
Abstract
Mental illness is common and will affect one person in every four at some stage in their lifetime [1]. The Global Burden of Disease study found that mental disorders are the fourth leading cause of global burden and the leading cause of disability [2]. Subsequent studies in developed countries have confirmed that mental disorders are the leading cause of disability [3, 4]. Estimates of the largest causes of disability in the world for the year 2000 placed six mental disorders in the top 20 and included schizophrenia, bipolar affective disorder and depression [1]. These mental disorders may have a significantly negative impact on the quality of life of individuals and their families. This impact results from a combination of the distressing symptoms of the disorder, medication side-effects, stigma and disruption in the individual's ability to participate in a healthy role in society – typically occupational and leisure activities, and meaningful relationships with family, friends and partner [5, 6].
From the 1970s onwards mental health service delivery in New Zealand moved from large stand-alone psychiatric hospitals to services that were located within the community and general hospital setting, a change reinforced by a National Mental Health Strategy in 1994 [7]. One of the two key goals was to ‘increase the health status of and reduce the impact of mental disorders on consumers, their families and the general community’ [7]. The intention of the strategy was to ensure that mental health services were adequately resourced to meet the needs of New Zealand adults with a severe mental disorder at any time [7]. The focus is a recovery approach to service delivery: to not only treat illness but fulfil basic needs (such as employment, income and housing) so that individuals can engage in meaningful roles in society [8].
Public secondary care mental health services in New Zealand are provided free to patients at the point of care, while primary care services are only partially subsidized, and the two systems function predominantly independently of each other. The private health-care sector is relatively small in New Zealand and, although some 40% of New Zealanders have private health insurance, there is minimal provision for mental illness from the private insurers. This means that private mental health care is an even smaller service [9]. In practice, this means that most people with severe mental illness are primarily treated long term in publicly funded secondary care mental health services and those with moderate and mild disorders access primary health services.
Schizophrenia is a severe disorder that is associated with high levels of disability and premature mortality, and for two-thirds of people it follows a chronic course over their lifetime [1, 10]. Over the last decade, treatment approaches (including a combination of new generation (atypical) antipsychotics, psychological and psychosocial interventions) have been recommended by clinical practice guidelines in an attempt to reduce the impairment and improve the quality of life for people with schizophrenia [10, 11].
The clinical symptoms of affective disorders are reported to not be as chronically disabling over time compared to schizophrenia, and higher levels of disability have been found for schizophrenia compared with the higher prevalence affective disorders [12, 13]. Most research contrasting schizophrenia with other disorders is population based and it is difficult to determine if the severity of illness across disorders at the time of contrast was similar. However, the study sample chosen for this review was expected to include some of the most severely mentally unwell outpatients in New Zealand, requiring specialty mental health service intervention. In 2004 the National Mental Health Strategy had been in place for 10 years, clinical practice guidelines had been produced by educational/professional bodies both internationally and locally, specific funding had been made available to ensure access to atypical antipsychotics since 1999, and medication audits over the last 3 years had shown a change in antipsychotic prescribing towards recommended practice for the treatment of schizophrenia [14]. Therefore, the question was whether people with schizophrenia would have significantly more impairment than those with a severe affective disorder receiving treatment in a similar environment.
The aims of the present study were (i) to review the demographic, social and functional characteristics and service utilization of outpatients with schizophrenia attending community mental health centres (CMHC) in four public health services in New Zealand; (ii) to compare this to outpatients with affective disorders (bipolar disorder and depression) attending the same CMHCs and to the general population; and (iii) to determine the conformity with guideline-based treatment of schizophrenia.
Methods
Study sample
This study was a retrospective, cross-sectional file review of all adult outpatients (n = 6164) attending three urban community mental health services in Auckland and a rural service in Northland in October 2004 (2001 catchment population 15–64 years, 872 718 people [15–18]). The cohort was identified as all ‘active outpatients’ (must have been an outpatient in October 2004) from the electronic patient information management system operated in each of the health services for the time of the review (31 October 2004). Only those outpatients with a DSM-IV diagnosis of schizophrenia, including schizoaffective disorder (schizoaffective disorder was included because both are severe long-term disorders and antipsychotic medications are prescribed to treat similar symptoms in both), bipolar disorder (including depressed, manic, hypomanic, mixed or unspecified) or major depression were included in this analysis (n = 5032).
Data collection
Study data were extracted from the paper/electronic clinical file that was used at each mental health service and the patient information management system by a senior psychiatric nurse (trained by the author) who had conducted a similar review 18 months earlier. The data were entered into an Access database with predetermined response options in order to ensure data quality and facilitate analysis. Data collection was piloted with 50 clinical files to ensure that the data variables were consistently recorded in the file, amendments were made and a protocol for collection was written. Data collected included demographics (gender, age, and ethnicity), social and functional information (relationship status, occupational activity, living arrangements and education), primary diagnosis, comorbid conditions and duration of mental illness (defined as time from first contact with a treatment provider), compulsory treatment and inpatient admission history. Primary diagnosis was recorded as the ‘major working diagnosis’ documented at the psychiatric assessment closest to the study review point (most patients are scheduled for 3 monthly appointments to coincide with prescription requirements). If there were inconsistencies between a documented long-standing diagnosis and ‘working diagnosis’ then attempts were made to clarify this with the clinician concerned. Axis I and II comorbidities were recorded if documented at the psychiatric assessment closest to the study review point. Physical health comorbidities were recorded if they were documented and also from medications prescribed con-currently (the Access database allowed for two additional Axis I, two Axis II and up to eight Axis III comorbid conditions to be recorded). Other information was extracted from clinical summaries, case reviews, discharge summaries and the multi-disciplinary progress notes recorded for the three months on either side of the review point. Wherever possible social and functional characteristics were recorded as standardized in the 2001 census questionnaire; but occupational activity could not because it was not documented in this manner. Rather, occupational activity recording was limited to the clinical file data and included full-time employment, part-time occupational activity (including part-time employment, sheltered employment, or volunteer activity), student, homemaker, retired and no occupational activity.
For the schizophrenia group, antipsychotic prescription data were also collected (type, administration route and dose). This information was recorded from the medication chart and verified in the body of the clinical notes or with duplicate copies of the prescription wherever possible, as the treatment the prescriber intended the outpatient to be taking on 31 October 2004. For the purposes of comparison, antipsychotic doses were converted into chlorpromazine equivalents (CPZe) and this is described elsewhere [19]. The study received approval from the Auckland Regional Ethics Committee (AKL2000/065).
Data analysis
Statistical analyses were conducted using SPSS (version 14; SPSS, Chicago, IL, USA). Statistical differences between groups were investigated using χ2 tests for categorical values and one-way analysis of variance for continuous variables. Post-hoc comparisons were conducted using Dunnett's T3 test. When sample distributions did not satisfy assumptions of normality (duration of mental illness) non-parametric tests were used (Kruskal–Wallis). Multiple logistic regression for three binary outcome variables of interest (living independently; having regular occupational activity; and being in a relationship with a partner) was undertaken to investigate the influence of potential confounding variables (gender, age, ethnicity, diagnosis, comorbidity, duration of illness and health service) on primary diagnosis. The probability level required to demonstrate significance was set at 0.01.
Results
Demography
The number of outpatients making up the schizophrenia group was 2883/6164; 46.8% of the active outpatient population. This group had a mean age of 39.1 years, two-thirds were male, half identified as European and they had been unwell for an average of 14 years. Comparison with outpatients with an affective disorder is shown in Table 1. There were more women in the bipolar and depression groups, and more M
Population description (n = 5032)
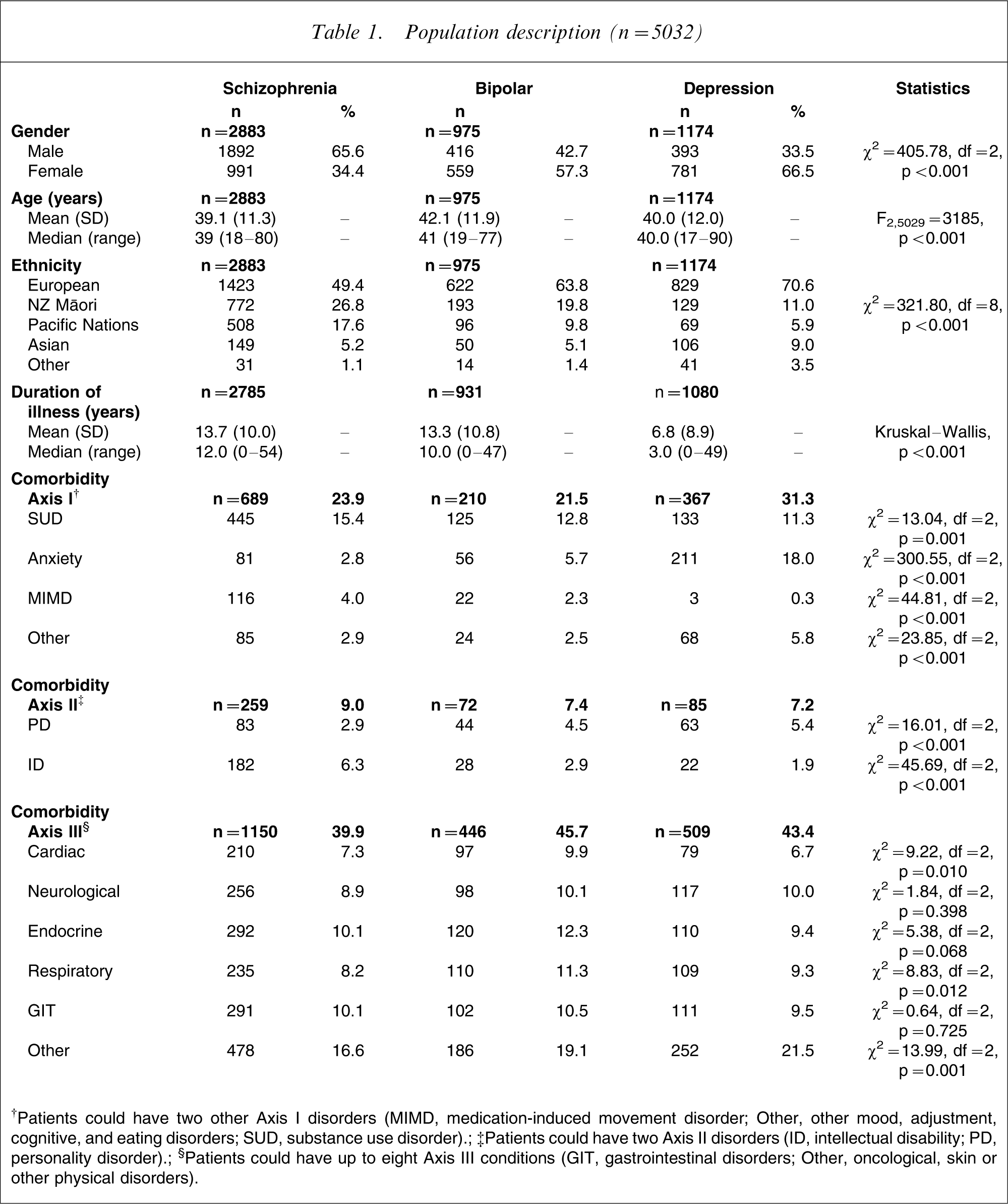
†Patients could have two other Axis I disorders (MIMD, medication-induced movement disorder; Other, other mood, adjustment, cognitive, and eating disorders; SUD, substance use disorder).
‡Patients could have two Axis II disorders (ID, intellectual disability; PD, personality disorder).
§Patients could have up to eight Axis III conditions (GIT, gastrointestinal disorders; Other, oncological, skin or other physical disorders).
Social and functional characteristics
Intimate relationships
Two-thirds of the outpatients with schizophrenia had never married (single) and <15% were living as married (Table 2). For outpatients with bipolar disorder and depression approximately one-third (36% and 27%, respectively) had never married and between 37% and 48% were living as married. In a general population sample the rate of never married was 32%, and 50% were living as married [20]. A logistic regression was run to control for other confounding variables on the binary outcome of being in a relationship with a partner (living as married; Table 3). Primary diagnosis remained significant in the model (p < 0.001), and gender (p < 0.001), age (p < 0.001), ethnicity (p < 0.001), duration of illness (p < 0.001) and Axis II comorbidity (p < 0.001) were also found to be associated with this outcome.
Social and functional characteristics
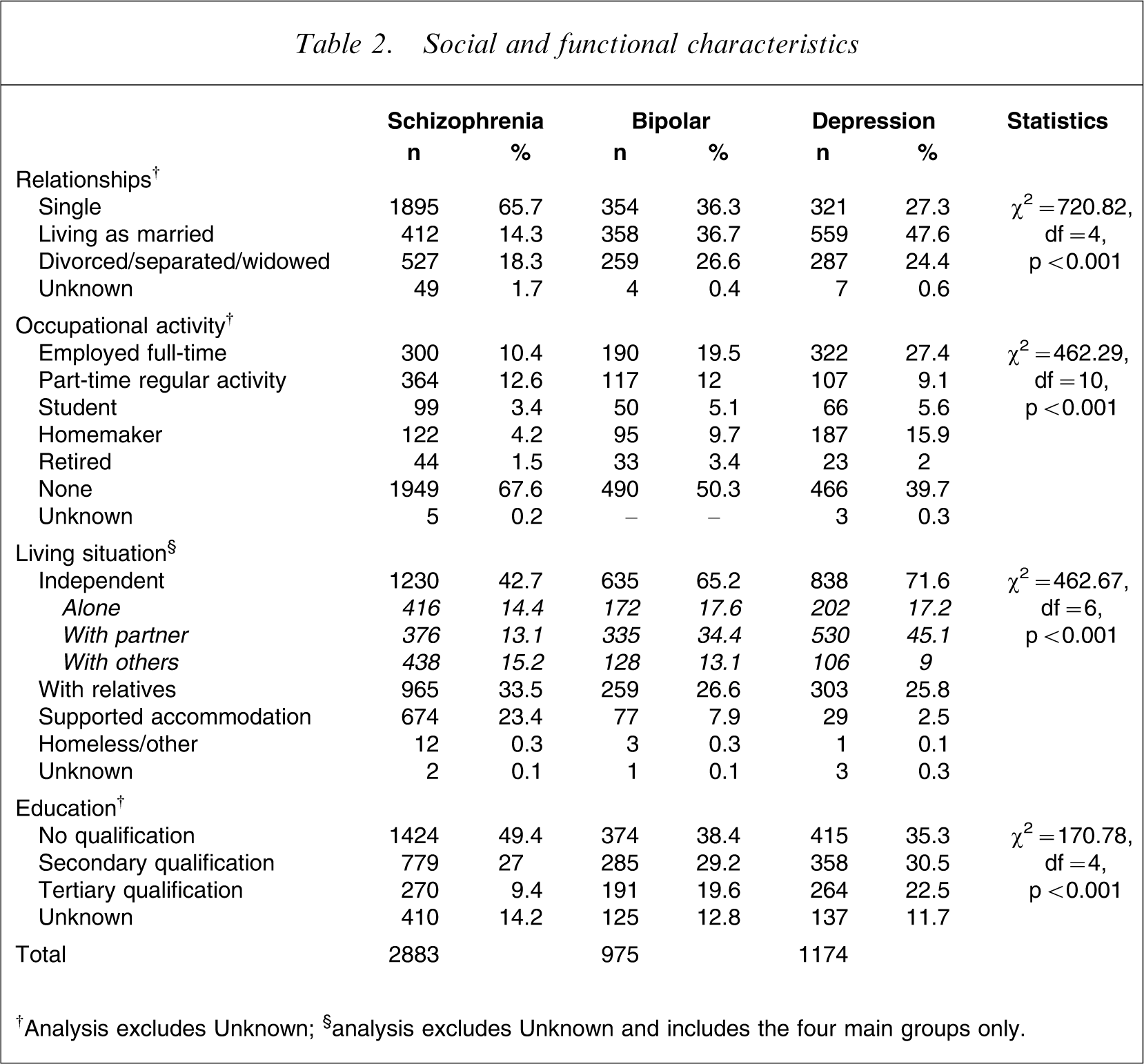
†Analysis excludes Unknown; §analysis excludes Unknown and includes the four main groups only.
Multiple logistic regression
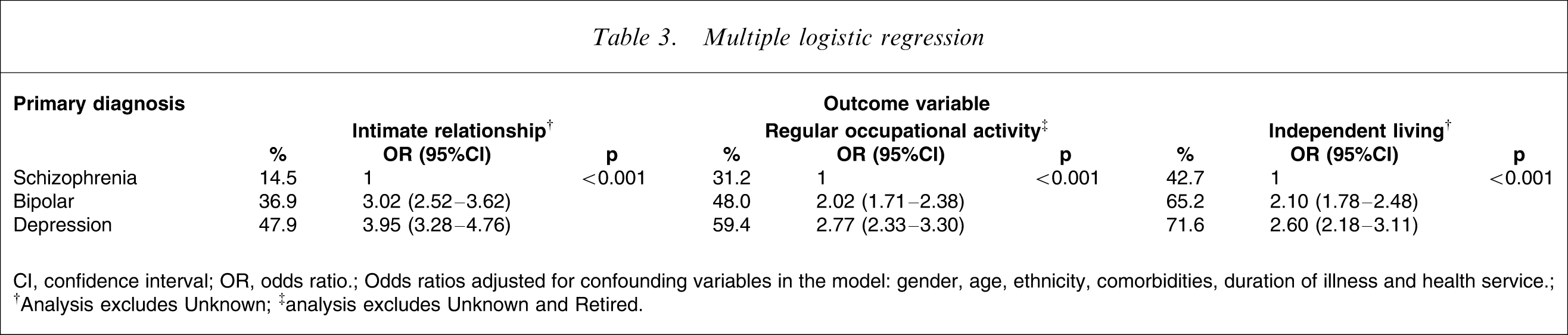
CI, confidence interval; OR, odds ratio.
Odds ratios adjusted for confounding variables in the model: gender, age, ethnicity, comorbidities, duration of illness and health service.
†Analysis excludes Unknown; ‡analysis excludes Unknown and Retired.
Occupational activity
Table 2 lists the occupational activity recorded for the three diagnostic groups. Having any occupational activity (excluding unknown and retired) was grouped and analysed as a binary outcome of any regular activity. More than two-thirds (68.8%) of the schizophrenia group were not reported to be involved in any form of regular occupational activity. There was a significant difference across the three groups; the proportion reduced in the bipolar group (52%) and reduced further for depression (41%). While it is not possible to compare the study data directly with the 2001 employment census figures, the overall picture is for a substantially lower rate of unemployment in the general population (7.5%) than in this mental health population.
The logistic regression analysis for having a regular occupational activity found primary diagnosis to be significant (p < 0.001) along with all other controlling variables in the model (Table 3).
Living situation
Forty-three percent of the schizophrenia group were living in some form of independent situation (including alone, with their partner or with others in shared rental accommodation e.g. flatting), 33.5% with their family, and just under one-quarter (24%) were living in supported accommodation (group mental health homes) facilitated by mental health services (Table 2). In contrast, there was a higher rate of independent living for both groups with an affective disorder and very few were living in supported accommodation.
Primary diagnosis was found to be significantly associated with the independent living outcome of interest in the regression model (p < 0.001). Gender (p < 0.001), age (p < 0.001), ethnicity (p < 0.001), duration of illness (p < 0.001), Axis II comorbidity (p < 0.001) and health service (p < 0.001) were also found to be associated with this outcome (Table 3).
Education
Half of the outpatients with schizophrenia had left secondary school with no qualification and <10% had completed a tertiary qualification (Table 2). For depressed and bipolar outpatients 35–38% had left secondary school with no qualification and 20–22% had a tertiary qualification. In a population survey 28% had left secondary school with no qualification and 32% had a tertiary qualification [20].
Service utilization
There was a significant difference between the diagnostic groups in the total number of psychiatric admissions prior to the review point (Table 4). The schizophrenia and bipolar outpatients had similar rates of admission over the entire range (none, 1, 2–5, 6–10, 11–20, >20 admissions), but 68% of those in the depression group had never been admitted. In the 18 months prior to the review period, acute admissions were significantly higher in both the schizophrenia (27.5% had at least one admission; range 1–10) and bipolar outpatients (32.4% had at least one admission; range 1–7) compared with only 14.8% of those with depression (range 1–7).
Clinical characteristics
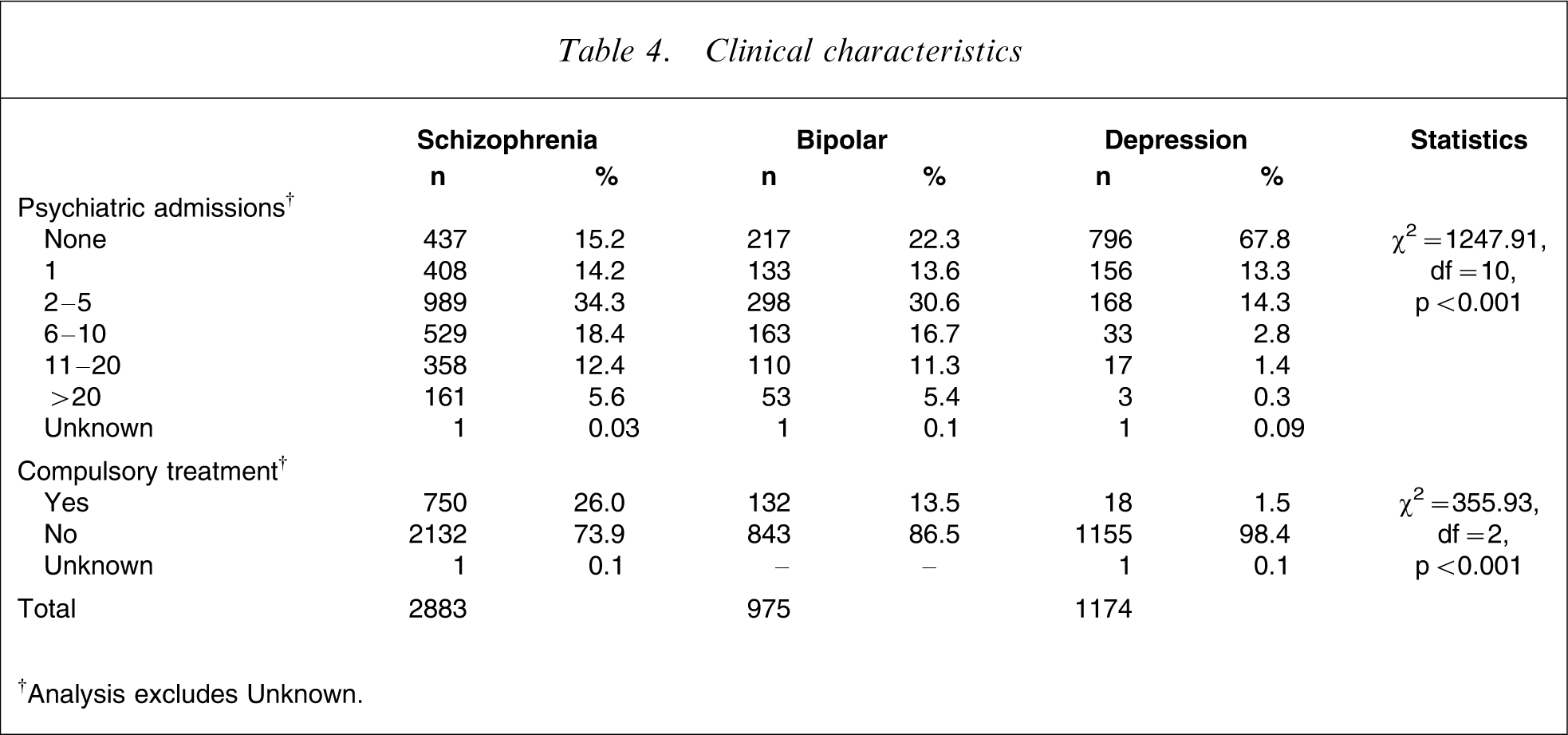
†Analysis excludes Unknown.
Receiving of compulsory community treatment under the Mental Health Act [21] at the time of the review (October 2004) was significantly higher for those with schizophrenia when compared to both affective disorders and was rare for those with depression.
Antipsychotic prescribing
Among the schizophrenia group, 96.8% (n = 2791) were prescribed antipsychotic medication and the majority (n = 2356; 84.4%) were prescribed antipsychotic monotherapy. The majority of treatment was oral therapy, with fewer than one-quarter (22.6%) prescribed an injectable depot antipsychotic (only 11 patients were receiving risperidone long-acting injection because it was not funded at the time of the study). Atypical antipsychotics were prescribed for 81.1% (n = 2263) of this group and clozapine was the most commonly prescribed antipsychotic (n = 911; 32.6%). Seventy-eight percent (n = 2180) of the schizophrenia outpatients were prescribed a total antipsychotic daily dose below 600mg CPZe day–1 (mean 425 mg; median 364 mg; range 8–2200 mg; SD 253 mg). Just under half (n = 1325; 47.5%) were prescribed a maintenance dose within the therapeutic dose range of 300–600 mg day–1 [22]. A very small proportion of outpatients (n = 72; 2.6%) were prescribed a total daily dose >1000 mg CPZe. Overall the treatment reflected both local and international clinical practice recommendations [10, 11, 23].
Discussion
This is the first large review describing demographic, social and functional characteristics and mental health service utilization for people with schizophrenia who live in the community and who are treated by specialist mental health services in New Zealand. This study found significant disruption and impairment of an individual's ability to lead a healthy meaningful role. Having some form of regular occupational activity, an intimate relationship with a partner, ability to live independently and achieve educational qualifications were significantly reduced for people with schizophrenia when compared to people with severe affective disorders treated by the same specialist services and were greatly at odds with those of the general population.
In terms of regular occupational activity, seven out of 10 individuals with schizophrenia had none. Establishing a relationship with a partner also appeared to be difficult for those with schizophrenia; almost seven out of ten 10 never been married. Educational achievements were also poor for those with schizophrenia. This high level of impairment is similar to other community-based studies examining the impact of schizophrenia conducted after deinstitutionalization in Europe and Australia [12, 24–27]. These studies also found consistently high rates of being single and unemployed in outpatients with schizophrenia. There were differences in living situation reported between the European studies and the New Zealand findings (comparative data were not available for Australia); Hansson et al. found high rates of independent living (70%), with only 19% of patients living with relatives [25]; Thornicroft et al. found similar rates to New Zealand for living with relatives (39% and 34%, respectively) [27] and Ochoa et al. found even higher rates (57%) [26]. This may be due to cultural differences and attitudes to a nuclear versus extended family approach to living in these countries, rather than mental illness per se.
The present study found that one in every four outpatients with schizophrenia was living in supported accommodation. Most commonly, this is a group home situation shared by mental health patients in which the placement is determined by mental health services. Comparing usage rates of this type of living environment globally is difficult because of the different availability of this type of public resource. In New Zealand it appears to be a common form of housing for individuals with schizophrenia. However, studies examining mental health patient perspectives have found that living independently was consistently preferred to living with other people with a mental illness [28, 29].
Outpatients with schizophrenia and bipolar disorder had significantly more psychiatric admissions than those with major depression. This is possibly related to the much shorter duration of illness observed in the depression group, but may be a consequence of inpatient bed shortages and the resulting ability to admit only those with the highest acuity and disturbed behaviour. Outpatients with schizophrenia were also twice as likely to receive compulsory community treatment as those with bipolar disorder, indicating a higher need for service intervention.
Overall the outpatients with schizophrenia were consistently the most impaired; those with depression the least and the bipolar group were in between. These findings remained significant even when controlling for other variables in the model. Higher levels of disability in outpatients with schizophrenia compared to affective disorders were also found in the 1997 Australian National Survey of Psychotic Disorders [12], and a review of health-related quality of life in bipolar disorder reported that this was similar to those with depression, but better than those with schizophrenia [13]. However, Dickerson et al. have suggested that social functioning and neurocognitive deficits may not be diagnosis specific; that is, the degree of impairment is similar between bipolar disorder and schizophrenia [30]. This present New Zealand study, however, found significant differences between the three diagnostic groups on all social and functional characteristics and service utilization.
Optimal treatment for schizophrenia recommended by current clinical practice guidelines focuses on both symptom and functional recovery, with a range of pharmacological, psychosocial and psychological interventions [10, 11, 31]. The cost-effectiveness of optimal treatment for schizophrenia with current evidence-based interventions has, however, been shown to avert only 22% of the burden of schizophrenia; most of the burden of schizophrenia was unavertable with best treatment [32]. Andrews et al. did find that providing optimal treatment was no more expensive and significantly increased the health gain for schizophrenia, reinforcing the importance of evidence-based care [32].
Antipsychotics are identified as a vital ingredient in the package of care and more specifically the atypical antipsychotics first line. Clozapine is recommended as early as possible for treatment-resistant schizophrenia and polytherapy is not recommended except for brief periods of switching. The present findings confirm that the atypical antipsychotics were the treatment of choice for most outpatients with schizophrenia and clozapine was the most commonly prescribed antipsychotic. The majority of outpatients were receiving antipsychotic monotherapy by the oral route and doses were within the recommended range. In summary the present study found that the antipsychotic prescribing practice for the treatment of schizophrenia was consistent with current evidence-based practice.
Psychosocial interventions (including family interventions, cognitive behaviour therapy and vocational rehabilitation) are also recommended to be provided to schizophrenia patients and their families [10]. While pharmacological care in this clinical setting was found to be evidence based, other psychosocial and psychological treatments are not readily available to patients and their families with schizophrenia in New Zealand [O'Hagan M, Mental Health Commissioner: personal communication] and there are no local studies or reports documenting the size of this gap in service provision. However, provision of a broader range of services is reflected in the recovery vision sought by mental health service users in the overall development of services in New Zealand over the next 10 years [33].
When interpreting the results of the present study, there are a number of limitations that need to be considered. This was a cross-sectional, retrospective review of information recorded in patient clinical files. Although a prospective study that gathers data by interviewing patients using validated questionnaires can collect specific information, this design is limited to smaller numbers of patients and potential biases in the patient group who consent to participate in the study, that is, patients with time to participate may be less likely to have a regular occupational activity. Additionally, treatment may not represent real-world practice in such a study because the prescriber is aware that their interventions are being reviewed. The present findings represent real-world antipsychotic prescribing for schizophrenia; reflecting the total antipsychotic regimen that the prescriber intended the patient to take at the time of the review, but the study did not explore adherence to treatment or the clinical effects of treatment.
The present study is limited by the quality and availability of information that has been recorded by members of the mental health team for each patient, for example educational qualifications were poorly recorded and this is reflected in the 13% unknown category. However, the study population included all patients actively engaged in specialist care at the time of the study and does not suffer from participation bias from patients or prescribers. Comparison with national data such as census counts also needs to be undertaken with caution, because the information in the present study was collected in a different manner for a different purpose.
The cross-sectional nature of the study means that the impact of treatment over time on a serious mental disorder cannot be inferred from the findings; they merely provide a snapshot of the social and functional status of these outpatients irrespective of the current treatment plan. This snapshot does not, for example, provide information regarding duration of access to evidence-based pharmacological treatment for the outpatient sample. It is possible, therefore, that these social and functional outcomes may continue to improve over time.
The present findings, while limited by the nature of the recording, provide information on current trends in social and functional impairment and patterns of care in schizophrenia compared to severe affective disorders in New Zealand. The large size of this outpatient study cohort receiving treatment in a public mental health service should strengthen the representativeness of the study.
In conclusion, the present study showed that significant impairment in social and functional roles and extensive use of specialist mental health service use still exist for patients with schizophrenia despite delivery of evidence-based pharmacological treatment. While acknowledging that a large proportion of the burden of schizophrenia is unavertable with existing interventions (contributed by early onset in late adolescence, lifetime course and neurocognitive and negative symptoms inherent in the clinical nature of schizophrenia), improvement in health outcome is possible with optimal treatment incorporating a range of evidence-based, cost-effective interventions that focus on both symptoms and function. Better understanding of this complex disorder is also needed so that research into new interventions is well directed.
Footnotes
Acknowledgements
The author would like to thank the Northern District Support Agency, Eli Lilly NZ, AstraZeneca NZ and Janssen-Cilag NZ for an unrestricted research grant. Thanks also to Kirsten Norris, Morgan Kelly and Karen Day for data collection and entry, Mental Health Services and staff from Waitemata, Counties Manukau, Auckland and Northland DHBs, Dr Grant Paton-Simpson for database support, Elizabeth Robinson for statistical advice and Professor Peter Joyce and Assoc Professor Janie Sheridan for support and feedback.