Objective: To inform the debate on the relationship between gender and depression by examining clinicians’ ratings on selected HoNos items in two cultural groups.
Method: Scores on items 1 (overactivity/aggression) and 2 (depression) as recorded by clinicians in the CAOS study of more than 12,000 unselected New Zealand psychiatric service users were analysed by gender and self identified ethnicity.
Results: The lowest ratings for depression and highest for overactivity/agression were assigned to Maori males. Female Maori, were rated next, followed by male non-Maori. Female non-Maori were rated highest on depression and lowest on overactivity/agression.
Conclusions: Amongst the hypotheses to explain these findings are those relating to service utilization, rater bias, criteria bias, and cultural pathoplastic effects. These questions need answers.
That female individuals receive diagnoses of depression more often than do male subjects has been noted in both mental health service user characteristics and in community population surveys [1–4]. Gender-based differences such as these have often been accepted as reflecting epidemiological reality. It has also been hypothesized that there may be a gender bias in the selection, wording, or use of the criteria [5].
A number of publications have raised the issue of a racial or ethnic bias in clinicians’ assessment of psychiatric patients [6–12]. These have generally shown higher rates of diagnosis of schizophrenia and/or observations of violence and lower rates of depression in so-called minority groups such as African–Americans [8, 13–16]. Recent New Zealand work has raised the possibility of a race-based bias in the recognition of some common, diagnostically relevant phenomena. Such a bias could lead to an over-diagnosis of mood elevation, particularly when using standard decision trees such as those used with the Composite International Diagnostic Interview [9, 17].
New Zealand is a multicultural country with a legislative commitment to biculturalism that, along with the origins of the country's nationhood, stems from the treaty agreement made between Ma(accepted as the first occupiers) and the European colonizers. While the current population is of mixed ethnicity, people of European descent numerically dominate (68%), followed by New Zealand Maori (15%). The remaining 17% contains people of Asian (8%), Pacific (7%) and other (2%) origins [18]. Given the existence of standardized clinical assessment information on large numbers of service users in New Zealand [19–21], associations between gender, ethnicity and clinical diagnoses can be examined from existing data.
Method
As part of a major research project into casemix definition and outcomes (CAOS), standardized assessments were performed on 12 756 (unselected) mental health service users in New Zealand [19–21]. Assessment of phenomenology was recorded by using the Health of Nations Outcomes Scale (HoNOS) [20–22]. Seven of the 12 scales on the HoNOS (aggression/overactivity; deliberate self-harm; substance misuse; cognitive problems; hallucinations/delusions; depressed mood; other psychological problems) record the clinician's judgements on diagnostically relevant psychiatric phenomena. In the present paper selected data from that study are summarized, displayed and discussed to the extent that it reflects on the relevance of gender and ethnicity to the diagnosis of depression.
Results
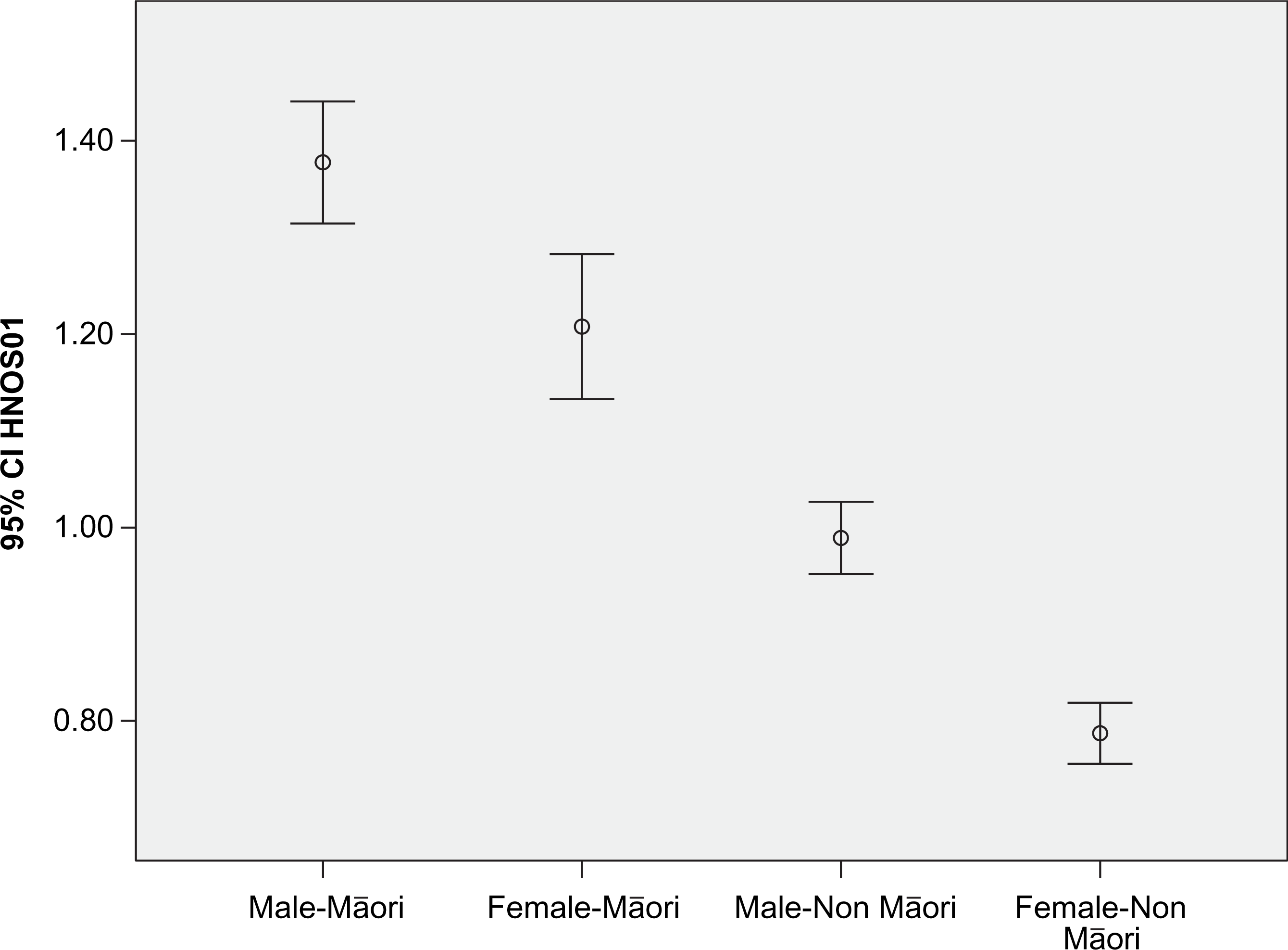
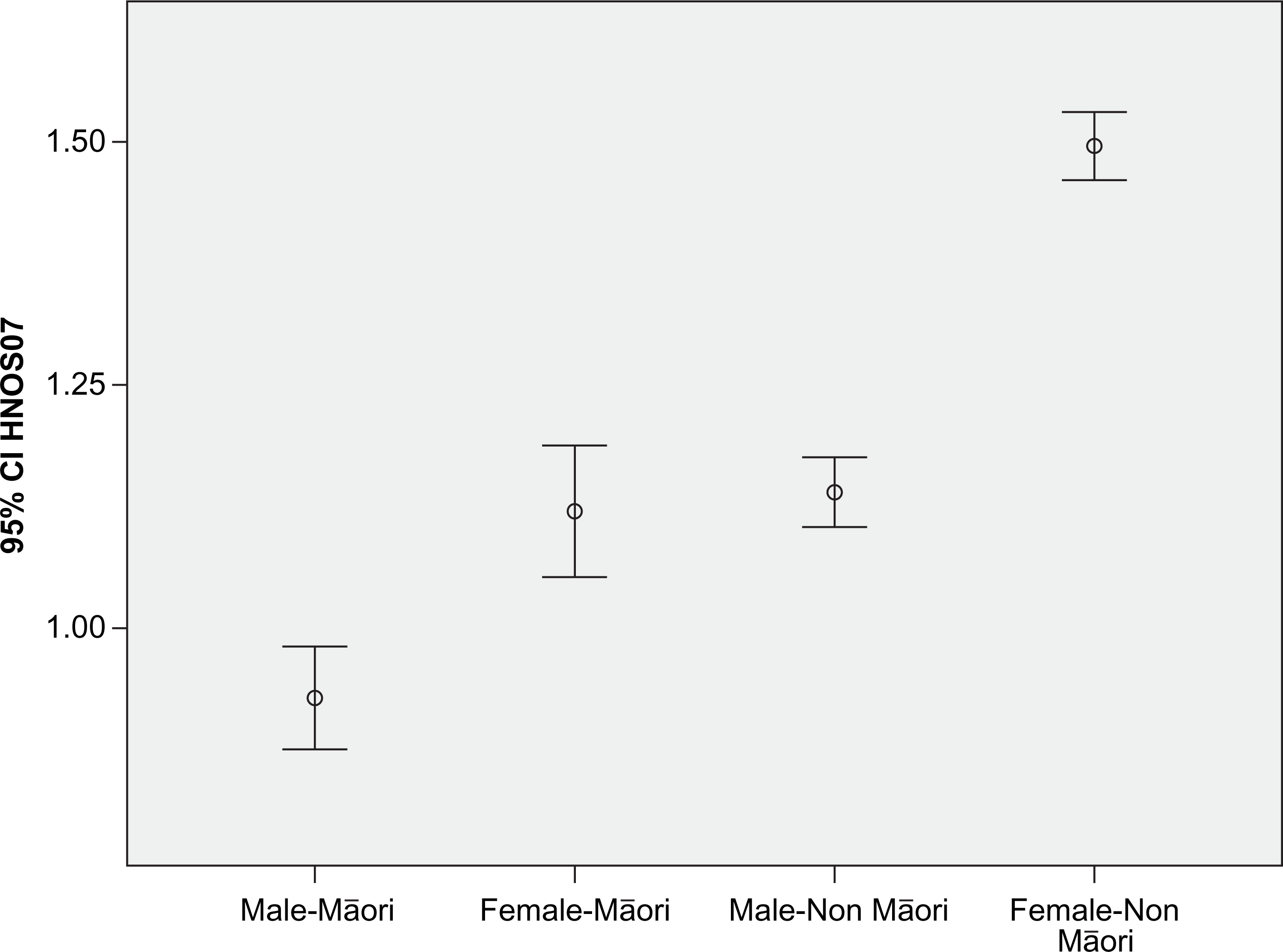
In the CAOS study the male: female ratio for the total dataset was 53:47 with Maori comprising 20% (against 15% across the country as a whole). The HoNOS information for three items, derived from the 12 576 consecutive mental health service users at approximately one-third of the New Zealand mental health services, was extracted. The data by gender and ethnicity are displayed in Figure 1 for HoNOS, item 1 (aggression/overactivity) and in Figure 2 for depression (HoNOS item 7). Pacific Polynesians were excluded from the displayed data because their number was too small to be analytically useful as a separate group, whereas to combine them with Maori would be conceptually unhelpful and culturally inappropriate.
Health of Nations Outcomes Scale (HoNOS) item 1 (aggression/overactivity). CI, confidence interval.
Health of Nations Outcomes Scale (HoNOS) item 7 (depression). CI, confidence interval.
HoNOS item 1, aggression/overactivity
On HoNOS item 1 (rating aggression and over activity) a clear separation between the four gender/ethnicity groups is apparent. For Maori, both sexes score higher than for non-Maori. The separation for depression (Figure 2) shows that female Maori and male non-Maori are similar, with non-Maori female subjects achieving by far the highest depressive rating and Maori male subjects the lowest.
For HoNOS item 2 (self-harm) there were no statistical differences between the four gender/ethnic groups.
HoNOS item 7, depression
The diagnoses made in the CAOS study are consistent with the patterns described here in that depression was much more common in non-Maori (30% of episodes) than Maori subjects (16% of episodes), and in female (27% of episodes) than male subjects (15% of episodes).
Discussion
The evidence discussed here is confined to numerical measures of clinicians’ judgements across ethnicity and gender. The striking directional similarity between Maori/non-Maori ratios and male/female ratios for HoNOS items 1 (aggressive/overactive behaviour) and 7 (depression) requires explanation. Whether or not these gender- and ethnicity-based differences in the rates of labelled depression in mental health service users are the result of real differences in incidence, diagnosis and gender-specific differential rates of service use, or of clinicians’ false perceptions and mislabelling are open questions that await definitive hypothesis-driven, appropriately designed research. The relevance of cross-cultural misperceptions has been highlighted in a US context [14].
A major point of difference between Maori and non-Maori culture may be that, in terms of gender behaviour, the former is more often perceived as displaying behaviour associated with masculinity – the explanations for which involve a range of paradigms and contexts [23–25]. This contention is consistent with ethnicity-based explanations for differential crime rates [26], the public perception regarding male aggression (the ‘Once were warriors’ syndrome), the high rates of perceived aggression [27] and the service use of seclusion and antipsychotic drugs on Maori patients [28, 29]. All of these findings have parallels with studies involving African–Americans [14]. Aspects of Maori kawa (protocols) and the aggressive components of some areas of the Maori performing arts are topics of frequent debate that relate to equally important notions of indicators of mental health in patriarchal societies [25].
There is a need to explore how, in the context of this discussion, this differs from the dimension of the high levels of competitiveness and aggressiveness encouraged across areas of New Zealand society as a whole, with the ‘entertainment value’ of violence in sport and video games being an excellent example. Alternatively, it is entirely possible that Maori are being inappropriately labelled as aggressive, as has happened with other ethnic minorities outside New Zealand despite the objective evidence not supporting the description [14]. Ultimately, explanations will be sought in a mix of sociocultural and individually based concepts.
A high rate of completed suicide in Maori, despite apparently lower levels of depression, is consistent with unrecognized depression [11]. If there is validity to the suggestion that it is in line with male-gendered behaviour not to show one's feelings and/or not to seek help [5, 30] (a behaviour also associated with Maori male individuals [31]), then the male: female ratio on the recognition of depression can be easily accounted for.
Concluding comment
Underrepresentation of treated depression in male and/or Maori subjects could be a consequence built into current diagnostic systems or a linguistic artefact tied to the perceptions of clinicians. This points to the need for future research designed to unravel these issues and to deal with (i) the possibility that differences between Maori and non-Maori and male and female are spurious relationships confounded by some personality and/or socioeconomic variables; and (ii) to further explore the way in which gendered behaviour in non-Maori and in Maori culture could impact on patterns of mental health status.
References
1.
KesslerRCMcGonagleKASwartzMBlazerDGNelsonCB. Sex and depression in the National Comorbidity Survey 1: lifetime prevalence, cronicity and recurrence. J Affect Disord1993; 29: 85–96.
2.
RorsmanBGrasbeckAHagnellO. A prospective study of first-incidence depression. Br J Psychiatry1990; 156: 336–342.
3.
Blair-WestGWCantorCHMellsopGWEyeson-AnnanML. Lifetime suicide risk in major depression: sex and age determinants. J Affect Disord1999; 55: 171–178.
4.
WellsJE, Oakley BrowneMA, ScottKM, McGeeMA, BaxterJ, KokauaJ; New Zealand Mental Health Survey Research Team. Te rau hinengaro: the New Zealand Mental Health Survey: overview of methods and findings. Aust N Z J Psychiatry2006; 40:835–844.
5.
BrownhillSWilhelmKBarclayLSchmiedV. ‘Big build’: hidden depression in men. Aust N Z J Psychiatry2005; 39: 921–931.
6.
WhaleyAL. Cross-cultural perspective on paranoia: a focus on the black American experience. Psychiatry Q1998; 69: 325–343.
7.
DialaCCMuntanerCWalrathCNickersonKLaVeistTLeafP. Racial/ethnic differences in attitudes toward seeking professional mental health services. Am J Public Health2001; 91: 805–807.
8.
HuttonHEMinorMHBladesJRLangfeldtVC. The ethnic differences on the MMPI Overcontrolled–Hostility Scale. J Pers Assess1992; 58: 260–268.
9.
MellsopGDutuGEl-BadriS. CAOS Contribution to understanding cultural/ethnic differences in the prevalence of bipolar affective disorder in New Zealand. Aust N Z J Psychiatry2007; 41: 392–396.
10.
StrakowskiSMSheltonRCKolbrenerNL. The effects of race and comorbidity on clinical diagnosis in patients with psychosis. J Clin Psychiatry1993; 54: 96–102.
11.
TapsellRMellsopGW. The contributions of culture and ethnicity to New Zealand mental health research findings. Int J Soc Psychiatry2007; 53: 317–324.
12.
WangEWDiamondPM. Empirically identifying factors related to violence risk in corrections. Behav Sci Law1999; 17: 377–389.
13.
VelasquezRJCallahanWJYoungR. Hispanic-White MMPI comparisons: does psychiatric diagnosis make a difference?. J Clin Psychol1993; 49: 528–534.
14.
HicksJW. Ethnicity, race and forensic psychiatry: are we color-blind. J Am Acad Psychiatry Law2004; 32: 21–33.
15.
LawsonWBYesavheejAWernerPD. Race, violence and psychopathology. J Clin Psychiatry1984; 45: 294–297.
16.
KalesHCBlowFCBinghamCRCopelandLAMellowAM. Race and inpatient psychiatric diagnoses among elderly veterans. Psychiatr Services2000; 51: 795–800.
17.
KesslerRCUstunB. The World Mental Health (WMH) Survey Initiative Version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). Int J Methods Psychiatr Res2004; 13: 93–121.
18.
TatauKahukara. Public Health Intelligence Monitoring Report No. 5. Wellington, NZ: Ministry of Health, 2006.
19.
EagarKGainesPBurgessP. Developing a New Zealand casemix classification for mental health services. World Psychiatry2004; 3: 172–177.
20.
TrauerTEagarKMellsopG. Ethnicity, deprivation and mental health outcomes. Aust Health Rev2006; 30: 310–321.
21.
TrauerTEagarK. New Zealand mental health consumers and their outcomes. Health Research Council of New Zealand, Auckland2004.
22.
WingJKBeevorASCurtisRHParkSHaddenSBurnsA. Health of Nation Outcome Scales (HoNOS). Br J Psychiatry1998; 172: 11–18.
23.
IhimaeraW. The uncle's story. Penguin, Auckland2000.
24.
HokowhituB. Maori masculinity, post-structuralism, and the emerging self. N Z Sociol2003; 18: 179–201.
25.
PirretJ. Hegemonic masculinity and its effect on Maori men's health. Master of Arts Thesis, University of Waikato, Waikato, New Zealand, 2000.
26.
MellsopGDutuGMcClintockK. Population funding formula cultural coefficients. N Z Med J2007; 115: 91–93.
27.
ParkerG. Beyond major depression. Psychol Med2005; 35: 467–474.
28.
El-BadriSMMellsopGW. Aggressive behaviour in an acute general adult psychiatric unit. Psychiatr Bull2006; 30: 166–168.
29.
HumberstoneVWheelerALambertT. An audit of outpatient antipsychotic usage in the three health sectors of Auckland, New Zealand. Aust N Z J Psychiatry2003; 37: 240–245.
30.
GaldasPMCheaterFMarshallP. Men and health help-seeking behaviour: literature review. J Adv Nurs2005; 49: 616–623.
31.
McCreanerTNairnR. Tauiwi general practitioners talk about Maori health: interpretative repertoires. N Z Med J2002; 115: 272–279.