
Abstract
Insomnia is a common and major public health problem. Based on stricter criteria of insomnia, most of the recent studies have reported a prevalence of approximately 10–20% in the general population with a female predisposition [1–13].
Insomnia could be a normal transient reaction to acute stress, a symptom of underlying psychiatric or physical disorder, a discrete psychiatric disorder per se, or a risk factor for other psychiatric disorder. As a discrete psychiatric disorder, it was labelled as primary insomnia in DSM-IV [14], as non-organic insomnia in ICD-10 [15] and as psychophysiological insomnia in International Classification of Sleep disorders, second edition (ICSD-II) [16]. It has been reported that 10–54% of subjects with chronic insomnia suffer from primary insomnia [17–21]. In the community, the prevalence of primary insomnia was reported to be 1.3% in a telephone survey of 5622 subjects via the Sleep-Eval system [22]. These epidemiological studies supported a face validity of primary insomnia being a distinct clinical diagnosis. The establishment of a clinical diagnosis, however, also requires knowledge of its distinct aetiological factors, clinical course, outcome and prognosis. Long-term diagnostic stability of schizophrenia and affective disorders over 30–40 years has been shown to be 92.5% and 78.3%, respectively [23]. There were limited data showing whether primary insomnia was a short- or long-term disorder. Information about the natural history and consequence of chronic primary insomnia was also lacking [24]. To our knowledge, there has been only one 64 month follow-up study on 28 patients with primary insomnia [25]. Most of these 28 patients still reported sleep disturbance at the end of the follow-up period although a trend of improvement was noticed.
A number of population-based studies showed that insomnia was a risk factor for other psychiatric disorders [17, 26–34]. Most of these studies tried to exclude pre-existing psychiatric problems by structured interview. They reported an increased risk of developing depressive disorders (odds ratio [OR] = 2.0–39.8), anxiety disorders (OR = 6.3–20.3) and alcohol dependence syndrome (OR = 1.75–2.4) over a variable follow-up period of 1–34 years.
The aim of the present study was to investigate (i) longitudinal diagnostic stability and (ii) the factors associated with the development of other psychiatric disorders in primary insomnia patients in a psychiatric clinic.
Method
The present study was a combination of a retrospective case note review with a prospective follow up on the patients who were diagnosed as suffering from primary insomnia during their first consultation in a university psychiatric outpatient clinic at Prince of Wales Hospital, Shatin, Hong Kong, from 1995 to 2000. Their case notes and/or the computerized clinical database were first screened for the face validity of the diagnosis of primary insomnia.
Inclusion criteria included (i) age 18–65 years; (ii) satisfying the DSM-IV criteria [14] for primary insomnia and with at least 3 days of sleep problems per week during their first consultation; and (iii) written informed consent. Exclusion criteria included (i) presence of medical disorders that directly affected their sleep; and (ii) existence of prior psychiatric disorders before the patient's first consultation.
Figure 1 illustrates the methodology and recruitment procedure. The condition from the onset of insomnia (Tb) to the first interview (T1), which included the insomnia symptom profile at the first consultation T0 (presence of difficulty in initiating sleep [DIS], difficulty in maintaining sleep [DMS], early morning awakening [EMA], and the frequency of insomnia in days per week) and other psychiatric symptom, background and treatment history were retrieved from the case notes. Subjects were interviewed face to face twice, with the first interview (T1) done between December 2001 and March 2002 and a further 6 month prospective follow-up interview (T2) between July and September 2002.
Methodology and recruitment process. Tb, onset of insomnia; T0, first consultation; T1, first interview; T2, follow-up interview.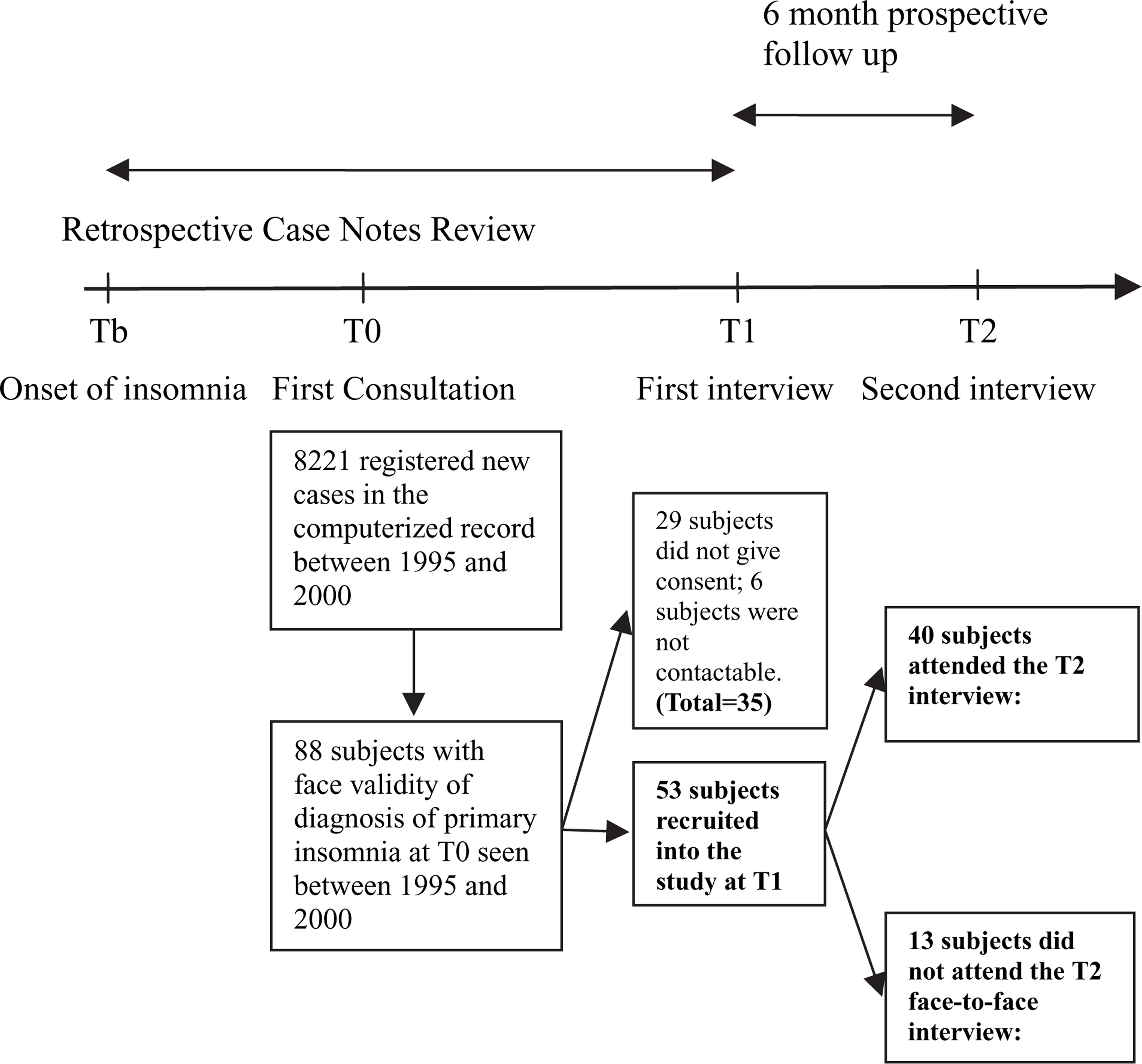
At T1 and T2, all subjects were further investigated with (i) a Chinese bilingual version of the Structured Clinical Interview Schedule for DSM-IV In-patient (SCID-I/P) version 2.0 [35, 36], with which the authors had ample experience in conducting the semi-structured clinical interview; (ii) a structured sleep questionnaire; and (iii) a visual analogue scale (VAS: 0–10).
The structured sleep questionnaire provided more details on the insomnia symptoms. This questionnaire has been used for epidemiological studies on sleep disorders including insomnia and narcolepsy [12, 37, 38]. The questions covering insomnia symptoms have face validity and the validity of self-report sleep duration in the questionnaire was also supported by actiwatch measurement [39]. The structured questions about insomnia were as follows: do you have difficulty in falling asleep (DIS); for those who answered ‘no’ or ‘seldom’, they would not be considered as suffering from significant DIS and would proceed to questions on DMS and EMA. For those who answered ‘sometimes’ or ‘always’, they would be asked about their sleep latency and also the frequency of DIS in the previous month with the choices of ‘no’, ‘occasional’, ‘1–2 times per week’, ‘3–4 times per week’ and “> 4 times per week’. A similar set of questions were asked for DMS and EMA.
Non-restorative sleep (NRS) was assessed with the question ‘Do you think you get adequate rest after sleep?’; choices of ‘inadequate’ or ‘poor’ meant NRS while ‘good’ or ‘satisfactory’ meant no NRS.
For the VAS, subjects were tested on the subjective severity of insomnia, perceived stress in the family (marital relationship, child care, relationship with parents or in-laws), work and financial aspects at T0 (by retrospective rating at T1), T1 and T2, respectively. Subjective deterioration in any one of these areas was defined as an increase in the visual analogue score between ‘T0 and T1’ or ‘T1 and T2’.
Subjects who developed other psychiatric disorders after T0 were classified into the disorder group, and those who did not were classified into the insomnia group. Within the insomnia group, symptom improvement was defined as frequency of insomnia fewer than 3 times per week at the time when they were last interviewed (either at T1 or T2). SPSS version 9.0 (SPSS Inc., Chicago, IL, USA) was used for data analysis. χ2 test, Mann–Whitney U-test and Student's t-test were used for comparing the disorder and insomnia group. Because of the small number of subjects, only factors with p < 0.05 were included in the survival analysis. Survival analysis with Kaplan–Meier analysis was used to analyse the duration of absence from other psychiatric disorders since the onset of insomnia. Cox regression analysis (using forward stepwise method) was used to explore the factors affecting the duration of absence from other psychiatric disorders.
This study was approved by the institutional Clinical Research Ethics Committee.
Results
From 1995 to 2000 there were a total of 13 896 new patients referred to the outpatient clinic at Prince of Wales Hospital (PWH), Shatin, Hong Kong, from general practitioners and other specialties. There was no pre-screening method as referred to the psychiatric diagnosis prior to the attendances in the psychiatric clinic. Altogether, there were 8221 patients within the age group of 18–65. Eighty-eight subjects out of these 8221 patients fulfilled the inclusion criteria, in which 53 eligible subjects (60.2%, M:F = 23:30) attended the face-to-face interview and were confirmed as suffering from primary insomnia by the SCID-I/P version 2.0 (Figure 1). Thirty-five subjects (39.8%) refused to join or could not be contacted, in which two of them developed depression after T0 as recorded in their case notes. Their age, sex ratio and the duration of insomnia before T0 was not significantly different from the recruited subjects.
At T1, 29 of these 53 subjects (54.7%) were still followed up at the clinic. Eleven subjects (20.8%) were receiving treatment from other medical clinics, and 13 subjects (24.5%) were not followed up by any western medical practitioners. The mean duration of insomnia symptoms of these 53 subjects before the first consultation at the psychiatric clinic (Tb–T0) was 11.0±9.6 years and the mean duration from T0 to T1 was 3.19±1.9 years (Figure 2). Follow-up study with face-to-face T2 interview was completed for 40 subjects at 5.8±1.6 months after T1. Thirteen subjects (24.5%) did not attend the face-to-face interview at T2. One of these 13 subjects developed other psychiatric disorder between T0 and T1 and was classified into the disorder group. In order to ascertain their outcome, these 12 subjects who did not attend the T2 face-to-face interview were further interviewed by phone at T2 in addition to reviewing their case notes. One subject died of malignancy 4 months after T1 interview and he had presented with insomnia 2 years prior to the diagnosis of malignancy. All these 12 subjects were not found to have any major diagnostic change compared to T1.
Survival function for all subjects (n = 53). Tb, onset of insomnia.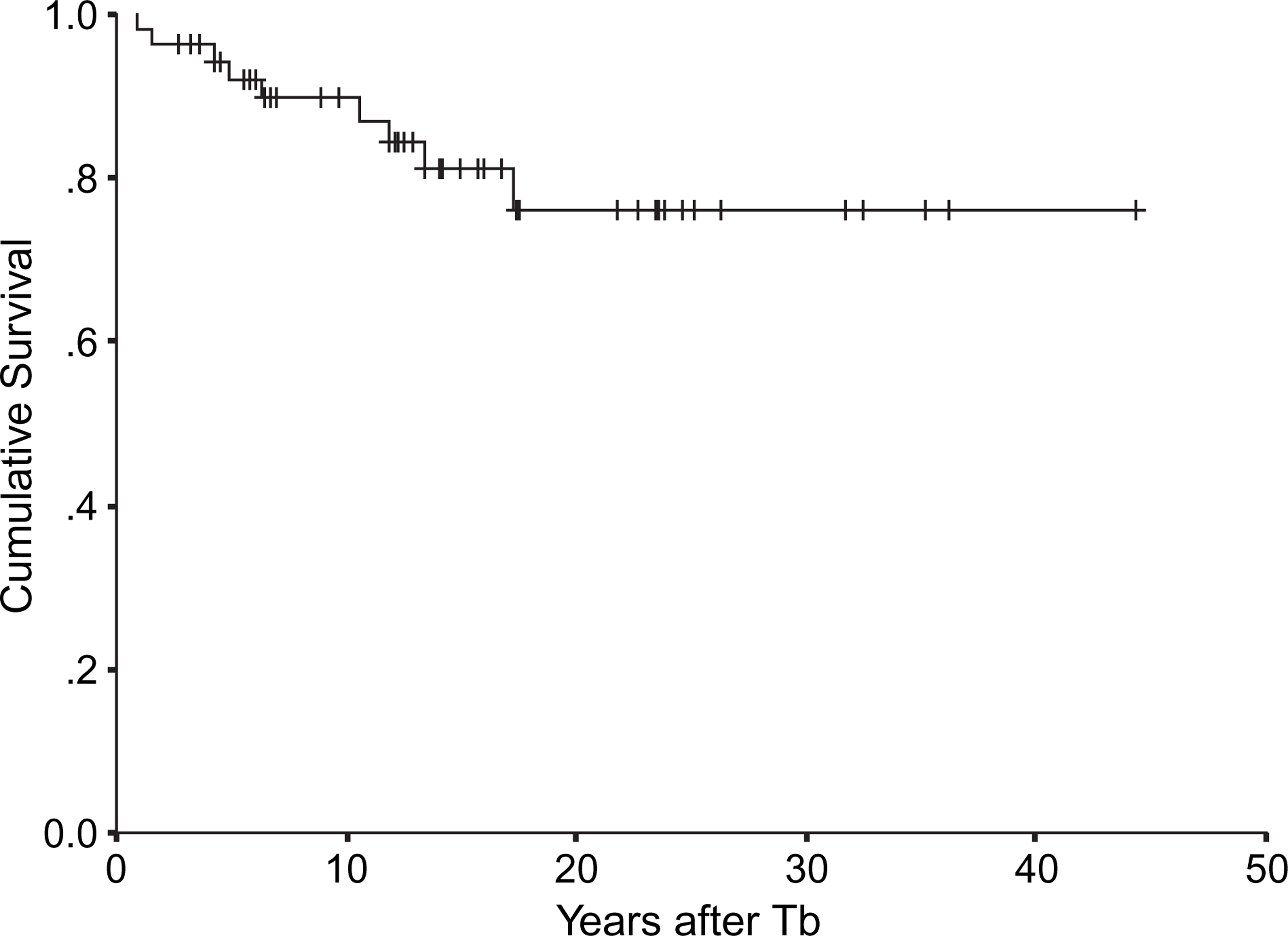
There were 44 subjects (83.0%) in the insomnia group with a median duration of 13.4±1.2 years (95% confidence interval [CI] = 11.0–15.9) after the onset of insomnia. Nine subjects (17.0%) were in the disorder group and they developed mood or anxiety disorders at a median duration of 6.3±2.2 years (95%CI = 1.9–10.7) after Tb and a median of 1.8 years (95%CI = 0–5.5) after T0 (Figure 3). The diagnoses included major depressive disorder (n = 4), dysthymia (n = 1), bipolar affective disorder (n = 1), anxiety disorder not otherwise specified (n = 2) and somatoform pain disorder (n = 1). Except for the subject with dysthymia who was diagnosed at T2 (because of the duration criteria this patient was diagnosed as having dysthymia 3 months after T1), all subjects were found to have developed other psychiatric disorders at the T1 interview.
Survival function of the disorder group (n = 9). Tb, onset of insomnia.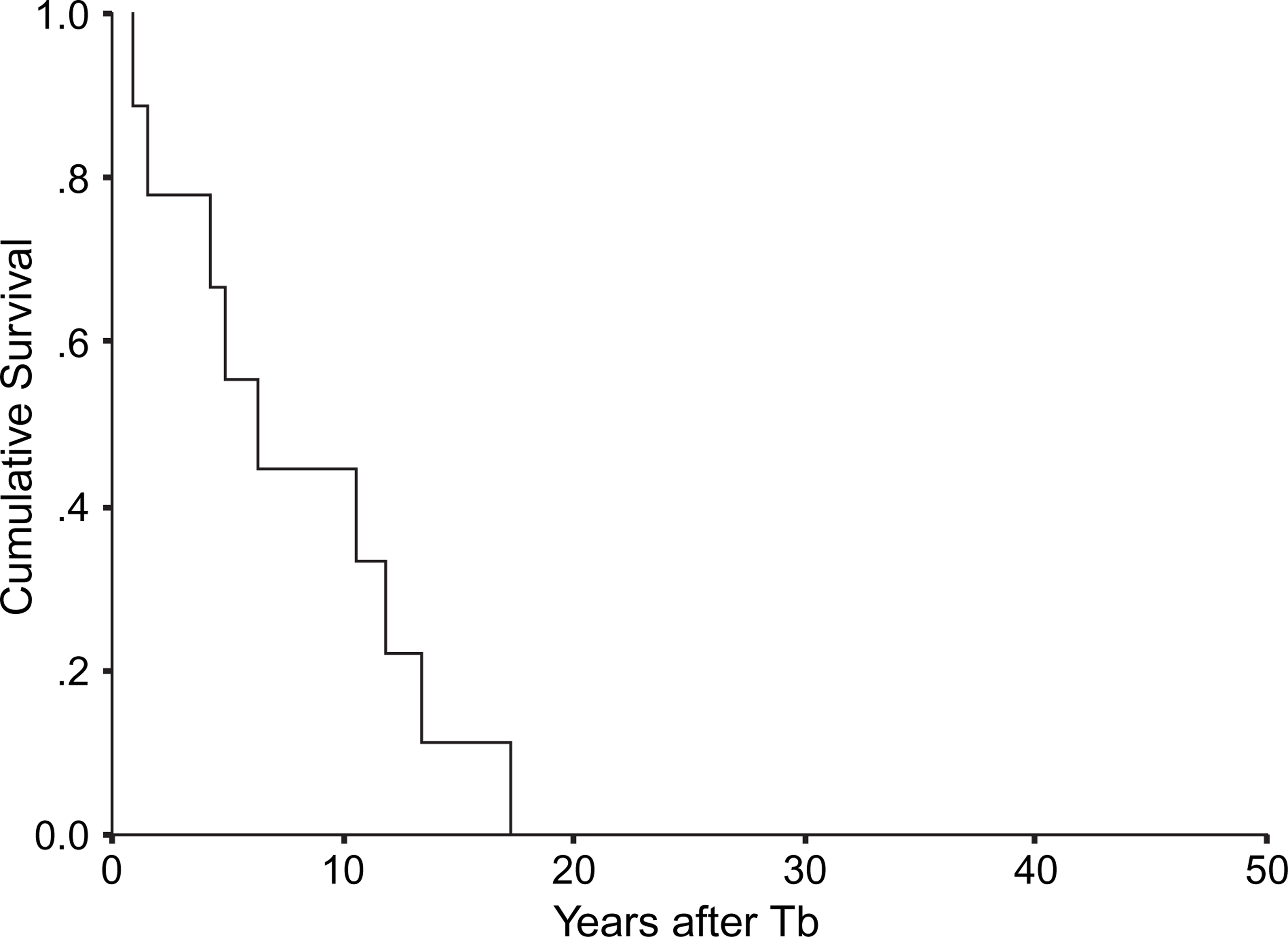
The demographic data and insomnia symptoms profile are given in Table 1. The disorder group reported a shorter duration of symptoms at the first consultation (Tb–T0), more number of days per week with insomnia complaint at T0 and more subjective deterioration of insomnia complaint from T0 to T1. There was no significant difference in the types of insomnia complaints (DIS, DMS, EMA) between the two groups at T0 and T1, although in both groups there was a reduction in the number of subjects having frequent insomnia complaints from T0 to T1 (15 out of 44 subjects in the insomnia group and three out of nine subjects in the disorder group reported a frequency of insomnia <3 days per week; Table 1). There was no significant difference between the two groups in the total number of types of insomnia complaints (i.e. no significant difference in single vs multiple types of insomnia).
Insomnia group and disorder group comparison
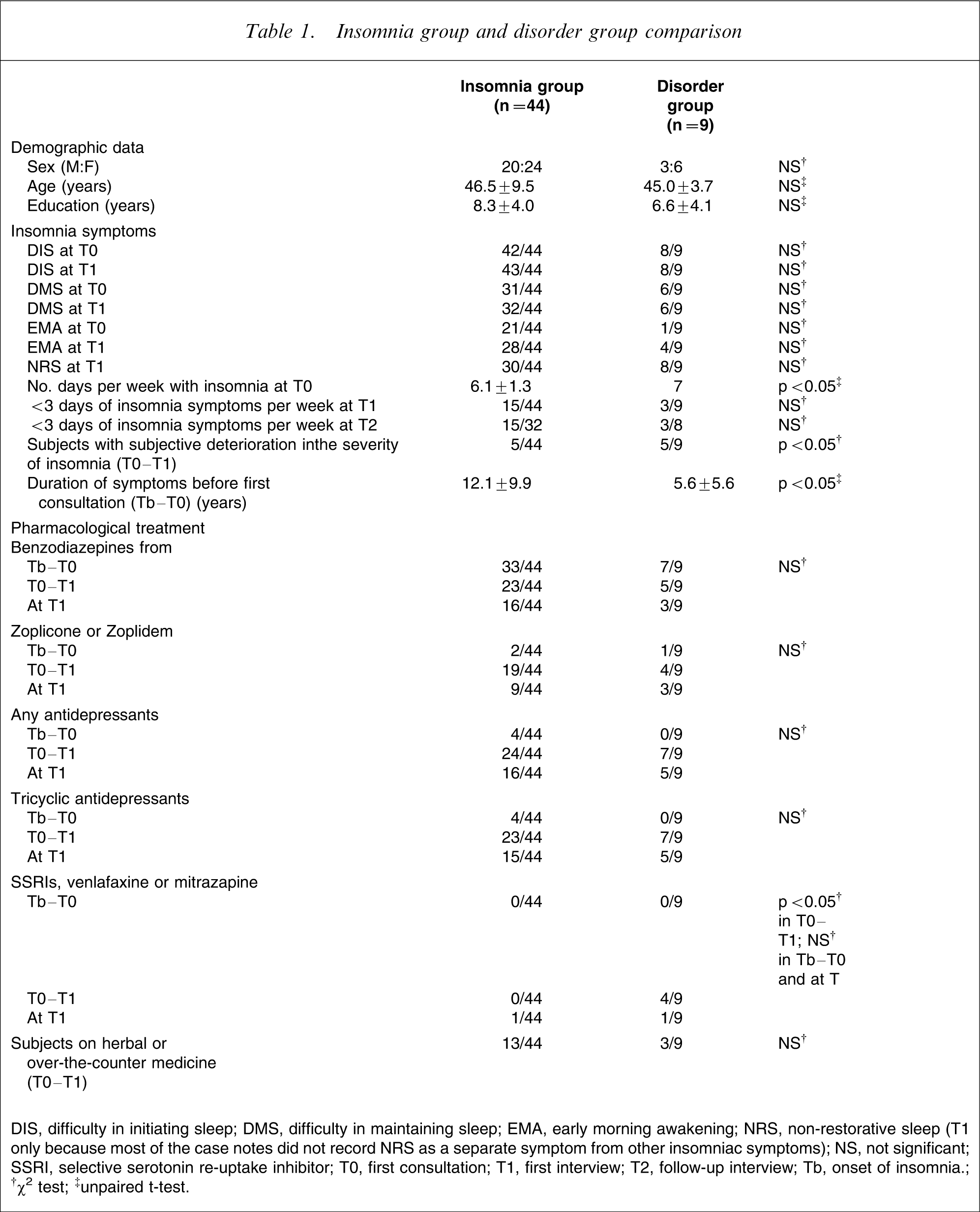
DIS, difficulty in initiating sleep; DMS, difficulty in maintaining sleep; EMA, early morning awakening; NRS, non-restorative sleep (T1 only because most of the case notes did not record NRS as a separate symptom from other insomniac symptoms); NS, not significant; SSRI, selective serotonin re-uptake inhibitor; T0, first consultation; T1, first interview; T2, follow-up interview; Tb, onset of insomnia.
†χ2 test; ‡unpaired t-test.
Thirty-eight subjects (71.1%) reported some background physical disorders, in which 21 (39.6%) reported pain symptoms but none of them reported their insomnia being directly affected by the pain. Seven (13.2%) had hypertension, four (7.3%) had diabetes mellitus, two (3.7%) had cancer, one (1.8%) had controlled systemic lupus erythromatosis without the need of steroid therapy, and one (1.8%) had idiopathic orofacial dyskinesia. The disorder group was found to have more background physical disorders (n = 1.44, mean rank 36.00) when compared to the insomnia group (n = 0.95, mean rank 25.16, p = 0.039).
There was no significant difference in the family history of psychiatric or sleep disorder. There was no significant difference between the two groups in the number of subjects having an anxious or obsessive–perfectionistic premorbid personality, as recorded in their case notes at T0.
Increased level of marital stress (Fisher's exact test, p = 0.026); increased level of financial stress (OR = 10.9, 95%CI = 1.8–63.6); more areas with increased stress (disorder group: mean rank = 35.2; insomnia group: mean rank = 25.5, p = 0.027) from T0 to T1 was more common in the disorder group than in the insomnia group.
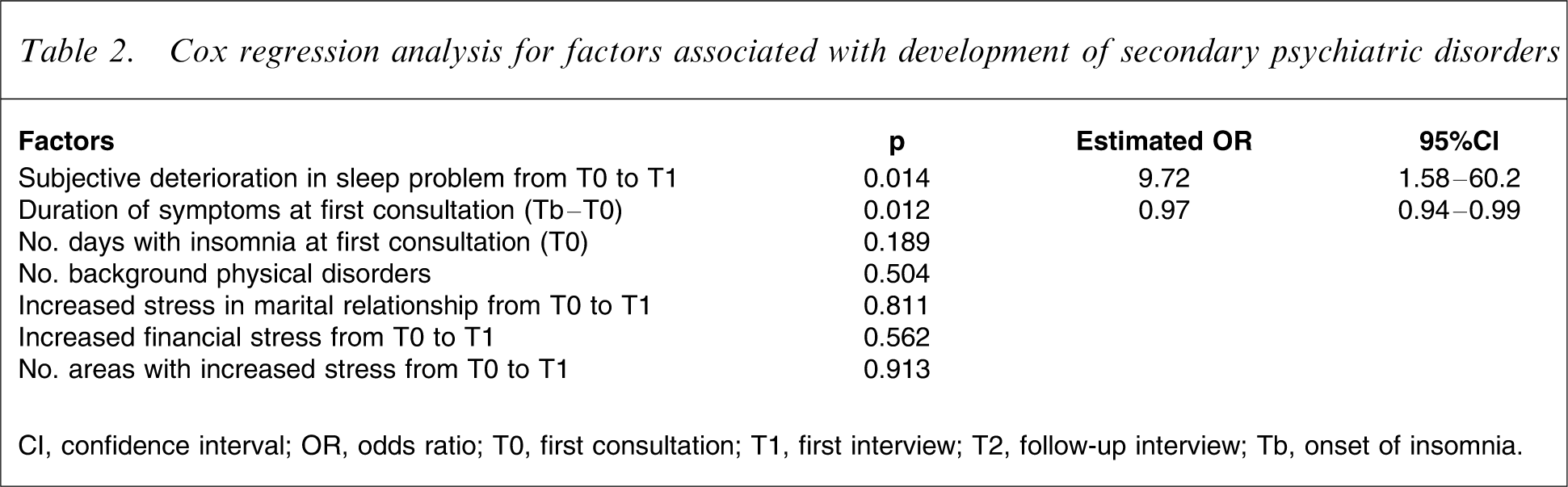
The significant factors were further investigated with Cox regression model (Table 2). Only the subjective deterioration in sleep symptoms from T0 to T1 (estimated OR of 9.72, 95%CI = 1.58–60.2, regression coefficient = 2.25) and a shorter duration of insomnia symptoms at first consultation (Tb–T0; estimated OR = 0.97, 95%CI = 0.94–0.99, regression coefficient = − 0.03) was significantly associated with the development of other psychiatric disorders.
Cox regression analysis for factors associated with development of secondary psychiatric disorders
CI, confidence interval; OR, odds ratio; T0, first consultation; T1, first interview; T2, follow-up interview; Tb, onset of insomnia.
The pharmacological treatment in both the insomnia and disorder groups is given in Table 1. There was a reduction in the use of benzodiazepine and increased use of non-benzodiazepine hypnotics and tricyclic antidepressants after the subjects were seen in the clinic at PWH. The increased use of selective serotonin re-uptake inhibitors in the disorder group was most likely a consequence rather than the cause of the development of other psychiatric disorders. Because the details and compliance of non-pharmacological treatment was not well documented in the case notes, they were not analyzed in the study.
Out of the 44 subjects in the insomnia group, 17 (38.6%) reported symptoms improvement, with six of them free from any medications (including Western and herbal medicine). For those subjects (n = 27) who did not have improvement in symptoms, they were older in age (48.7±6.9 years vs 42.9±11.9 years, p = 0.036), had lower education (6.9±3.7 years vs 10.5±3.6 years, p = 0.003), more tea consumption (OR = 4.1, 95%CI = 1.0–15.7), and did not receive antidepressant treatment before attending the clinic at PWH (Fisher's exact test, p = 0.018). Multivariate analysis using binary logistic regression showed that only the higher education level predicted symptom improvement (p = 0.008, estimated OR = 0.76, 95% CI = 0.62–0.93).
Discussion
In order to ascertain the accuracy of the diagnosis as well as to exclude prior psychiatric problems before the onset of insomnia, we used a combination of detailed case notes review and the structured clinical interview. Approximately 1% (88 out of 8221) of the psychiatric outpatients suffered from primary insomnia, with similar female predisposition as seen in the epidemiological studies [13].
The majority (n = 44, 83.0%) of the present subjects did not develop other psychiatric disorders with a median insomnia duration of 13.4 years. This suggested that primary insomnia was a long-term disorder in the present clinical population. In addition, approximately one-sixth of subjects (n = 9, 17%) developed subsequent mood disorder, anxiety disorder and somatoform disorder during their course of illness. Therefore the present result is consistent with the finding in the general population that primary insomnia is a risk factor for new-onset mood and anxiety disorder.
There have been controversies as to whether subjective perception or objective quantification of insomnia (e.g. as defined by number of days with insomnia) was more associated with psychiatric disorders. In univariate analysis, we found that there was a more frequent insomnia complaint (in terms of number of days per week at T0) in the disorder group than in the insomnia group. Similar finding was shown by Taylor et al. that an increased frequency of insomnia or awakening was related to increased depression and/or anxiety [34]. However, on logistic regression the present study shows only that subjective deterioration in insomnia and being an early help seeker (a shorter duration from Tb to T0) was associated with the development of psychiatric disorders. Improvement in the insomnia symptoms as measured by the sleep questionnaire (defined as <3 days of insomnia complaints per week) was not shown to reduce the risk in developing subsequent psychiatric disorders (Table 1). Edinger et al. similarly reported that subjective perception of insomnia, rather than objective quantification of insomnia, was associated with mood and anxiety symptoms [40]. In a study by Moul et al., depression-related insomnias and primary insomnias were separable only by characteristic symptoms of depression, but not by objective measurement in the frequency and severity of insomnia (including symptom counts and Pittsburgh Sleep Quality Index) [41]. Taken together, the clinical implication of the present finding in patients with primary insomnia is that a development of subsequent psychiatric disorder should be watched for if there is a complaint of deterioration in their insomnia symptoms.
In most clinical disorders it is expected that the longer the exposure to a risk factor, the more likely the occurrence of a subsequent disorder. In contrast, the present subjects with a longer history of insomnia before their first psychiatric consultation were not found to be at higher risk of developing subsequent psychiatric disorders. Hence, there might be two distinct clinical courses in the present primary insomniac subjects. The majority of them had a longitudinal diagnostic stability, but in a proportion of primary insomniacs this could either be a risk factor or even a prodrome for secondary psychiatric disorder.
The switching from benzodiazepine to tricyclic antidepressant was common among primary insomnia patients after being seen by psychiatrists [42]. Treatment with tricyclic antidepressants (mostly at low doses), however, was not shown to prevent the development of subsequent psychiatric disorder in the present subjects. Further study is thus needed in evaluating the role of antidepressant in preventing the development of future psychiatric disorders in primary insomnia, particularly in terms of the dosage and duration of treatment. Non-pharmacological treatment of insomnia has been shown to reduce depression after improvement in insomnia [43]. However, the lack of detailed record of the non-pharmacological treatment in the present subjects limited analysis in this aspect.
Approximately one-third (n = 17) of insomniac subjects reported symptom improvement during the course of their illness. Better education was shown to be the only predictive factor for improvement in the insomnia symptoms. This might be related to a better understanding and management of the illness. Better education has been shown to be a favourable prognostic factor in depression and other psychiatric conditions through better skills in solving life-related problems [44].
There were several limitations in the present study. The small sample size was definitely a problem. The retrospective design between Tb to T1 posed several problems: (i) the absence of a detailed record in the case notes about the premorbid personality or measurement with personality inventory at T0 made it difficult to determine the contribution of personality in the development of subsequent psychiatric disorder; (ii) the use of retrospective VAS in the measurement of psychosocial stress and severity of sleep problem might be subject to recall bias; and (iii) a number of insomniac subjects might not have been included in the study because they might have developed other psychiatric disorders well before their first consultation (thus decreasing the number of subjects in the disorder group), whereas some might have been in remission from their symptoms and did not require psychiatric intervention (thus decreasing the number of subjects in the insomnia group). A longer prospective follow-up period might also be needed to find those subjects who might need an even longer duration to develop subsequent psychiatric disorders.
In conclusion, the present study demonstrates the longitudinal diagnostic stability of primary insomnia and its role as a risk factor or possibly a prodrome for future psychiatric disorders. Clinically, there should be high vigilance on the development of secondary psychiatric disorders in those primary insomniac patients with aggravation in their insomniac symptoms and in those early help seekers.
Footnotes
Acknowledgements
The authors would like to thank the Hong Kong College of Psychiatrists for permission to publish this paper, which is part of the dissertation submitted for the Part III Examination 2002 for the first author. We would also like to thank Ms Mandy Yu for her help in data collection.