
Abstract
Objectives:
The purpose of this study was to investigate whether there were gender-specific depressive symptom profiles or gender-specific patterns of psychotropic agent usage in Asian patients with depression.
Method:
Clinical data from the Research on Asian Psychotropic Prescription Patterns for Antidepressant study (1171 depressed patients) were used to determine gender differences by analysis of covariates for continuous variables and by logistic regression analysis for discrete variables. In addition, a binary logistic regression model was fitted to identify independent clinical correlates of the gender-specific pattern on psychotropic drug usage.
Results:
Men were more likely than women to have loss of interest (adjusted odds ratio = 1.379, p = 0.009), fatigue (adjusted odds ratio = 1.298, p = 0.033) and concurrent substance abuse (adjusted odds ratio = 3.793, p = 0.008), but gender differences in other symptom profiles and clinical features were not significant. Men were also more likely than women to be prescribed adjunctive therapy with a second-generation antipsychotic (adjusted odds ratio = 1.320, p = 0.044). However, men were less likely than women to have suicidal thoughts/acts (adjusted odds ratio = 0.724, p = 0.028). Binary logistic regression models revealed that lower age (odds ratio = 0.986, p = 0.027) and current hospitalization (odds ratio = 3.348, p < 0.0001) were independent clinical correlates of use of second-generation antipsychotics as adjunctive therapy for treating depressed Asian men.
Conclusion:
Unique gender-specific symptom profiles and gender-specific patterns of psychotropic drug usage can be identified in Asian patients with depression. Hence, ethnic and cultural influences on the gender preponderance of depression should be considered in the clinical psychiatry of Asian patients.
Introduction
Depression, a worldwide public health issue, is a major contributor to morbidity, disability, mortality and other conditions that arise from mental illness (Bastiampillai et al., 2013; Jacob, 2013; Park et al., 2013, 2014a; Whiteford et al., 2013). Gender plays a significant role in depression rate, symptom profile, treatment response and illness course, as well as other clinical features of depression (Marcus et al., 2005; Schuch et al., 2014). It is a consistent finding that the lifetime prevalence of major depressive disorder is much higher in women than in men (Regier et al., 1993; Kessler et al., 1994). Previous substantial studies have revealed that depressed women are more likely than depressed men to have atypical symptoms, such as increased appetite, weight gain, anxiety, interpersonal sensitivity and somatic complaints (Lamers et al., 2010; Marcus et al., 2005; Silverstein, 2002). Furthermore, although controversial, it has been proposed that there is a significant correlation between gender and probability of responding to antidepressant treatment (Yang et al., 2011).
Ethnic and/or cultural factors as well as biological and psychosocial factors can shape depressive symptoms and treatment responses (Bromberger et al., 2004; Kanazawa et al., 2007; Leach et al., 2008). The Research on Asian Psychotropic Prescription Patterns for Antidepressants (REAP-AD) study is part of the Research on East Asia Prescription Patterns of Psychotropic Drugs (REAP) study (Xiang et al., 2012). REAP-AD has collected clinical and treatment data for patients in Asia who were prescribed antidepressants. The aim of REAP-AD was to identify the clinical factors that influenced antidepressant prescription patterns. It is one of the largest international surveys of the prescription of antidepressants in Asian countries and regions. Therefore, its findings can reveal overall trends in clinical manifestations and patterns of psychotropic drug usage (Shinfuku, 2014).
Gender disparities in depressive symptoms and related features have been well studied in the Unites States and Europe (Kessler et al., 1994; Kuehner, 2003; Marcus et al., 2005; Regier et al., 1993; Schuch et al., 2014). However, such studies are rare in Pan-Asian countries. Therefore, the objective of this study was to investigate whether there were gender-specific depressive symptom profiles or gender-specific patterns of psychotropic agent usage among Asian patients with depression using data from the REAP-AD study.
Methods
Study overview
During the study period from March to June 2013, a total of 2320 psychiatric patients who were prescribed antidepressants in the Department of Psychiatry were recruited into the REAP-AD study. Hence, inpatients prescribed antidepressants in Departments of Medicine and Surgery in general hospitals were excluded from the REAP-AD study. A total of 2320 psychiatric patients were recruited from China (n = 350), Hong Kong (n = 81), India (n = 309), Indonesia (n = 269), Japan (n = 246), Korea (n = 259), Malaysia (n = 311), Singapore (n = 135), Taiwan (n = 199) and Thailand (n = 311). Protocols and consent forms were approved by the individual Institutional Review Boards (IRBs) of the survey centers, comprising four in China, one in Hong Kong, five in India, three in Indonesia, five in Japan, four in Korea, six in Malaysia, two in Singapore, four in Taiwan and five in Thailand. To guarantee consistent data collection and entry, consensus conferences were held before the survey. The data collection center was situated in the Taipei City Psychiatric Center, Taipei, Republic of China.
Study subjects
To reflect the true clinical situation and for convenience of sampling, the inclusion criteria used for the REAP-AD study for psychiatric patients using antidepressant medication during the survey period were used in this study. Since not only patients with depressive disorders but also those with other disorders can use antidepressants, the subjects of the REAP-AD study were used in this study regardless of their psychiatric diagnosis (Shinfuku, 2014). All study subjects gave informed consent prior to participation. Diagnoses were made by clinical psychiatrists in the 39 survey centers in accordance with either the International Classification of Disease, tenth revision (ICD-10; World Health Organization, 1992) or the Diagnostic and Statistical Manual of Mental Disorder, fourth edition (DSM-IV; American Psychiatric Association, 1994). Demographic and clinical characteristics (depressive symptom profiles, clinical variables and patterns of psychotropic drug usage) of the patients were collected by clinical psychiatrists at the survey centers.
In our study, we used only those patients with a diagnosis of depressive episode (F33) or recurrent depressive disorder (F34). Patients under the age of 18 years were excluded. As shown in Table 1, a total of 1171 individuals from the REAP-AD study were used in our study.The minimum number of recruits in each of the 10 Asian countries and regions was 38 and the maximum number was 400.
Gender differences in baseline variables.
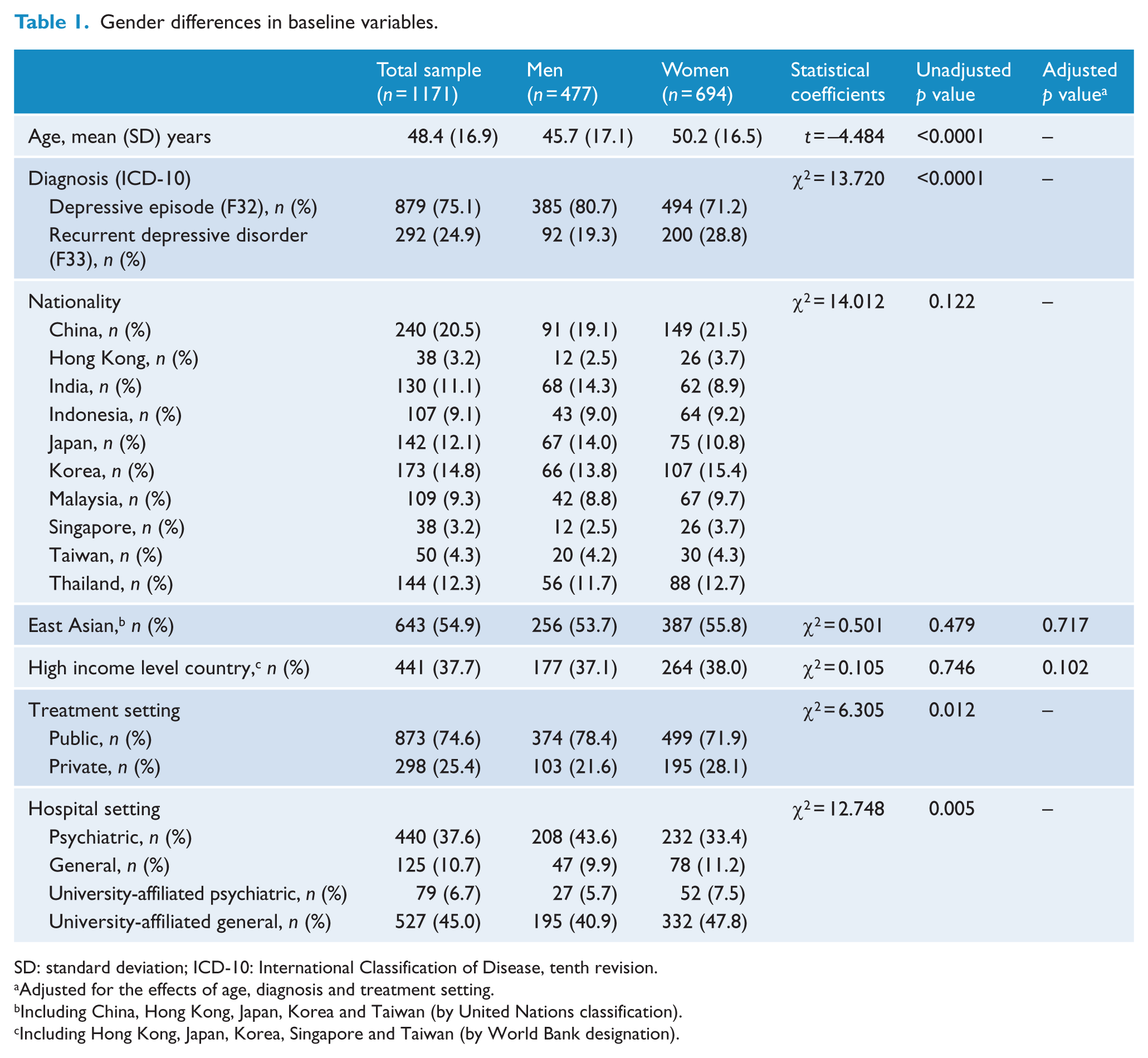
SD: standard deviation; ICD-10: International Classification of Disease, tenth revision.
Adjusted for the effects of age, diagnosis and treatment setting.
Including China, Hong Kong, Japan, Korea and Taiwan (by United Nations classification).
Including Hong Kong, Japan, Korea, Singapore and Taiwan (by World Bank designation).
Baseline variables
In our study, 10 Asian countries and regions were grouped according to their geographical contiguity and income level. Using the United Nations classification, the 10 countries and regions were classified into the following three groups: East Asia (China, Hong Kong, Japan, Korea and Taiwan), South Asia (India) and South-East Asia (Indonesia, Malaysia, Singapore and Thailand). For statistical analysis, these three groups were then dichotomized into East Asia, and South and South-East Asia. Using the World Bank income designation, the countries and regions were also grouped into high income (Hong Kong, Japan, Korea, Singapore and Taiwan), upper middle income (China, Malaysia and Thailand) and lower middle income (India and Indonesia) countries. These groups were also split into high and middle (upper and lower) income countries.
Depression symptom profiles and clinical variables
The following 10 depressive symptom profiles listed in the National Institute for Health and Care Excellence (NICE) guidelines (National Institute for Health and Clinical Excellence, 2009) were used to establish the presence or absence of depressive symptoms: persistent sadness, loss of interest, fatigue, insomnia, poor concentration, low self-confidence, poor appetite, suicidal thoughts/acts, agitation/retardation and guilt/self-blame. Each depression symptom profile was evaluated by clinical psychiatrists in the survey centers. The degree of depression was defined by the total number of depressive symptoms, and four categories of depression were used: subthreshold (<4 symptoms), mild (= 4 symptoms), moderate (5–6 symptoms) and severe (>6 symptoms). Comorbid psychiatric disorders were determined based on ICD-10 (i.e. mental and behavioral disorders due to psychoactive substance abuse [F1] and neurotic, stress-related and somatoform disorders [F4]). In addition, medical comorbidities were defined by the presence of the following physical illnesses: myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, chronic pulmonary disease, rheumatic disease, peptic ulcer disease, mild liver disease, diabetes mellitus, hemiplegia/paraplegia, renal disease, malignancy, moderate to severe liver disease, metastatic solid tumor, AIDS/HIV and other medical illnesses.
Patterns of psychotropic drug use
In this study, we considered as new antidepressants selective serotonin reuptake inhibitors (SRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), norepinephrine and dopamine reuptake inhibitors (NDRIs), mixed noradrenergic-serotonergic antidepressants, selective norepinephrine reuptake inhibitors (NRIs), serotonin receptor antagonists and weak monoamine transport effectors. Tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs, both irreversible and reversible) were considered older antidepressants (Sim et al., 2014). Combination treatment was defined as treatment with two or more antidepressants. Augmentation therapy was defined as concurrent treatment with an antidepressant and some other psychotropic drug (Won et al., 2014). The classification into first- and second-generation antipsychotics was based on the introduction of clozapine (Park et al., 2014b).
Statistical analysis
Independent t-tests for continuous variables and χ2 tests for discrete variables were used to compare sociodemographic characteristics, depressive symptom profiles, comorbid psychiatric and medical diseases, and use of psychotropic medications in male and female subjects. Analysis of covariance (ANCOVA) for continuous variables and logistic regression analysis for discrete variables were used to control for the influence of confounding variables. A binary logistic regression model was fitted to identify independent clinical correlates of gender-specific usage of psychotropic agents. Standard methods such as goodness of fit were used to select and validate the final model. The logistic regression was based on the forward selection method to avoid multicollinearity. Statistical significance was set at p < 0.05 (two-tailed) for all tests. All statistical analyses were performed using SPSS 18.0 software for Windows (SPSS Inc., Chicago, IL, USA).
Results
Baseline variables
As shown in Table 1, approximately 60% of the 1171 individuals selected for this study were women. The mean age of the subjects was 48.4 (standard deviation [SD] = 16.9) years. Most subjects (75.1%) were diagnosed with a depressive episode, with more than half (61.7%) from East Asia. The representation from China (20.5%) was greater than from any other country. On average, the men (45.7 years, SD = 17.1) were younger than the women (50.2 years, SD = 16.5; t = –4.484, p < 0.0001). In addition, the proportion of depressive episodes (F33) in men was higher than in women (χ2 = 13.720, p < 0.0001). In terms of treatment setting, the proportion of men in public hospitals was higher than that of women (χ2 = 6.305, p = 0.012). Moreover, more men were in a psychiatric hospital setting, whereas more women were in a university-affiliated general hospital setting (χ2 = 12.748, p = 0.005). To mitigate the influence of confounding variables, gender differences in baseline variables, depressive symptom profiles and usage of psychotropic drugs were evaluated by adjusting for the effects of age, diagnosis and treatment setting. In terms of nationality, no significant difference between male and female patients was found according to geography (adjusted odds ratio [aOR] = 1.048, p = 0.717) or economical status (aOR = 0.792, p = 0.102).
Depressive symptom profiles and clinical variables
As shown in Table 2, men differed from women in the following characteristic depressive symptoms: they had more loss of interest (aOR = 1.379, p = 0.009) and fatigue (aOR = 1.298, p = 0.033), but less frequent suicidal thoughts/acts (aOR = 0.724, p = 0.028). No significant difference was found between men and women in the following symptoms: reporting of persistent sadness (aOR = 0.886, p = 0.378), insomnia (aOR = 0.932, p = 0.582), poor concentration (aOR = 1.030, p = 0.825), low self-confidence (aOR = 1.103, p = 0.498), poor appetite (aOR = 0.791, p = 0.073), agitation/retardation (aOR = 0.962, p = 0.794) and guilt/blame (aOR = 0.849, p = 0.329). In terms of the degree of depression, using subthreshold depression as a reference category, there were no significant gender differences in the frequency of mild depression (aOR = 1.372, p = 0.060), moderate depression (aOR = 1.039, p = 0.802) or severe depression (aOR = 0.876, p = 0.522). A higher proportion of men had comorbidities of behavioral disorders due to psychoactive substance abuse (aOR = 3.793, p = 0.008). In addition, a higher proportion of men had inpatient treatment (aOR = 1.433, p = 0.009). However, there were no significant differences in the comorbid incidence of neurotic, stress-related and somatoform disorders (aOR = 0.832, p = 0.439) or physical illnesses (aOR = 0.921, p = 0.579).
Gender differences in depressive symptom profiles and clinical variables.
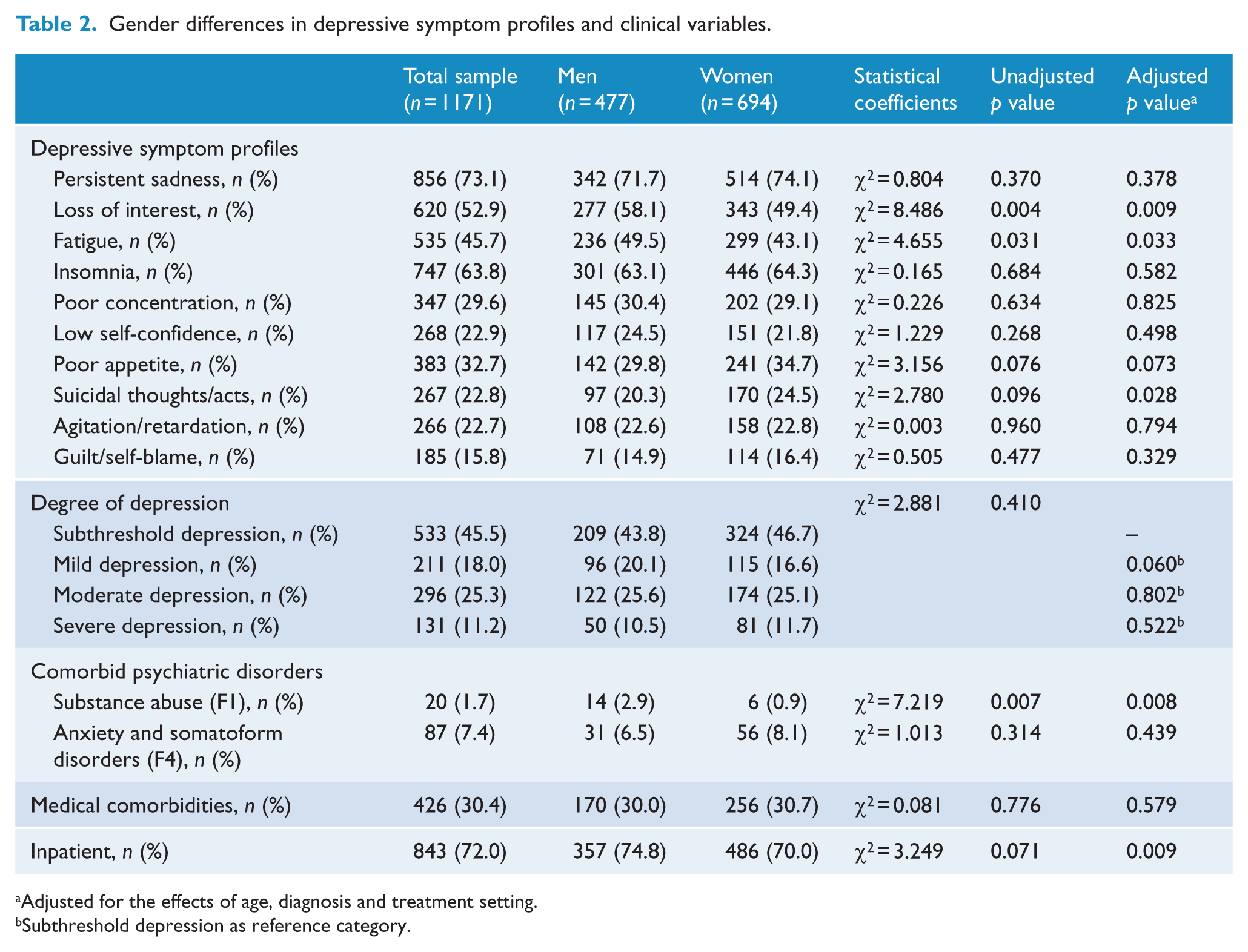
Adjusted for the effects of age, diagnosis and treatment setting.
Subthreshold depression as reference category.
Patterns of psychotropic drug usage
As shown in Table 3, a higher proportion of men used second-generation antipsychotics (aOR = 1.320, p = 0.044) when psychotropic drugs were used as adjunctive therapy. However, there was no significant gender difference in the prescription of newer antidepressants (aOR = 1.020, p = 0.892), combination treatment (aOR = 0.822, p = 0.171), augmentation treatment (aOR = 0.942, p = 0.640), anxiolytics (aOR = 0.972, p = 0.833), hypnotics (aOR = 1.367, p = 0.084), mood stabilizers (aOR = 0.913, p = 0.551), first-generation antipsychotics (aOR = 0.919, p = 0.688) or antiparkinson agents (aOR = 0.912, p = 0.731).
Gender differences in patterns of use of psychotropic drugs.
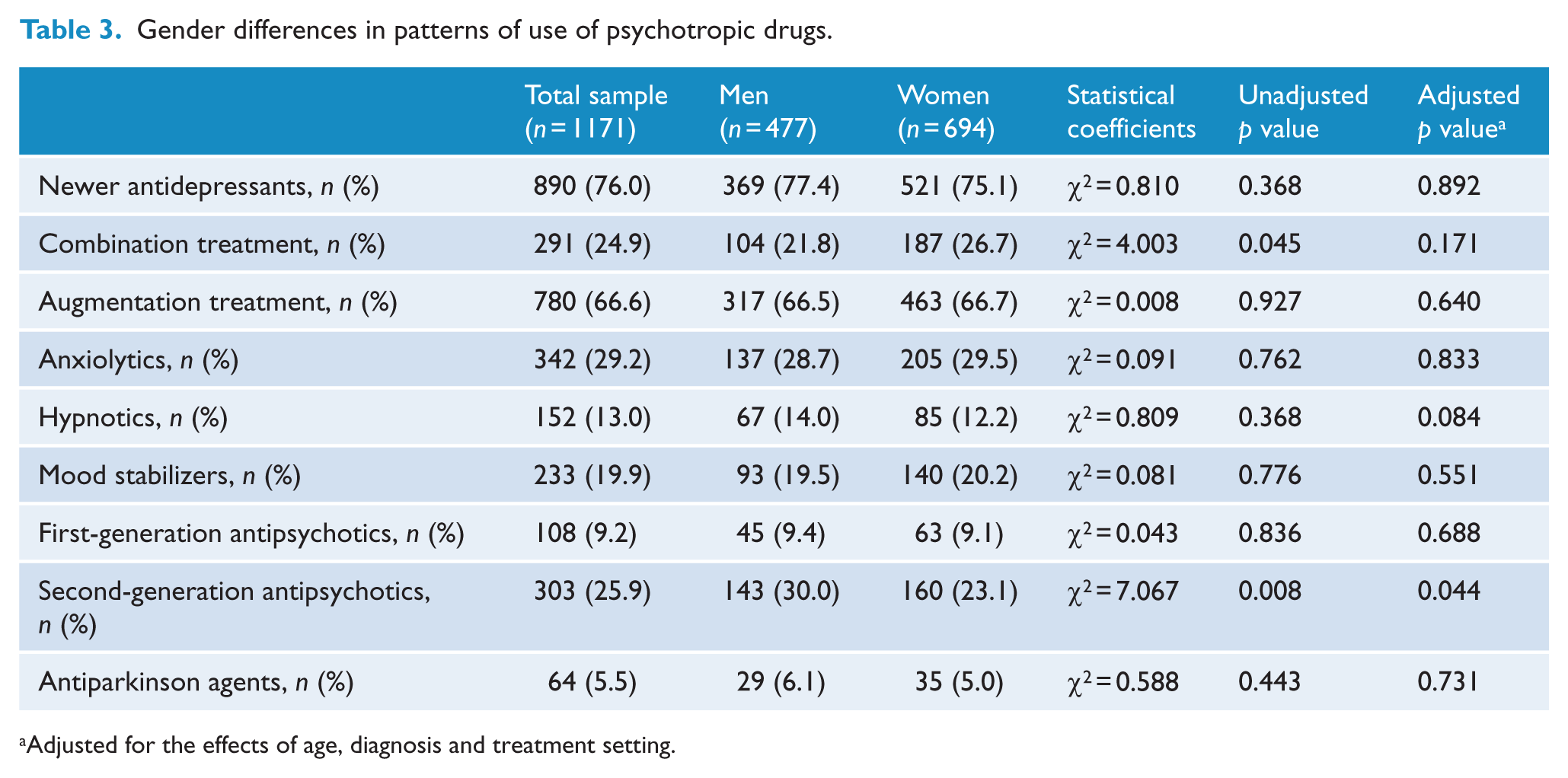
Adjusted for the effects of age, diagnosis and treatment setting.
Independent clinical correlates of supplementation with second-generation antipsychotics in men with depression
A binary logistic regression model was fitted for depressed men. In the model, the category of depressed men treated with additional second-generation antipsychotics was defined as the dependent variable and the category of depressed men not treated with second-generation antipsychotics served as the reference category. Age, diagnosis (depressive episode or recurrent depressive disorder), loss of interest, fatigue, suicidal thoughts/acts, concurrent mental and behavioral disorders due to psychoactive substance abuse and inpatient treatment were covariates. As shown in Table 4, Hosmer–Lemeshow goodness-of-fit test (χ2 = 9.569, df = 8 and p = 0.297) confirmed that the fitted logistic model was acceptable. The final model accounted for 10.4% (Nagelkerke R2) of the variability. It showed that lower age (odds ratio [OR] = 0.986, p = 0.027) and current hospitalization (OR = 3.348, p < 0.0001) were independent clinical correlates of the prescription of second-generation antipsychotics in depressed men.
Independent clinical correlates of adjunct therapy with second-generation antipsychotics in depressed male patients (n = 477) in a binary logistic regression model.
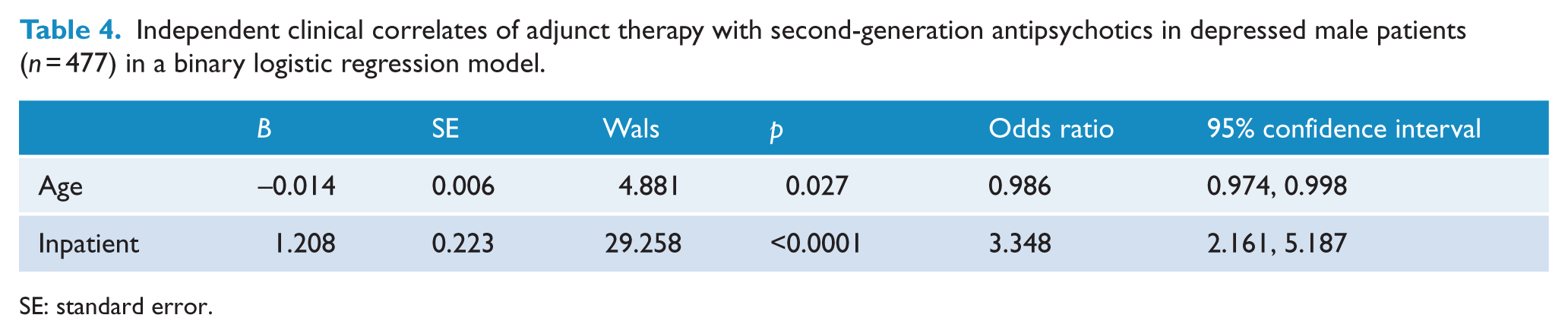
SE: standard error.
Discussion
Depressive symptom profiling in this study revealed that significantly more men than women suffered from loss of interest and fatigue. However, men were less likely to have suicidal thoughts/acts. More men than women reported concurrent substance abuse and current hospitalization, and more were prescribed adjunctive second-generation antipsychotics. Finally, younger age and current hospitalization were identified as independent clinical correlates of the prescription of adjunctive second-generation antipsychotics for depressed men.
The finding that depressed men tend to report more motivational symptoms (loss of interest and fatigue) is partially consistent with findings from the São Paulo Megacity Mental Health Survey (Alexandrino-Silva et al., 2013), which reported that depressed men had decreased energy and other symptoms related to reduced psychomotor activity. Based on the findings of the Genome-based Therapeutic Drugs for Depression (GENDEP) study, loss of interest and decreased activity have been correlated with unsuccessful treatment response to escitalopram and nortriptyline in adults with moderate or severe depression (Uher et al., 2012). The male preponderance of motivation-type depressive symptoms revealed by our study suggests that there is a greater illness burden in male depressives.
Our study revealed that men were less likely than women to have suicidal thoughts/acts. This is inconsistent with previous findings from the sequenced treatment alternatives to relieve depression (STAR*D) study (Marcus et al., 2008), which reported that male patients with depression reported more suicidal ideation. Although higher suicide rates have been reported in men in Western cultures (Canetto and Sakinofsky, 1998), the reverse pattern has been reported in East Asian contexts. For example, higher suicide rates were found in women in a rural region of China (Yip, 2008). Given the substantial proportion of Eastern Asians among our study subjects, the influence of Buddhist and Confucian cultures on gender roles may have affected gender differences in terms of suicidal ideation (Han et al., 2013). In addition, the higher frequency of atypical, anxiety and somatic symptoms which were previously used to characterize depressive symptom profiles for women (Marcus et al., 2005, 2008; Schuch et al., 2014) was not found in our study. These discrepancies might be due to limitations of our data since they were collected from patients in psychiatric facilities participating in the REAP-AD study and might not be representative of the generality of patients in these countries and regions. Recently, it was reported that Korean outpatients with major depressive disorder suffered more often from hypochondriasis than their American counterparts but less often from depressed mood (Jeon et al., 2014). Therefore, the reversed patterns of typical and atypical symptoms in depressed Asian patients may have contributed to the lower frequency of atypical symptoms in women in our study. However, we cannot exclude the possibility that the overall gender differences in depressive symptoms may be artifactual (Parker and Brotchie, 2010). For example, the higher levels of symptom disclosure and help-seeking behavior in women may inflate diagnoses of depression. Hence, although it has been suggested that male depressive syndrome is a specific clinical disorder characterized by higher frequencies of hyperthymic temperament and soft bipolarity (Azorin et al., 2014), it is not clear whether this distinctive entity actually exists.
Although the higher rate of current hospitalization in men might denote a greater illness burden, there was no significant gender difference in overall severity of depression. Our findings were consistent with previous reports that symptom severity, global severity and functional impairment did not differ between men and women (Frank et al., 1988; Young et al., 1990). We encountered an elevated frequency of concurrent mental disorders and behavioral disorders in male patients due to psychoactive substance abuse (F1), in agreement with the previous finding that the males among the 1115 subjects in the Netherlands Study of Depression and Anxiety (NESDA) reported higher comorbidity of alcohol use or dependence than women (Schuch et al., 2014). Gender was also considered to be a contributing factor to the inverted U-shaped relationship between depressive severity and alcohol abuse (Roger et al., 2000). However, it has been proposed that the higher prevalence of comorbid alcohol/substance abuse in men may mask depressive symptoms (Maier et al., 1999; Piccinelli and Wilkinson, 2000). Hence, one might speculate that gender is not a determining factor for comorbid alcohol use disorder but rather a factor masking depressive symptoms in patients with depressive disorders.
In addition, concurrent rates of neurotic, stress-related and somatoform disorders (F4) did not differ between depressed men and women in our study. On the other hand, Schuch et al. (2014) found that women reported greater comorbidity of panic disorder with agoraphobia and lifetime overall anxiety disorder than men in the data of the NESDA. In addition, female gender was suggested as a determinant of comorbid anxiety disorders in 350 patients with late-life depression (age >60 years) (Van der Veen et al., 2014). These discrepancies could be caused by differences in inclusion criteria (including age), variable moderating effects of cultural influences and other factors. Hence, we cannot conclude unambiguously that there are gender differences in comorbid anxiety disorders, and further study of this issue is needed.
We found that more men than women received adjunctive treatment with second-generation antipsychotics. However, there was no significant difference between men and women in prescription of the newer antidepressants, antidepressant combinations or additional agents. Second-generation antipsychotics have been recommended as increasing treatment responses when first-line treatment according to clinical guidelines fails to work (National Institute for Health and Clinical Excellence, 2009; Won et al., 2014). The more frequent use of second-generation antipsychotics by men may have resulted from a higher rate of failure of first-line treatment, a higher rate of comorbidity or a greater illness burden in men. Our binary logistic modeling showed that lower age and current hospitalization were independent clinical correlates of supplementation with second-generation antipsychotics in depressed men. Higher rates of active suicidal ideation, irritability and anhedonia, and persistence of depressive symptoms in younger adults than in older adults have been previously reported (Wilkowska-Chmielewska et al., 2013). The close relationship between age, current inpatient care and use of second-generation antipsychotics in depressed men may imply that there is a greater burden of depression in men than in women. It may also indicate a cause–effect relationship between gender differences in depressive symptoms and the use of psychotropic agents in Asian patients. On-going studies of these topics have suggested that there may be a subtype of depression involving gender-specific clinical features (Alexandrino-Silva et al., 2013; Oquendo et al., 2013).
There are several limitations to our study. First, the menopausal status of women patients was not evaluated. Age–sex patterns of affective disorders including depression and anxiety have only been identified in premenopausal women (Faravelli et al., 2013). Second, we did not adjust for gender biases in psychometric assessment, and these may have contributed to the gender disparity in depressive symptoms, as reported in previous studies (Cole et al., 2000; Leach et al., 2008; Salokangas et al., 2002). Third, we did not use a modification to Bonferroni’s procedure for testing multiple hypotheses. Fourth, inter-rater reliability was not examined. Fifth, since many of the subjects in our study were East Asian, our findings cannot be generalized to the entire Asian context. Sixth, we did not provide any training to standardize data collection, so the quality of the collected data was not well-controlled. Finally, as data from the REAP-AD study are not epidemiological, there is a potential for sampling bias. Patterns of psychotropic drug usage can depend on the type of psychiatric institution even in the same country or region. Despite these limitations, our study for the first time indicates overall trends in gender differences in the clinical features of Pan-Asian patients with depression. It provides baseline information which can be used for other on-going studies in Asian countries and regions and in other cultural/ethic contexts.
Conclusion
There are unique gender-specific depressive symptom profiles in the Asian contexts. Most notably, there are higher rates of loss of interest and fatigue among Asian male depressed patients than among their female counterparts but a lower rate of suicidal thoughts/acts. The gender difference noted in the use of psychotropic drugs may be associated with, or a secondary consequence of, gender differences in depressive symptoms and related clinical features. Our findings suggest that the pathoplastic effects of culture and race on the clinical presentation of depressive disorders can be seen in gender differences in the clinical features of depression in the Asian context. However globalization, urbanization and industrialization have the potential to mask geographical influences on the culture/ethnic-specific clinical features of mental disorders (Bhugra et al., 2007).
Footnotes
Acknowledgements
The authors are grateful to the following clinicians for their contribution to the REAP-AD study: China: Si Tian Mei, He Yang Lin, Hao Wei, Li Tao; Hong Kong: Helen Chiu, Xiang Yu Tao, Gabor S Ungvari; Japan: Shigenobu Kanba, Hironori Kuga, Naoki Uchida, Kanako Sejima, Senta Fujii, Akira Monji, Jun Nakamura, Shinji Shimodera; Korea: Jong Il Lee, Sang Woo Hahn; Singapore: Eee Heok Kua, Chay Hoon Tan, Kang Sim, Jia Yin Teng, Sandeep Naik, Vincent Lu, Rathi Mahendran; Taiwan: Mian-Yoon Chong, Yi-Hsin Yang, Shih-Ku Lin, Kuan-Pin Su, Tsung-Ming Hu, Shu-Yu Yang; India: Adarsh Tripathi, Ajit Awasthi, Sandeep Grover, Dipesh Bhagabati, Roy A Kallivayalil, Nilesh Shah; Malaysia: Chee Kok Yoon; Thailand: Pichet Udormatn; Indonesia: Andi J Tanra, Isa Multazam, Agung Frijanto, Mara M Maramis, Elmeyda Effendy, Hervita Diatri, Shelly Iskandar, Carla Marchira, Yuniar Sunarko, Tini Sri P.
Declaration of interest
The authors report no conflicts of interest. The authors are solely responsible for the contents and writing of the paper.
Funding
The authors report no funding source.