
Abstract
Child and adolescent mental health services in New Zealand have historically been underresourced [1, 2]. In 1998 the Mental Health Commission Blueprint for Mental Health Services in New Zealand stated that the child and adolescent mental health area was the most dramatically deficient within the mental health sector in terms of staffing [3]. In recent years there has been a considerable increase in funding for child and adolescent mental health services [4, 5]. However, despite this increase in funding, progress toward Blueprint staffing guidelines has been slow [5]. This lack of progress is concerning, and staffing issues in child and adolescent mental health services demand attention. The lack of progress in the area is compounded by the failure of many District Health Boards to fill their vacant positions [5]. Staffing was a particular problem in the northern region of the country, where 22% of the District Health Board-funded community child and adolescent mental health positions were reported vacant as at 30 June 2003 [5].
Career choice and attitudes to certain practice areas will inevitably impact on the health-care workforce, its development and a nation's health services. This is especially significant for areas such as child and adolescent mental health that struggle to recruit and retain suitably qualified staff. What is not yet known is how people can be encouraged to consider certain specialist areas as a career choice. Related studies conducted in the area of vocational psychology have shown that personal interest is strongly predictive of job choice and satisfaction [6–10]. Other experts in the field suggest that job attributes such as the nature of the work, advancement opportunities, work location, and the industry also have a strong and consistent impact on career intentions and job choices [11, 12]. However, it is difficult to generalize findings from vocational psychology research because these factors have not been systematically studied in relation to undergraduate health-care professionals.
Previous studies in the area of health students and their career intentions are frequently small in scale, with fewer than 100 participants [13–31], and are often conducted with one professional group [13, 19, 21, 23, 26, 31–38]. Results from this limited body of research suggest that classroom and placement experiences can positively influence students’ career intentions [15, 16, 20, 27, 39–41].
Although they are used throughout New Zealand's child and adolescent mental health services, nurses, occupational therapists and social workers qualified in New Zealand receive minimal training in child and adolescent mental health at undergraduate level [25]. The respondents in the Peters study of child and adolescent mental health content in undergraduate courses expressed an interest in increasing training in the area [25]. Additionally, providing training has the potential not only to increase students’ theoretical knowledge, but also to encourage people to work in child and adolescent mental health. Funding from the Ministry of Health for workforce development made it possible to develop a workshop to increase undergraduate training in child and adolescent mental health and to measure the impact of this on the career intentions of students undertaking the training. The present hypothesis was that a workshop on child and adolescent mental health would impact favourably on students’ career intentions to work in child and adolescent mental health.
Method
Design
A prospective study with pre-workshop, post-workshop and follow-up measurements (3–16 weeks after the workshop) was conducted to identify whether training in child and adolescent mental health positively influenced nursing, occupational therapy and social work students’ career intentions in relation to child and adolescent mental health.
A quality of teaching questionnaire was also administered after the workshop for student and educator participants. The inclusion of this measure was based on the assumption that an engaging and interesting workshop would be more successful in encouraging students to consider a career in child and adolescent mental health.
Study population and recruitment procedure
To be included in the study, participants needed to be degree-level nursing, occupational therapy and social work students at educational institutions in New Zealand. Educational institutions were excluded from the study if they provided education at less than degree level (i.e. National Diploma, Level 6) or at a postgraduate level. These exclusion criteria were set to ensure that participating students were studying at a comparable level.
Letters were sent to the heads of schools/departments of all eligible courses in January 2004 offering a free 3 h workshop on child and adolescent mental health for students. If heads of schools/departments gave consent then students and staff could be asked to participate in this study.
Ethical approval for this study was sought and granted by the University of Auckland Human Participants Ethics Committee prior to commencement. In accordance with ethical approval, written consent from the heads of schools/departments and educators was obtained before the workshops started. Participants indicated consent by completing the questionnaires, after reading the participant information sheet that was provided to heads of department, educators and student participants. The information sheet clearly stated that if individuals did not wish to participate they could elect not to complete questionnaires.
Measurement
Because there is no established instrument to measure allied health students’ career intentions we developed a new measure. Hence, a self-report questionnaire was created specifically for the current study to gather information from respondents about their career intentions. This questionnaire was developed in consultation with allied health professionals and an experienced biostatistician. A postgraduate research group reviewed it, before it was piloted and subsequently used with the student participants. The questionnaire was called the Career Intentions Questionnaire (CIQ) and was divided into three sections: demographic data (including age, sex and ethnicity); students’ ratings of their stated career intentions in nine areas (based on 100 mm-long visual analogue scales); and a survey of factors thought to impact on students’ career intentions. Students were asked to rate their intentions to work in the nine areas because it was thought that students might have more than one career path in mind.
The Quality of Teaching Questionnaire (QTQ) for student and educator participants was based on standards of established evaluation of teaching quality at the University of Auckland. We selected 12 key statements from the database of statements to evaluate the workshop's quality of teaching. These statements focused primarily on the content of the workshop and the teaching process rather than factors associated with the teacher/presenter to provide information on a planned adaptation of the workshop to an interactive CD-based teaching resource. The QTQ was administered after the workshop for students and their educators.
Workshop development and content
To ensure that the content of the workshop was theoretically sound and was appropriately matched for the targeted undergraduate students, three advisory groups were established and consulted before the workshop design and content was finalized. The three groups consisted of an internal advisory group (made up of child and adolescent mental health experts at the University of Auckland), an external advisory group (which included interested educators within nursing, occupational therapy and social work) and a Maori advisory group (consisting of a Kaumatua/elder from the University of Auckland, and Maori child and adolescent mental health clinicians). The workshop was interactive and multimedia in format and included video clips, illustrations/pictures and a powerpoint presentation. It was divided into three sections: child and adolescent development, recognition of child and adolescent mental illness, and evidence-based interventions in child and adolescent mental health.
Statistical analysis
The same participants were used across the measures to reduce the influences of extraneous variables on the dependent variable. The differences in change in career intentions scores over time between the occupational groups were analysed using generalized mixed linear models that allowed for repeated measures over time and for students’ educational institutions. Age, gender and ethnicity data were included in the models. To investigate whether any differences found were likely to be related to the workshop, changes in intentions to work in child and adolescent mental health were compared with changes in intentions to work with older adults. The quality of teaching data was converted to a summary score. Kruskal–Wallis and Mann–Whitney U-tests were used to test differences in medians between groups. SPSS (2002; SPSS Inc., Chicago, IL, USA) and SAS (version 9; SAS Institute Inc., Cary, NC, USA) statistical packages were used for analyses.
Results
Eighteen nursing, two occupational therapy and eight social work schools were invited to participate in this study (28 in total). As a result of the letters sent to the head of departments/schools and follow-up telephone contacts, 14 workshops (excluding the pilot) were scheduled with students and their educators and these were conducted in seven centres throughout New Zealand. A telephone survey of educational institutions that did not participate in the study was conducted to ascertain their reasons for not taking part. Of those that responded, the majority (six institutions) declined to participate because staff were new to the institution or were too busy to organize, coordinate or respond to the workshop request. Three institutions did not participate because the letter was not circulated to the relevant staff, or their expression of interest was not received.
Before the workshop, 373 students (representing an 80% class attendance rate) completed the CIQ, 347 students completed the CIQ after the workshop and 236 students completed the CIQ at the follow-up point in time (representing a 63% follow-up rate).
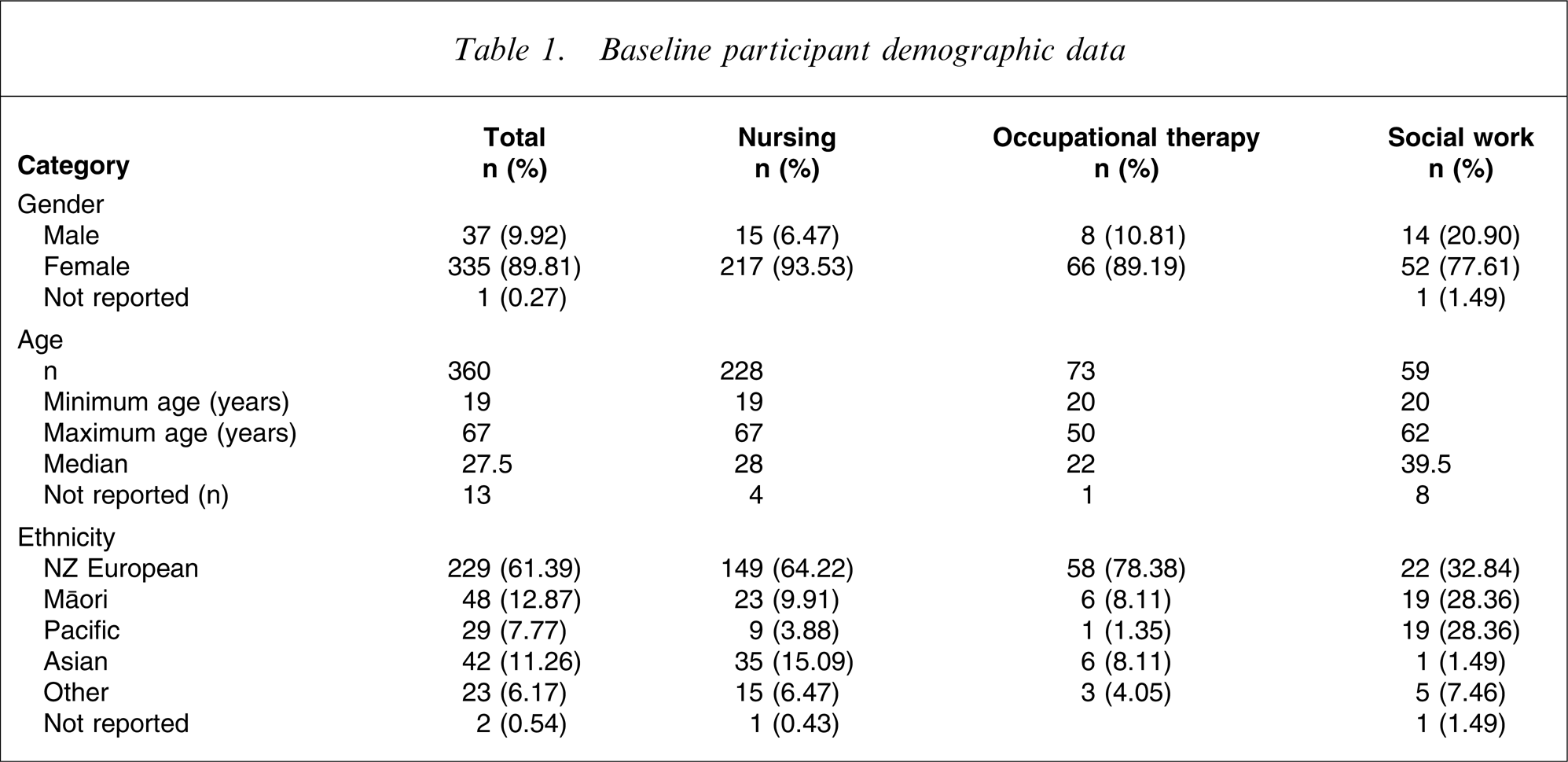
Table 1 presents the demographic characteristics of the study participants before the workshop. The participants were predominately women. The median age was 27.5 years and the majority of participants were New Zealanders of European descent.
Baseline participant demographic data
Intention to work in child and adolescent mental health
The workshop had a positive impact on students’ career intentions in relation to child and adolescent mental health, but this was not sustained longer term. A repeated-measures analysis showed an overall time effect (F2,546=16.29, p < 0.0001). Further investigation of this difference was carried out using a multiple comparison test (Scheffe test), which showed a highly significant positive increase in career intentions toward child and adolescent mental health between pre-workshop and post-workshop ratings (p < 0.0001), which dropped again between post-workshop and follow-up ratings (p = 0.004), with no change between pre-workshop and follow-up assessment (p = 0.43).
There was no differential effect by students’ professional group (p = 0.08), ethnicity (p = 0.6), gender (p = 0.75) or age (p = 0.26). Figure 1 shows students’ mean intentions (±95% confidence intervals) to work in child and adolescent mental health, before and after the workshop, and at follow up. Responses are missing on the child and adolescent mental health statement from 11 to 25 of the surveys over time because not everyone answered all of the statements of the questionnaires.
Intention to work in child and adolescent mental health, mean±95% confidence intervals.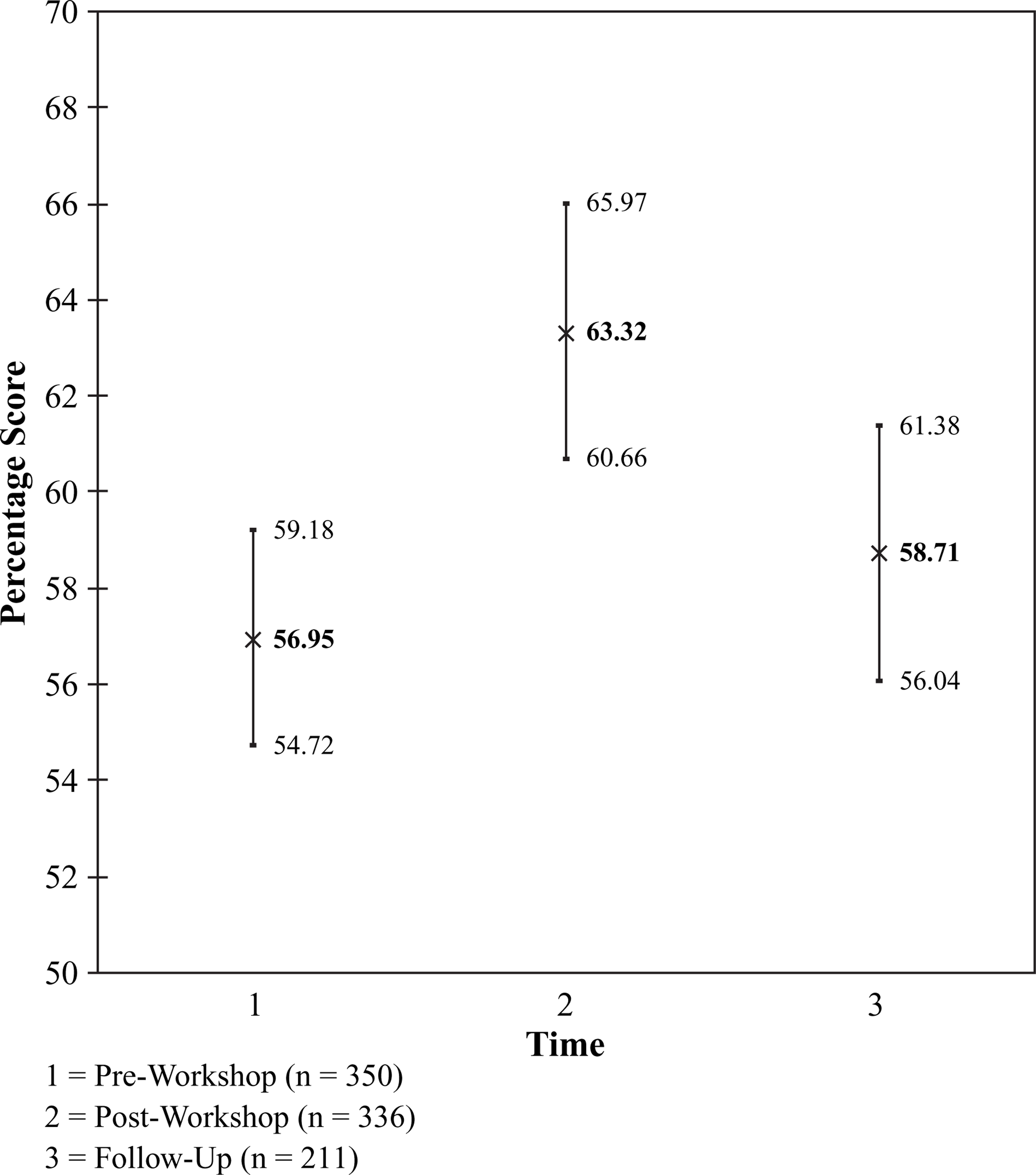
Working in child and adolescent mental health was also found to be consistently popular for a number of students. Seventy-three participants (20% of the pre-workshop participants) rated working in child and adolescent mental health very favourably (with ratings of between 80 and 100, maximum favourable rating = 100). Of those 73 participants, 61 continued to rate the area very favourably over time, and a minority (n = 6) gave follow-up ratings of <80 (data for six participants were missing because they completed only the pre-workshop questionnaire).
Intentions to work with older adults
As expected, there was no change in intentions to work with older adults after the workshop although repeated-measures analysis showed an overall time effect for intentions to work with older adults (F2,542=3.96, p = 0.02). However, this was due to a change after the workshop (i.e. ratings between post-workshop assessment and follow up). Perhaps this was to do with other teaching and/or placement experiences that took place after the workshop, which positively influenced students toward working with older adults.
Quality of teaching questionnaires
A total of 328 student participants responded to all 12 statements in the QTQ and their total score was out of a possible score of 60 (most favourable). The ratings for the workshop were extremely positive, with an average score of 55/60 for nursing, 53/60 for occupational therapy and 54/60 for social work participants. A series of Kruskal–Wallis tests showed no significant associations between the total QTQ median scores and students’ ethnicity (χ2(df = 4) = 2.64, n = 306, p = 0.6), professional group (χ2(df = 2) = 2.39, n = 328, p = 0.3), age (χ2(df = 2) = 1.48, n = 293, p = 0.5), or gender (χ2(df = 1) = 0.20, n = 306, p = 0.7).
The average total score for educators in the QTQ out of 60 was 55.5. A series of Mann–Whitney U-tests found that for 11 out of the 12 statements, there were no significant differences between student and educator ratings, with the exception being statement 4 (‘The multimedia format of the session was effective’), when educators gave significantly lower ratings (Mann–Whitney U = 1646, Z = − 2.198, p = 0.028). But if allowance is made for multiple testing this does not remain significant.
Discussion
We have shown that a workshop or classroom teaching can positively influence students’ career intentions toward a practice area. The study involved a large group of students, who would go on to become nurses, occupational therapists and social workers. One would assume that this group would already be predisposed to wanting to work in child and adolescent mental health because they had already chosen to train in ‘helping professions’. However, the group was far from homogeneous, and therefore students were unlikely to all respond in the same way. Although we attempted to promote the area to a large group, it is unrealistic to think that every student would want to work in child and adolescent mental health. A large group of students would not want to work in mental health and/or with children and youth, irrespective of any teaching session they participated in. Additionally, child and adolescent mental health services require only a small number of the most suitable students to eventually work in their services. Therefore, although we measured all of the students’ career intentions, it may be that those students consistently interested in the area should be the focus of further workforce development research and support.
The use of visual analogue scales allowed for subtle variations and trends over time to be observed. These patterns might not have been observed had the students rated their career intentions with Likert scales, because this form of measurement is less precise [42–44]. However, it is important to note that patterns that are statistically significant may not have translated into differences in job-hunting activities. Another issue of note is that some students simultaneously rated several visual analogue scales favourably, while others clearly rated only one area favourably. This highlights that some students will be more flexible (and possibly more easily influenced) in relation to their job choices than others.
Strengths and limitations of the study
The present study had a number of strengths: it was prospective in nature; it measured career intentions over time; involved half of all the institutions that provide degree-level programmes in nursing, occupational therapy and social work in New Zealand; and students could endorse a range of preferences in relation to their career intentions. This is thought to be important because Wittman et al. cautioned against thinking that students have only one career path in mind [45]. Therefore participants in the present study were able to select more than one area of interest and to express their level of interest in a continuous (as opposed to a categorical) manner.
However, the study also had some limitations, such as a potential recruitment bias (half of the eligible institutions did not participate) and it was not possible to establish how similar or dissimilar the study group was to the overall relevant student population. Like the vast majority of previous research in the field, the present questionnaires lacked evidence of their reliability and validity [11–17, 19–23, 25, 27, 29, 32–39, 41, 46–51]. However, every available step was taken to ensure that questionnaires were refined, improved and tested before their eventual use. The workshop exposed students to the content of work in child and adolescent mental health, but the focus was not on career prospects or opportunities in the field because this was an educational intervention. The workshop was generic in focus and did not provide information about profession-specific specialist areas, such as the nursing role in inpatient child and adolescent mental health. The follow-up period was variable (3–16 weeks after the workshop). Finally, the study did not measure actual job choice, but rather students’ career intentions. Job choice is an issue that requires further study. As the Ohman et al. study of physiotherapists in Sweden showed, students’ pre-graduation expectations may not accurately reflect the realities of the subsequent work environment [37].
Conclusion
The workshop led to a significant positive impact on students’ motivation to pursue a career in child and adolescent mental health, although this effect was transient. This would suggest that for a long-term effect more teaching may be required to increase the impact of the intervention. The impact of the intervention may also be increased if it is delivered in combination with other strategies, such as positive fieldwork placement experiences. Sixty-one students involved in the present study indicated a strong interest in working in child and adolescent mental health. If all of these students could be recruited to the area this would have a positive impact on the workforce, which in New Zealand is only 667 full-time equivalent community-based clinicians [52]. Attention to undergraduate training is an important component of any strategy to address the worldwide shortage of workers in child and adolescent mental health.
Footnotes
Acknowledgements
The authors thank the Ministry of Health for funding this child and adolescent mental health workforce development project via the Werry Centre (Department of Psychological Medicine, University of Auckland). We would like to thank all the advisors, educators and students involved in this project.