a public health level.
Footnotes
Acknowledgements
The authors are grateful to the experts who contributed to the bipolar education program: Professor Phil Mitchell, Professor Gin Malhi, Assoc. Professor Meg Smith, Dr Margo Orum, Dr Sarah Russell, Dr Anne-Marie Rees, Ms Fay Jackson, Assoc. Professor Neil Cole, Assoc. Professor Vijaya Manicavasagar. The research study is supported by a National Health and Medical Research Council Program Grant.