
Abstract
Keywords
Individuals with a diagnosis of borderline personality disorder (BPD) typically have difficulties in the regulation of affect, impulse control and interpersonal functioning [1]. Their attachment relationships tend to be unstable and fluctuate between idealization and devaluation of other, which is indicative of a fundamental difficulty in balancing the needs for both autonomy and intimacy [2]. The majority have experienced significant early relational trauma, which remains unresolved and continues to disorganize their mental functioning [3]. Attachment theory suggests that early trauma and disorganization of attachment are related to later personality dysfunction, and specifically to difficulties in interpersonal functioning, deficits in reflective function (the capacity to envision mental states in the self and others) and poor tolerance of negative affect [3]. Given these pervasive psychological and emotional deficits, it is likely then that parents diagnosed with BPD will experience difficulties in fulfilling their parenting role and in the promotion of secure attachment with their children [4]. Although there is increasing research interest into the aetiology [5] and treatment of BPD [6, 7], parenting issues for adults with BPD have been relatively neglected.
Clinically, mothers with BPD report feeling estranged, anxious, overwhelmed or even angry with their infant from birth [4]. They are often inconsistent in their responses to their child's needs and they have difficulties in accurately interpreting infant affect [8]. Consequently, mothers with BPD are at risk of repeating disturbing and potentially traumatizing interactional patterns with their infant. Despite the potentially significant implications of these disturbed interactions on child development, direct research into describing the relational disturbances of this group is lacking.
To date, only two studies have investigated the interaction patterns of mothers with BPD and their offspring. Crandell et al. compared eight mothers diagnosed with BPD to mothers with no psychiatric disorder [9]. Mothers were video-recorded interacting with their 2-month-old infants using the Still-Face Procedure (SFP) [10]: mothers maintain a still, neutral facial expression and refrain from interacting with their infant and then re-engage their infant and return to natural interaction. In the standard SFP, it is expected that infants will be disturbed by their mother's lack of animation and attempt to re-engage her through vocalizing, gesturing and smiling [11]. However, in that study mothers with BPD were intrusively insensitive during the interaction with their infants, and their infants responded with dazed facial expressions rather than attempting to re-engage their mothers. That study offers preliminary evidence that mothers with BPD have interactional difficulties with their newborn infant.
In a further study, Hobson et al. examined attachment status and interpersonal relatedness in infants of 10 mothers with BPD and 22 non-clinical control mothers [12]. Using the Strange Situation Procedure (SSP), 50% of infants of mothers with BPD were ‘disorganized’, compared to 27% of comparison infants. Mothers with BPD were significantly more intrusive and insensitive than control mothers, and infants of BPD mothers were found to be less available for positive engagement. These infants scored lower on behavioural organization and mood state than control infants, and gave fewer positive looks during observation. Again, that study supports the view that mothers with BPD have difficulties with emotional parenting.
Clearly, research on parenting issues for mothers with BPD requires further study. Patterns of early interaction can be assessed in a number of ways. An alternative approach to the SFP and the SSP is to assess precursors to the development of a secure attachment relationship, such as sensitivity and emotional availability. The Emotional Availability (EA) Scale integrates attachment theory and emotional availability perspectives; assessing a mother's emotional responsiveness and affective attunement to their child's needs and goals, and the child's ‘secure base behaviours’ and affective availability to their parent [13]. Thus, the EA presents an alternative method for assessing the interaction for mothers with BPD with their infants.
In addition to the EA, self-report measures that assess parenting perceptions provide insight into how a mother's sense of self impacts on her parenting skills. Parents who lack a sense of efficacy in their ability to parent do not show persistence in parenting in the face of adversity [14]. Likewise, parents who report being stressed in relation to their parenting role have been shown to have a reduced capacity to parent optimally [15]. Without a positive and emotionally valued sense of self as a parent, affective competence, the parent's capacity to engage empathically with the infant, and their ability to establish patterns of emotionally responsive interaction, can be compromised.
Understanding the interaction patterns and parenting perceptions of parents with BPD is vital for providing appropriate interventions to this high-risk group of parents. Consistent with recommendations for assessing parenting in the literature [16], the present study used both observational and self-report methods in combination to understand the parenting dynamics of mothers with BPD.
Method
Participants
Mothers with BPD (n = 17) were recruited within the Western Sydney Area Health Service. To be eligible for the study, mothers with BPD had to (i) have an independent clinical diagnosis of BPD; (ii) meet DSM-IV criteria for BPD [1]; and (iii) score ≥8 on the Revised Diagnostic Interview for Borderlines (DIB-R; a semi-structured interview that reliably distinguishes BPD from other personality disorders [17]). It should be noted that the DIB-R was available for 11 participants. The first two authors (LN and CS) then reached a consensus agreement on BPD diagnoses. One mother was excluded because she presented with severe dissociative symptomatology precluding completion of the protocol. At the time of the study, no mother was in concurrent treatment (it is estimated that 50–60% had had some prior psychotherapy, albeit none had attended mother–infant therapy).
Control mothers (n = 21) were recruited from the community in Western Sydney. Control mothers had to (i) report no history of mental health problems; and (ii) score <13 on the Edinburgh Postnatal Depression Scale (EPDS [18]). One mother was excluded based on these criteria.
The following criteria also applied to all dyads: (i) infants were full-term and had no developmental delay or known neurological impairment; and (ii) infants were aged between 3 and 36 months. Based on these additional criteria, two mother–infant dyads from the BPD group were excluded. The final sample consisted of 14 mothers diagnosed with BPD and 20 community mothers.
Demographic characteristics of the sample are presented in Table 1. The observed differences in relationship status, education and employment status were consistent with DSM-IV (i.e. broken marriages, interrupted education and recurrent job losses are characteristic of BPD). Importantly, we explored whether the social disadvantage apparent in the BPD group could account for the results reported herein. We calculated a social disadvantage score for each participant by collapsing the following variables: relationship status, level of education, employment status and income. For both groups, we found no significant correlations between socioeconomic disadvantage and parenting observational and self-report results; thus social disadvantage is not an explanation for the findings.
Maternal demographic and infant characteristics
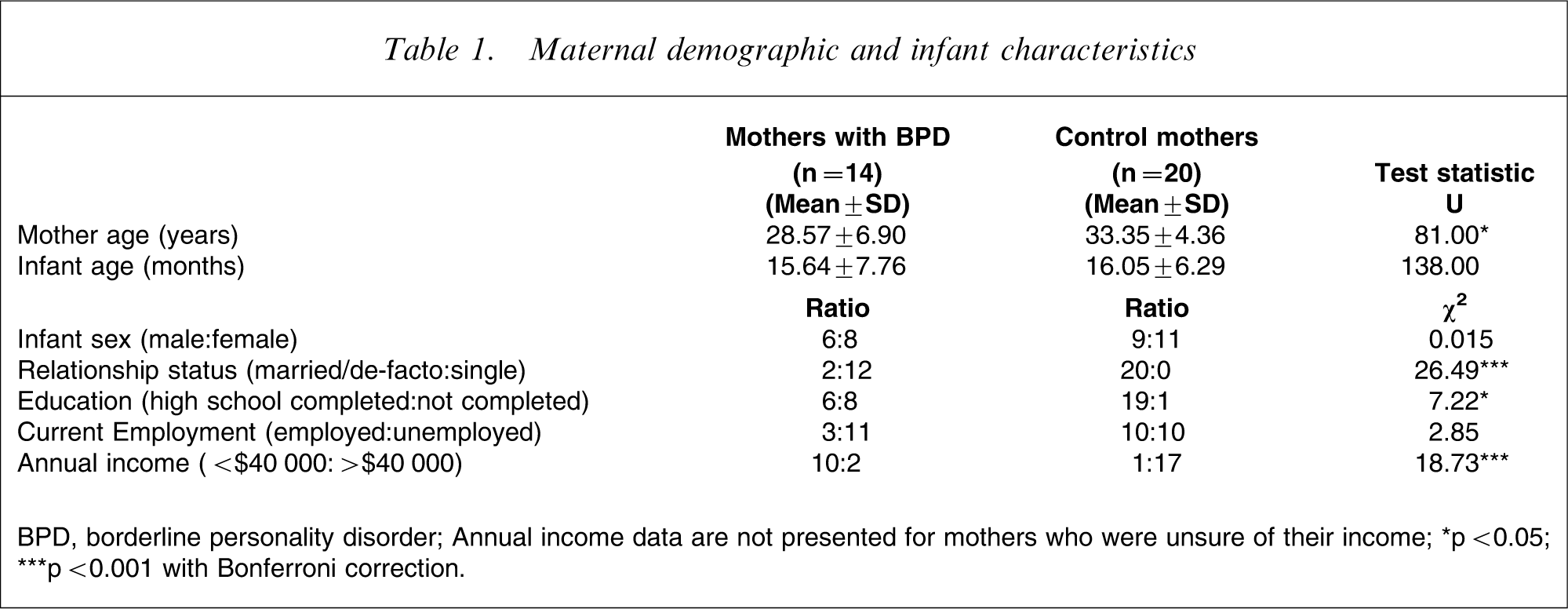
BPD, borderline personality disorder.
Annual income data are not presented for mothers who were unsure of their income.
∗∗p < 0.05; ∗∗p < 0.001 with Bonferroni correction.
Assessment procedure
Dyads attended two assessment sessions. In the first session a brief history was taken and mothers completed the following self-report measures: the EPDS [18] and the Symptom Checklist 90–Revised (SCL-90-R) [19] to assess their mental health; and the Parenting Stress Index–Short Form (PSI-SF) [15] and the Parenting Sense of Competence Scale (PSOC) [20] to assess their perceptions of parenting. In the second session, dyads were video-recorded during 10 min of free play interaction. The interaction was then coded according to the EA guidelines [21] by a reliable, trained and blinded independent coder.
Measures of maternal mental health
The 10-item EPDS screens women for depression after childbirth [18]. The EDPS has demonstrated satisfactory validity and reliability [22]. We used high scores on the EDPS to screen out control mothers experiencing depressive symptoms but did not apply this criterion to mothers with BPD. We felt that excluding these mothers would have produced a biased and unrepresentative sample because affective dysregulation is recognized as a component of BPD; namely, depression in BPD is closely associated with feelings of loneliness and unfulfilled longings for close interpersonal relationships [23].
The SCL-90-R consists of 90 questions and assesses nine domains of general psychopathology: somatization, obsessive–compulsions, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation and psychoticism [19]. The SCL-90-R has been widely validated in many populations and has established psychometric properties, with good internal consistency and high test–retest reliability [24, 25].
Measure of mother–infant interaction
The EA assesses mother–infant interactions along six dimensions of emotional availability: four parent scales (sensitivity, structuring, non-intrusiveness and non-hostility) and two child scales (responsiveness and involvement) [21]. Mothers are rated on their ability to respond appropriately to cues from their child, display appropriate and authentic affect and structure their child's activities, while infants are rated on their response to their parent's interaction both overtly and affectively and their ability to engage their parent during interaction. The psychometric properties of the EA are established [26]. The non-intrusiveness scale was not used because this scale does not distinguish between parents who actively allow their child to lead the interaction, from parents who are neglectful, withdrawn or passive and disengaged.
Measures of parenting perceptions and stress
The PSOC consists of 16 questions and assesses parental competence on two subscales: satisfaction and efficacy [20]. Both subscales have good internal consistency [27].
The PSI-SF contains 36 questions and assesses three dimensions of parenting stress: parental distress, parent–child dysfunctional interaction and child difficulty [15]. These dimensions sum to a total stress score. The PSI-SF scales have demonstrated high internal consistency and adequate test–retest reliability [15].
Data analysis
Data were analysed using SPSS for Windows version 13.0 (SPSS Inc., Chicago, IL, USA). Parametric and non-parametric tests were conducted as appropriate, with a Bonferroni correction applied to each family of comparisons. We used one-tailed tests of significance because we were predicting that mothers with BPD would have more mental health problems, more difficulties interacting with their infant and report less satisfaction, less competency and more distress in their parenting role.
Results
Mothers’ mental health
Mothers with BPD scored higher on the EPDS (mean = 13.00, SD = 4.97) than control mothers (mean = 4.25, SD = 2.75), t(18) = 5.97, indicating greater psychological distress. As can be seen in Table 2, statistically significant differences were found between the two groups on all SCL-90-R subscales, with mothers with BPD scoring higher on all indexes of psychopathology. These results are consistent with identifiable BPD symptomatology because mothers scored highly on the SCL-90-R impulsivity, affective and cognitive domains [28].
Maternal mental health
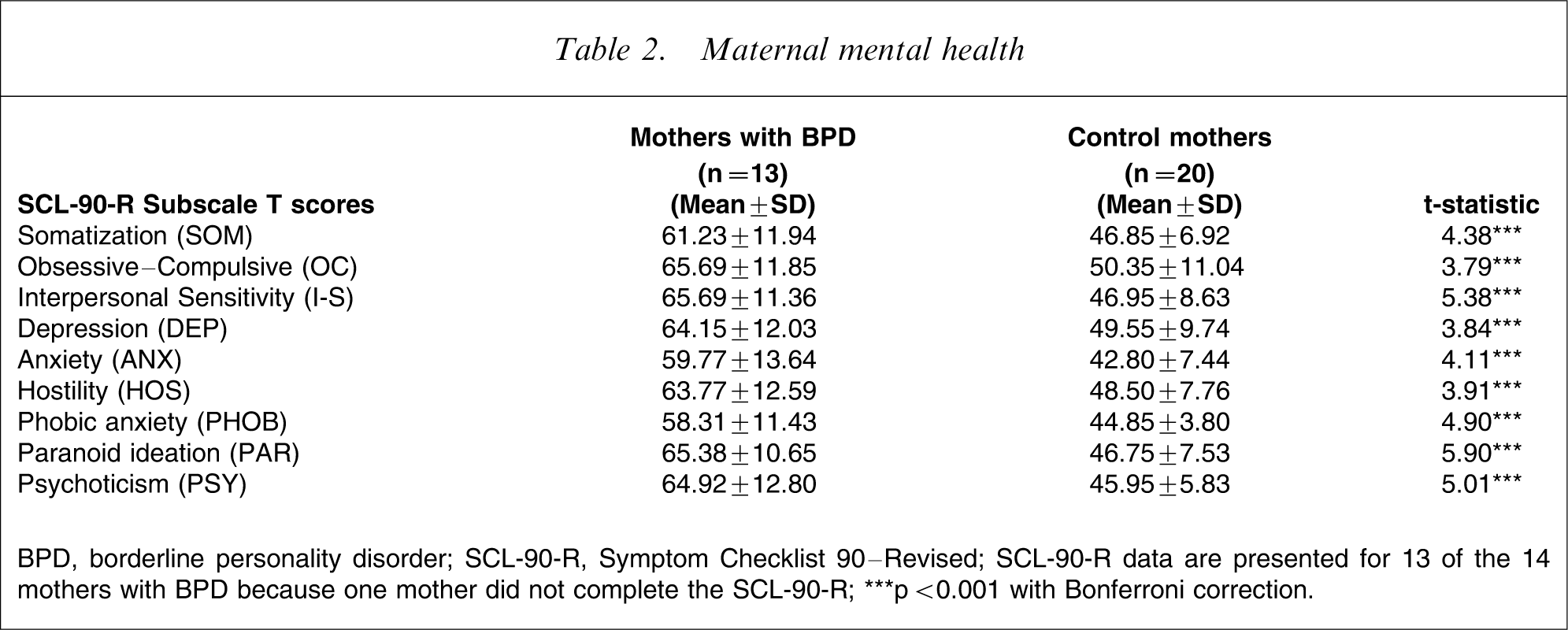
BPD, borderline personality disorder; SCL-90-R, Symptom Checklist 90–Revised.
SCL-90-R data are presented for 13 of the 14 mothers with BPD because one mother did not complete the SCL-90-R.
∗∗∗p < 0.001 with Bonferroni correction.
Comparison of mother and infant interaction styles on the EA
As can be seen in Table 3, statistically significant differences were found between the two groups on two of the three parent scales of the EA (sensitivity and structuring) and both child scales (responsiveness and involvement). An inspection of the data revealed the following:
Descriptive statistics for mothers’ and infants’ interaction styles on the EA
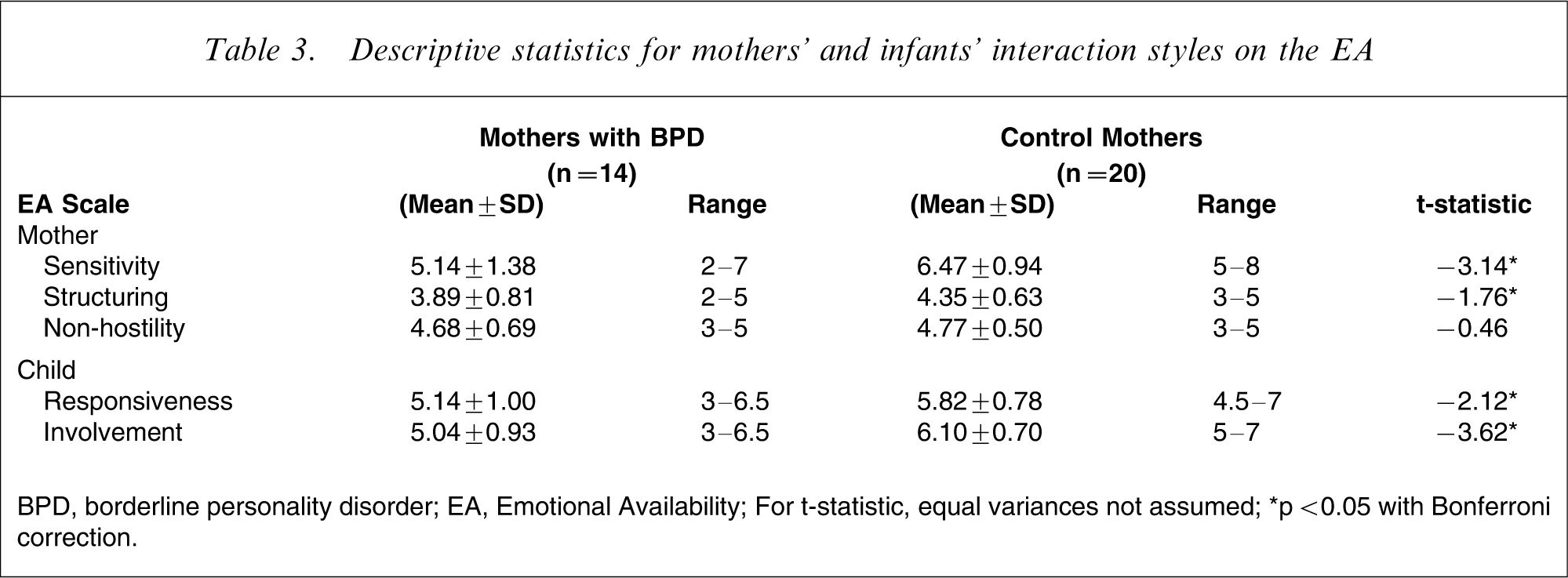
BPD, borderline personality disorder; EA, Emotional Availability.
For t-statistic, equal variances not assumed.
∗p < 0.05 with Bonferroni correction.
Sensitivity scale
Most mothers with BPD (64.3%; n = 9) were rated as ‘inconsistently sensitive’, ‘somewhat insensitive’ or ‘highly insensitive’ in comparison to the majority of control mothers (80%; n = 16) who were rated as either ‘highly’ or ‘generally’ sensitive.
Structuring scale
Five mothers with BPD (35.7%) were rated as either ‘inconsistent’ or ‘non-optimal’ in their attempts at structuring their infant's activities compared to three control mothers (15%) who received a (lowest) rating of ‘inconsistent’.
Non-hostility scale
Three mothers with BPD (21.4%) were rated as displaying ‘slight’ to ‘covert hostility’ toward their infant compared to two control mothers (10%) who received such ratings.
Child responsiveness scale
Three infants of mothers with BPD (21.4%) were rated as ‘somewhat non-optimal’ in their response to their mother's bids for interaction compared to only one control infant (5%). Additionally, it is noteworthy that no infant of a mother with BPD was rated as ‘optimally responsive’ (c.f. 11 control mothers’ infants; 55%).
Child involvement scale
Ten infants of mothers with BPD (71.4%) were rated as displaying ‘moderately optimal’ to ‘somewhat non-optimal’ involving behaviours toward their mother compared to four infants of control mothers (20%) whose behaviours received a (lowest) rating of ‘moderately optimal’. Additionally, no infant of a mother with BPD was rated as displaying ‘optimally involving’ behaviour (c.f. 16 control mothers’ infants; 80%).
Mothers’ self-perceptions of parenting and parental stress
As can be seen in Table 4, statistically significant differences were found between the two groups on the two subscales of the PSOC (satisfaction and efficacy) and three scales of the PSI-SF (parental distress, parent–child dysfunctional interaction and total stress). These results indicate that mothers with BPD perceive themselves to be less satisfied and less competent as parents, experience more difficulties in coping with their parenting role, feel less satisfied during and disappointed with their interaction with their infant, and experience significant stress. It is notable that three mothers with BPD (21.4%) scored above the 95th percentile on the PSI-SF parent–child dysfunctional interaction scale, while no control mothers scored in this range. According to Abidin, these high scores suggest the potential for child abuse in the form of neglect, rejection or episodes of physical abuse triggered by frustration [15]. Likewise, all mothers with BPD had scores approaching or above the 90th percentile on the PSI-SF total stress scale, while no control mothers scored in this range. This indicates that these mothers are experiencing clinically significant levels of stress in their parenting role.
Parenting perceptions
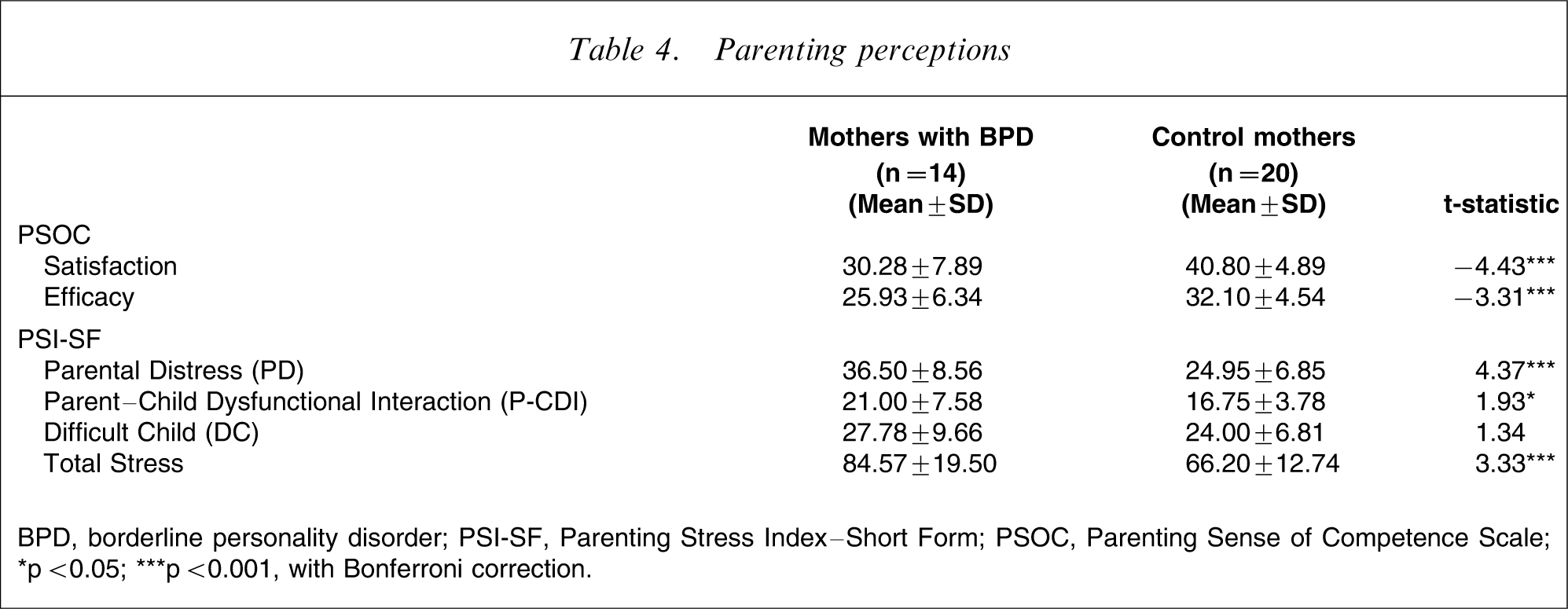
BPD, borderline personality disorder; PSI-SF, Parenting Stress Index–Short Form; PSOC, Parenting Sense of Competence Scale.
∗p < 0.05; ∗∗∗p < 0.001, with Bonferroni correction.
Trends in parenting indexed by observational and self-report measures
As can be seen in Table 5, correlations were conducted to establish the relationship between measures of parenting. Two observations are noteworthy. First, there is a relationship between increased parental distress (on the PSI-SF) and increased feelings of dissatisfaction and incompetence in parenting (on the PSOC). Second, parents who express more parental distress (PSI-SF) are less sensitive in parenting (EA).
Zero-order correlations among maternal observational and self-report indices
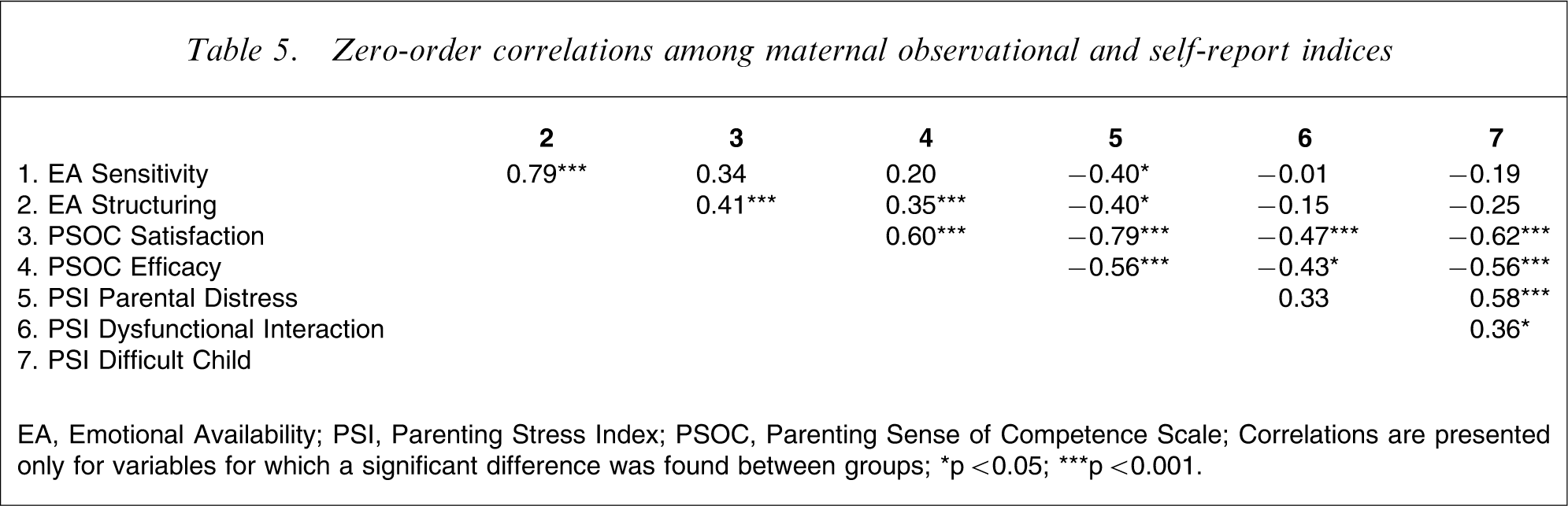
EA, Emotional Availability; PSI, Parenting Stress Index; PSOC, Parenting Sense of Competence Scale.
Correlations are presented only for variables for which a significant difference was found between groups.
∗p < 0.05; ∗∗p < 0.001.
Discussion
The present study examined the parenting attributes of mothers with BPD by assessing their interaction with their infant and their parenting perceptions. When compared to community controls, mothers with BPD were found to be less sensitive in their interaction with their infants and to be less effective in structuring their infant's activities. Moreover, the infants of mothers with BPD were less responsive to the mother's attempts at interaction and less willing or eager to engage their mother. On self-report measures, mothers with BPD reported dissatisfaction and incompetence in their parenting role and were more distressed than mothers from the community.
This research replicates existing research [9, 12] by demonstrating similar patterns of interactions albeit with a different measurement (the EA) and in an older age group of infants. Further, it extends the literature by reporting on the largest sample of mothers with BPD to date and by providing a more comprehensive overview of the parenting difficulties experienced.
These results support the long-held view of clinicians that mothers with BPD have significant problems with parenting. Parental sensitivity is considered a precursor to a secure attachment and a child's emotional and social development [21]. Parental structuring provides the necessary framework for interaction and the encouragement of a child's self-regulatory attempts [21]. Thus, the lack of parental sensitivity and poor structuring of mothers with BPD is of major concern when child outcome is considered. In addition, the infants of mothers with BPD do not orientate their behaviours toward their mother, appear disinterested in engaging their mother in interaction and are less responsive to the mother's bids for interaction. These findings indicate that the infants of mothers with BPD are withdrawing from social activities with their parents. The long-term consequences of this behaviour are that the infants of mothers with BPD could be developing avoidant patterns of interpersonal relatedness.
It was surprising that no significance difference was found between mothers with BPD and control mothers on the EA non-hostility scale. One explanation, which is consistent with the present sample of mothers, is that mothers with histories of trauma can either be ‘frightening to’ or ‘frightened of’ their infants [28]. In the present sample, rather than being actively hostile and displaying frightening or threatening behaviours, most mothers with BPD appeared ‘frightened of’ and withdrawn from their children. With a larger sample size, it is possible that more active hostility would be observed in mothers with BPD.
A strength of the present study was the combined use of observational and self-report measures. Self-report measures can tap into the ideas that parents have about themselves as parents, an important concept to consider when working with adults with BPD. Compared to control mothers, mothers with BPD perceived themselves to be less satisfied and less competent. The lower satisfaction scores of mothers with BPD suggest that they are more frustrated, anxious and unmotivated in their parenting role, while their lower efficacy scores imply that they perceive themselves to be less competent or capable as parents. These findings are concerning given that parents with low-self efficacy have been found to feel overburdened by their parental duties and as a result frequently become immobilized by the emotional and physical tasks involved [15]. The implication of this is that children of these parents are at greater risk of abuse or neglect.
In addition to rating themselves poorly as mothers, mothers with BPD reported higher levels of stress and, consistent with other studies [29], we found that high stress correlated with low self-efficacy. On the PSI-SF, mothers with BPD rated their role as a parent as stressful and their interaction with their child as stressful. High self-perceptions of stress in the parenting role are believed to have an adverse effect on the mother–infant relationship and the capacity to parent optimally. Moreover, high levels of parenting stress are associated with a negative authoritarian parenting style. This style of parenting has been associated with disruptive and later oppositional behaviour in children [15]. Thus the parenting style of mothers with BPD is likely to have an adverse outcome on child development and behavioural regulation.
A limitation of the present study was the use of community group for comparison rather than a group with another diagnosis (i.e. depression or personality disorder); but it was beyond the scope of this preliminary study to include such a group. Thus we acknowledge that depression in the BPD group may have contributed to the observed outcomes. In addition, the present study used a cross-sectional design to gain an understanding of the types of parenting challenges experienced by mothers with BPD. The next step would be to conduct a longitudinal study to explore the long-term impact of having a parent with BPD, for child outcome. Interestingly, Rutter and Quinton in the 1980s predicted that mothers with personality disorders would have more challenges with parenting than those mothers with Axis 1 conditions [30] and yet this area of research has been neglected.
Conclusions
The present study provides significant insight into and furthers understanding of the impact of BPD on parenting. Overall, our results indicate that the parenting role for mothers with BPD is challenging and stressful and as a consequence their interactions with their infant lack emotional responsivity and structure. Likewise, their children showed early signs in interaction that they are likely to be socially and emotionally developmentally disadvantaged. Observational and self-report methods provided insight into how the maternal state of mind directly influenced parenting behaviours (observed emotional interactions) and cognitive representations (perceptions of the self as a parent). Importantly, despite 50–60% of the present BPD sample having had prior psychotherapy, a clear implication of the present study is that mothers with BPD need to be identified early, with intervention targeted at that interaction with their infant and their self-perceptions of parenting. Currently, the authors are developing such an intervention programme known as ‘Getting to know you’ [31]. This programme uses video examples to support mothers with newborn babies to interpret and respond to their baby's early attempts at communication. Such intervention may protect their infants from social and emotional difficulties later in life. Clearly, further research is needed to identify and understand the parenting difficulties of mothers with BPD that directly impact on their children's developmental outcomes.
Footnotes
Acknowledgements
The present study forms part of a series of studies into mothers with BPD and their infants. We would like to thank the all the mothers and infants who volunteered to participate. We are also grateful to Sophie Rabone and Rochelle Dempsey for assisting with data collection.