
Abstract
Keywords
Post-traumatic stress disorder (PTSD) is a disabling and chronic condition [1, 2]. Because many sufferers remain symptomatic following treatment [3, 4] it is important to investigate predictors of outcome following psychological therapy. To date, research on PTSD has identified few factors that predict treatment outcome. Pre-treatment symptom severity is most consistently found to do so, generally accounting for 20–25% of the variance [4–6]. Comorbid conditions, such as anger, depression, anxiety, guilt, and disorders of extreme stress not otherwise specified, account for additional variance [7, 8]. Variables from the transtheoretical model of behaviour change (TTM) [9] have predicted treatment outcome more accurately than symptom severity for a range of problems (such as panic disorder and obesity) and settings (such as psychiatric outpatient clinics) [10–12]. Because constructs from the TTM can be directly influenced by psychological therapy [13], additional treatment components could be incorporated into current programmes if these constructs are found to influence outcome.
According to the TTM, people occupy different stages of readiness to change (operationalized as a categorical variable and termed ‘stage of change’; SOC) and use different strategies to overcome their problem(s) (‘processes of change’; POC). Readiness to change has also been conceptualized as a continuous variable (as used by Carey et al.[14] and hereafter designated by RTC-C). The TTM proposes that behaviour change involves progression through five SOCs: pre-contemplation (not considering change in the near future); contemplation (thinking about changing); preparation (deciding to change and beginning to make small changes); action (actively changing); and maintenance (preventing relapse and consolidating gains) [9]. There has been little examination of the predictive utility of SOC in PTSD populations, perhaps because ambivalence to change has normally been associated with addictive disorders. However, ambivalence may be relevant to PTSD that is characterized by avoidance, and whose treatment requires exposure to distressing memories and situations. In fact, Murphy et al. state that combat veterans are ‘often ambivalent about changing not only common problems associated with PTSD such as substance abuse, but also the symptoms of PTSD themselves’ [15]. In the only study that has examined this area, SOC was predictive of outcome for people receiving treatment for PTSD and/or a substance use disorder [16]. Those participants classified as being in pre-contemplation or contemplation had double the likelihood of relapse when compared to those in action or maintenance (48% vs 22%). However, the analysis did not differentiate between relapse of PTSD and substance use disorder.
As with the two readiness-to-change measures (SOC and RTC-C), the predictive utility of the different strategies that individuals use to bring about change (process of change POC) has not been examined in a PTSD population. Each process is a group of techniques, methods or interventions carried out by the person to alter their own affect, thinking and behaviour [9]. The 10 POCs that have received the most empirical support have been categorized into two factors: cognitive/experiential and behavioural [17]. Examples of cognitive/experiential processes of change include learning about the causes and consequences of behaviour, challenging beliefs and expectations about behaviour, or assessing the impact of behaviour on others. Examples of behavioural processes of change include restructuring the environment to reduce the occurrence of behaviour, self-rewarding positive behaviours, or actively seeking the support of others. POC factors measured midway through treatment have been found to predict outcome better than SOC, self-efficacy, social support, and demographic variables [12].
The present study examines the predictive utility of TTM variables in a PTSD veteran population. A previous study using this same population found that although the TTM constructs appeared to be internally consistent, many of the predicted relationships between the TTM variables were not found [18]. For example, contrary to the model, changes over time in assigned SOC and RTC-C were not related to POC. The results of this research led to the tentative conclusion that TTM variables may be operating in unique ways in a veteran PTSD population. Despite these results TTM constructs might still assist with prediction of outcome. Our first hypothesis is that SOC, RTC-C, behavioural processes and cognitive/experiential processes, when measured prior to treatment, will predict follow-up symptom severity, while controlling for baseline severity. Our second hypothesis is that changes in these variables across treatment and follow up will be associated with changes in symptom severity across the same time frame.
Method
Participants
Fifty of 53 male veterans in six out of seven consecutive preparation programmes for outpatient PTSD treatment in Australia consented to participate in the research. All participants (aged 45–72 years) lived in rural areas. The inclusion criteria for the preparation programme and thus the study required that the participant have a primary diagnosis of DSM-IV PTSD as a result of military service, as elicited by the Clinician-Administered PTSD Scale (CAPS) [19]. Participants were not excluded on the basis of comorbidity, medication usage, or prior treatment history. All participants had received some treatment prior to commencement, with most having been prescribed antidepressant medication. Some participants had received supportive counselling from the Vietnam Veterans Counselling Service, but none had received specific psychological intervention for PTSD.
Procedure
Following referral to the programme, assessment included a clinical interview with a psychiatrist, followed by a psychosocial and CAPS assessment administered by a psychologist. Three clinical psychologists and three intern clinical psychologists were involved in the preparation and treatment programmes. Each programme was conducted with a closed-group cohort of between five and 13 veterans. Veterans first completed a preparation programme over 2 consecutive days. This programme involved an introduction to the group; discussion of the nature of PTSD and commonly associated psychological problems; introduction to the SOCs; review of other services available; and discussion of the treatment programme offered. Veterans were approached immediately prior to the preparation programme and asked if they were willing to participate in the study and, on agreement, completed the first questionnaire packet.
One week after completing the preparation programme participants started the 14 week manual-based cognitive behavioural therapy treatment group outpatient programme [20], attending 2 days a week. One day review and booster sessions were held at 3 months and 9 months after treatment. Treatment consisted of psychoeducation, arousal reduction and other symptom management techniques, interpersonal problem-solving, communication skills, exercise therapy, sleep hygiene, exposure, cognitive restructuring, and relapse prevention. The exposure was primarily in vivo during the group sessions, with some nightmare rescripting. Imaginal exposure was offered during individual sessions (which also involved goal setting and discharge planning), as well as after completion of the treatment programme. Two or three family days were provided to give education and support to family members.
The measurement occasions were (i) before treatment (prior to preparation programme); (ii) 3 weeks into the treatment programme (subsequently labelled ‘early in treatment’); (iii) after treatment; and (iv) at 3 month follow up. The variables assessed on each occasion were symptom severity, RTC and processes.
Measures
The Clinician Administered PTSD Scale-Current Diagnosis version (CAPS-DX) is a diagnostic interview for PTSD that also provides a severity/frequency measure of symptomatology [19]. It has demonstrated good convergent validity with the Mississippi Scale for Combat-Related PTSD (r = 0.91) in a veteran population [21]. The Combat Exposure Scale (CES) consists of seven items and measures the severity of wartime experiences [22]. Other traumatic events were assessed using the Life Trauma Questionnaire (LTQ) [23], which was designed for the National Comorbidity Study [1] to assess traumas as defined by DSM-III-R.
Outcome was assessed by changes across treatment in self-reported severity of PTSD and comorbid symptoms. The PTSD Checklist–Military version (PCL) is a 17-item checklist derived from the DSM-IV criteria providing a continuous measure of PTSD severity [21]. The test–retest reliability was found to be 0.96 using a sample of male Vietnam-theatre veterans, internal consistency ranged from 0.89 to 0.92 for the three PTSD symptom clusters, and validity was supported by a kappa of 0.64 assessed against diagnosis from the Structured Clinical Interview for DSM (SCID) [21]. The 14-item Hospital Anxiety and Depression Scale (HADS) [24], which omits physical indicators of psychological distress, was used to assess anxiety and depression. It has acceptable internal consistency (Cronbach α between 0.80 and 0.93 for the subscales) and validity [25]. The General Health Questionnaire (GHQ-28) is a 28-item instrument that is a general index of psychological well-being [26]. The Likert scoring method was chosen, which has a sensitivity of 79.8% and specificity of 78.5% [27].
The University of Rhode Island Change Assessment Scale (URICA) assessed both the categorical and continuous measures of readiness to change (SOC and RTC-C, respectively) [28]. The URICA consists of 32 items and four subscales (pre-contemplation, contemplation, action, and maintenance). The URICA has been found to have high internal consistency [11] and its factorial validity has been supported across a variety of outpatient settings [11, 28]. The Process of Change Questionnaire (POCQ), which measures the use of 10 processes of change, was based on the Bellis 25-item version of the instrument, which has demonstrated good factor loadings, with a median factor loading of 0.76 [29]. Respondents are asked to indicate how frequently they engage in each activity on a 5-point Likert scale. We excluded three items assessing substance use, which is behaviour specifically unhelpful in PTSD and therefore could not be viewed as a process that would contribute to positive change in the present sample. For a similar reason, we replaced the stimulus control item ‘I avoid situations associated with my problems’ with ‘I avoid people who add to my problems’. Eight extra items were added to ensure there were three items for each of the processes, selecting the additional items on the basis of those that most highly loaded on the relevant POC factors from the Bellis [29] 72-item version, bringing the questionnaire to 30 items in total. The POCQ provides two factors scores. One factor assesses behavioural processes of change (e.g. ‘I reward myself when I don't give in to my problems’) and one factor assesses cognitive/experiential processes of change (e.g. ‘When I begin to experience my problems, I try to get in touch with what I am feeling’). In the current sample the POCQ scale had good internal consistency, with Cronbach's alpha ranging from 0.87 to 0.94 over the four time-points. Furthermore, a principal components analysis using scores across all time-points produced two components that were consistent with the cognitive/experiential and behavioural factors.
Statistical analyses
A principal components analysis of the symptom measures administered at each time-point (PCL, GHQ and HADS) indicated that they load onto one factor that accounted for 79% of the variance. Because the principal component weightings were similar (0.92 for the HADS, 0.86 for the GHQ and 0.89 for the PCL), one general symptom severity measure was computed by taking the mean of the scores on these measures.
Participants were allocated either to the contemplation (thinking about changing) or the combined preparation, action and maintenance (‘decided to change’) SOC group on the basis of their highest URICA subscale score. The formation of only two SOC groups was necessary given the low number of participants in the preparation (n = 4, 4, 2, 3), action (n = 7, 1, 2, 5), and maintenance (n = 4, 3, 4, 5) SOCs across the four time-points, respectively. Because only two participants were in the pre-contemplation SOC, and only at one time-point each (before treatment and early in treatment), their SOC at these times was not included in the analyses. The RTC-C score (possible range: −16 to 112) was computed by subtracting the score on the pre-contemplation subscale from the sum of the remaining scores [14].
Multiple regression analysis (SPSS Windows version 11.0; SPSS Inc., Chicago, IL, USA) was used for the prediction of symptom severity at follow up using data from the pre-treatment and the early-in-treatment assessment point (hypothesis 1). For each set of analyses, pre-treatment symptom severity was entered as a covariate and each independent variable (cognitive/experiential process usage, behavioural process usage, RTC-C and assigned SOC) was examined separately for its predictive utility. Mixed-effects regression analysis was used for the regression analyses examining the relationship between changes in each independent variable and symptom severity over time (hypothesis 2; (MIXREG Windows version 1.2) [30]. This approach has the advantage of allowing retention of cases with partially missing data. The time (weeks) variable was transformed (loge (week +1)) to make it more linear and was entered as a fixed effect. Each independent variable was examined in a separate regression analysis, and those found to have a significant interaction with time were then included in a full model. The independent contribution of each variable within this full model was determined by removing each variable in turn and comparing the log-likelihood of the reduced model with that of the full model. A final reduced model included only those variables that made a significant independent contribution. A likelihood ratio test was then conducted to determine whether the final model had a better fit than one using the intercept only. Finally, McFadden's ρ2 (a pseudo R2) was calculated for the final reduced model.
Results
Characteristics of the sample
Table 1 presents baseline information on participants who began the treatment programme. At assessment participants had severe levels of PTSD symptoms, which had existed for many years. Symptom severity at assessment was reflected in a mean CAPS score of 88.8 (SD = 17.5), which is well above the accepted diagnostic cut-off of 50, and comparable to other PTSD samples such as that described by Forbes et al. (mean = 81.84, SD = 16.86) [7]. The level of combat exposure experienced by participants, as assessed by the CES, was moderate, similar to the mean score (19.27) for Australian veterans seeking help from the Vietnam Veterans Counselling Service [31].
Subject characteristics at initial assessment
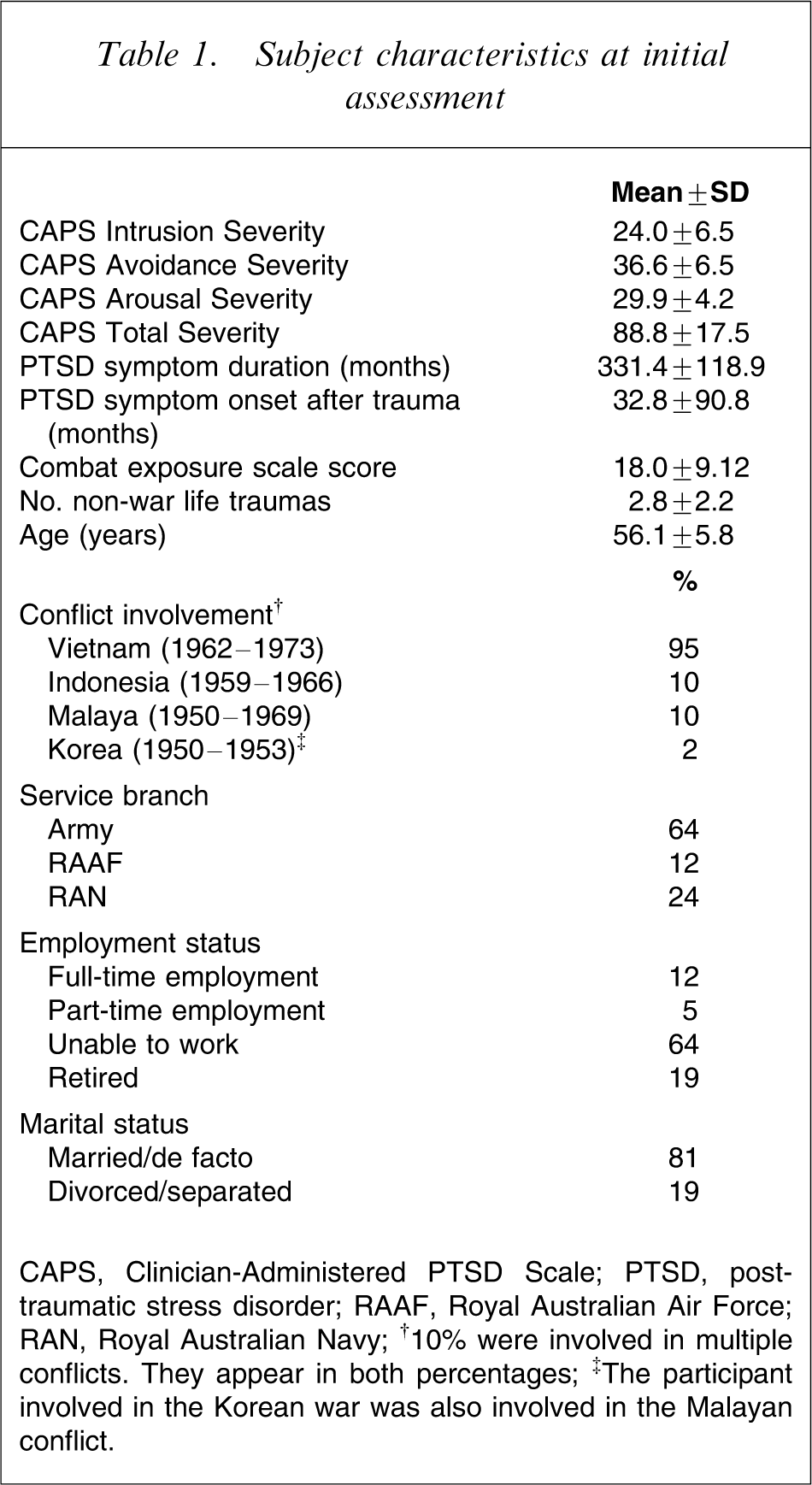
CAPS, Clinician-Administered PTSD Scale; PTSD, post-traumatic stress disorder; RAAF, Royal Australian Air Force; RAN, Royal Australian Navy.
†10% were involved in multiple conflicts. They appear in both percentages.
‡The participant involved in the Korean war was also involved in the Malayan conflict.
Table 2 shows scores on the outcome and TTM measures at each measurement time-point. The treatment effect size for the total PCL scores between pre-treatment and 3 month follow-up assessments was 0.74. This treatment effect compares favourably with the treatment effect reported by Creamer et al. between admission and 3 month follow up (0.58) [3]. Data were not complete at all time-points, primarily due to incomplete or misplaced questionnaires, or participants being absent at the collection points. Two participants withdrew from the study during the preparation programme, 10 participants who attended at least part of the preparation programme did not start treatment, and three dropped out of treatment. No differences were found for scores at pre-treatment or early in treatment assessment on the independent variables and symptom severity measures of participants (i) with and without end-of-treatment data, and (ii) with and without 3 month follow-up data.
Measures of symptoms and TTM variables
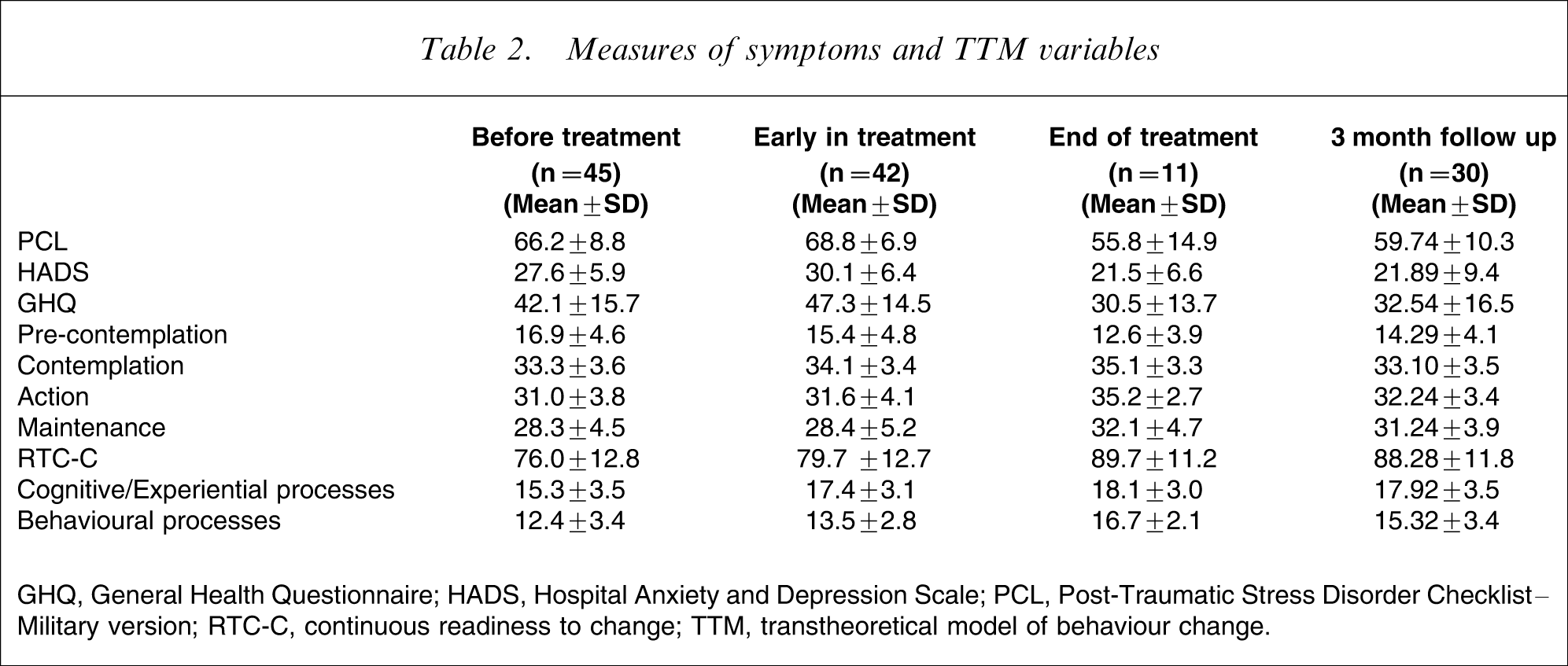
GHQ, General Health Questionnaire; HADS, Hospital Anxiety and Depression Scale; PCL, Post-Traumatic Stress Disorder Checklist–Military version; RTC-C, continuous readiness to change; TTM, transtheoretical model of behaviour change.
Prediction of changes in symptom severity
Assigned SOC was the only variable measured at the pre-treatment assessment that was predictive of 3 month follow-up symptom severity when pre-treatment symptom severity was entered as a covariate (R2=0.15, p < 0.05). When entered alone, pre-treatment symptom severity did not account for a significant amount of the variance in symptom severity at the 3 month follow up (R2=0.05, p = 0.14). No variable measured at the early-in-treatment time-point was predictive of 3 month follow-up symptom severity status when initial symptom severity was entered as a covariate.
Prediction of change in symptom severity and TTM variables over time
Mixed-effects regression analyses for each independent variable were conducted separately to determine the relationship between changes in symptom severity over time and changes in each of the TTM variables. There was no significant relationship between pre-treatment symptom severity and SOC (z = − 0.73, p = 0.46) or cognitive/experiential processes (z = 1.88, p = 0.06). Likewise, there was no significant relationship between changes in symptom severity over time and changes in SOC (z = − 0.46, p = 0.65) or cognitive/experiential processes (z = − 0.67, p = 0.51). Although participants with different RTC-C scores did not have significantly different pre-treatment symptom severity scores (z = 1.21, p = 0.23), there was a significant relationship between changes in symptom severity over time and changes in RTC-C (z = − 2.17, p ≤ 0.05). In other words, those participants who reported greater increases in RTC-C over time also reported a greater lessening in symptoms over time. Participants with different behavioural process usage were significantly different in terms of reported pre-treatment symptom severity (z = 2.06, p < 0.05). Furthermore, there were also differential decreases in symptom severity over time associated with changes in behavioural process usage (z = − 4.59, p ≤ 0.001). Given that RTC-C and behavioural process usage were the only variables significant in the separate analyses, a model was created using these variables (Table 3). A comparison of log-likelihood ratios showed that this model (with time, RTC-C, behavioural processes, the interaction of these two variables with time, and a random intercept) had a significantly better fit than a random intercept alone (Table 4; χ2 (df = 5) = 200.25, p < 0.001). The removal of either behavioural processes or RTC-C led to degradation in the model (χ2 (df = 2) = 43.61, p < 0.001, and χ2 (df = 2) = 63.68, p < 0.001, respectively). The McFadden's ρ2 for the model was 0.21. Given that it tends to be an underestimate of the correlation, such a value is considered highly satisfactory [32].
Changes in symptom severity over time as a function of changes in total RTC and behavioural processes of change
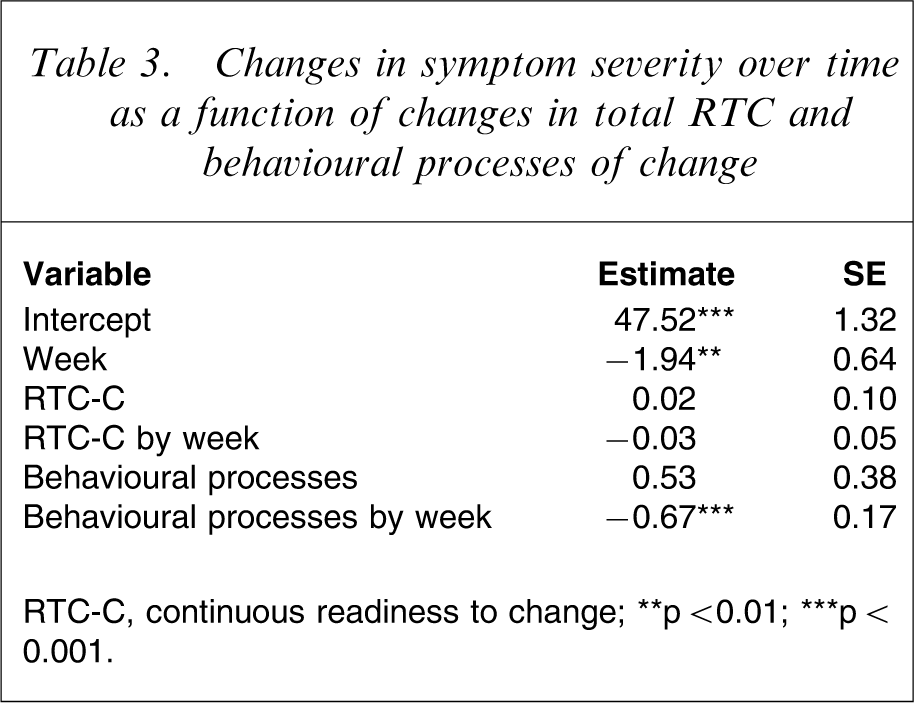
RTC-C, continuous readiness to change.
∗∗p < 0.01; ∗∗∗p < 0.001.
Model fitting information for symptom severity
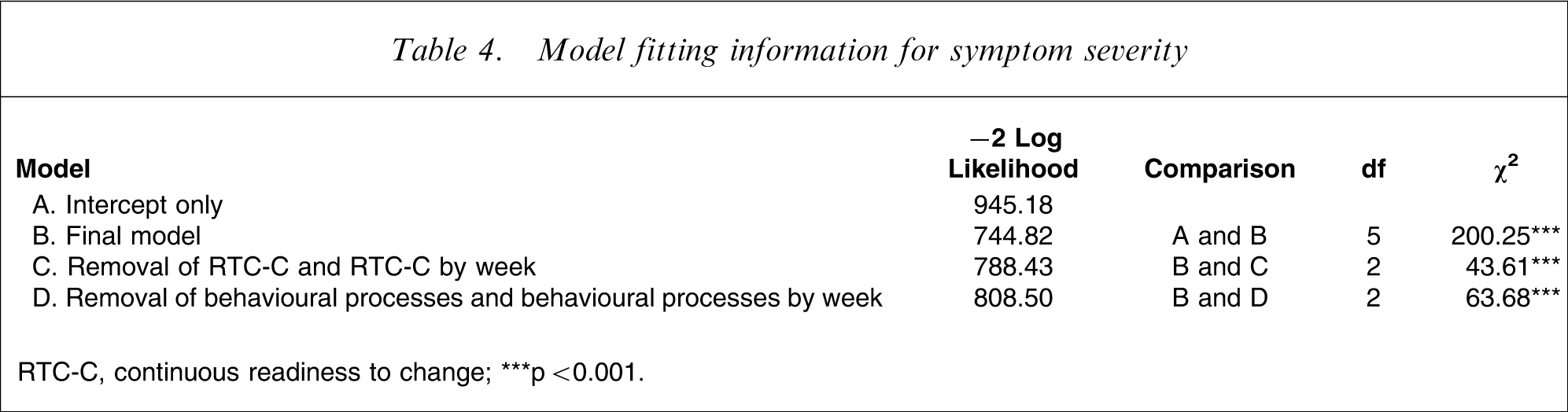
RTC-C, continuous readiness to change.
∗∗∗p < 0.001.
Discussion
The major aim of the present study was to determine whether variables measuring constructs of the TTM, measured both at specific time-points early in treatment and across time, significantly predict symptom severity following treatment. It is recognized that TTM may not be an ideal model of change for PTSD. For example the disadvantages of engaging in therapy for people with PTSD (such as the prospect of having to face triggers of anxiety) may differ in nature from those associated with an addictive or eating disorder (such as having to give up a desired substance or behaviour). Furthermore, PTSD is a complex disorder and its treatment targets a relatively large number of behaviours, each of which might be under different stages of change across treatment. Veterans may enter treatment not to directly resolve their PTSD, but to save their relationships, because of destructive anger or other peripheral reasons. However, variables from the TTM have been found to predict outcome from psychological therapy for a variety of disorders and, as with other populations, knowledge of the characteristics that predict outcome may lead to improvements in the effectiveness of treatment.
Surprisingly, of all the TTM variables assessed prior to treatment only assigned SOC was predictive of improvements in symptom severity over treatment and follow up. This result suggests that those people who were ready to change, or actively involved in change prior to starting treatment, benefited more from treatment than those people only considering change. Changes in RTC-C and behavioural processes over time, but not changes in assigned SOC, were predictive of changes in symptom severity over time. The SOC construct may have had reduced applicability in the current sample because participants generally scored highly across each of the contemplation, action, and maintenance SOC scales [18]. Therefore, participants may not have been in distinct SOCs, but rather, in several SOCs concurrently for different behaviours. Participants may have considered multiple behaviours when completing the URICA (because participants were asked these questions with regard to PTSD as opposed to specific symptoms such as anger), and the continuous RTC-C score may well have been more sensitive to change than assigned SOC per se. RTC-C is particularly sensitive to changes in pre-contemplation, which has been suggested to be important in predicting treatment outcome [33].
In summary, veterans who start treatment actively contemplating change and who increase RTC across treatment have better outcomes. These findings are consistent with some of the predictors found in recent studies. For example, increased levels of comorbid anger may interfere with engagement in treatment and is consistent with an external sense of responsibility and blame [7], both constructs being incompatible with RTC. In another example, non-responders in the Tarrier et al. treatment trial reported treatment to be less credible, were seen as less motivated and attended fewer sessions [34]. Again, the RTC construct may well reflect these general motivational factors. Behavioural, but not cognitive/experiential, process usage was also found to predict outcome. Cognitive/experiential processes have been found to be stable across SOC (excluding pre-contemplators) in trauma patients [18], thus suggesting that usage is independent of whether or not people describe themselves as actively changing or trying to change. In addition, it is possible that combining cognitive and affective processes may have diluted their predictive utility. Research on the association between coping style and PTSD symptomatology suggests that emotion-focused strategies are not helpful [16, 35].
The naturalistic nature of this study affords both benefits and limitations. On the one hand, the results of such research may transfer more readily to clinical practice. On the other hand, participants in one treatment group were not asked to participate in the study due to a concern by the clinical team that a number of group members were at high risk of dropping out of treatment and that the completion of the research assessment would have heightened this risk. It is interesting to note that this group did in fact undertake a truncated version of the treatment programme due to low motivation. Had they been included in the present study the number of participants in the pre-contemplation SOC may have increased, with consequent improvement in the prediction of changes in symptom severity. The data collected in the present study were limited to one outpatient group treatment programme, conducted in various regional settings with male combat veterans whose trauma occurred more than 30 years prior to this treatment. It is also worth considering that participants who had voluntarily entered into an intensive treatment programme that required separate assessments by a psychiatrist and a clinical psychologist may have almost by definition moved on from a pre-contemplation SOC. Thus, the results may not generalize to different samples. Initial symptom severity was not a significant predictor of symptom severity at follow up, unlike the results of most previous research [4–6]. This suggests that the present sample may have been anomalous and thus it may be useful to replicate the study across a range of trauma populations, including those with recent-onset PTSD. The significance of the findings, and the extent and the nature of the analyses conducted, were also limited by the low subject numbers, particularly at the end-of-treatment time-point. Ten of the original 50 participants did not complete any treatment, resulting in the sample size providing sufficient power to detect only a large effect size (R2=0.35) [36]. Furthermore, the small numbers precluded analysis of potentially interesting subgroups, such as individual SOCs.
Notwithstanding these difficulties, the present study is the first to the authors’ knowledge to consider the predictive utility of TTM constructs in a veteran sample by assessing changes in variables over time. In summary, increases in RTC-C and behavioural processes were associated with decreasing symptom severity over time. In terms of the predictive utility of TTM variables at specific points in time, we found that only initial SOC was predictive of change in symptom scores over treatment and follow up. A possible viewpoint, in light of the results of Rooney et al.[18], is that the use of categorical stages of change has limitations in a multifaceted disorder such as PTSD. We must also acknowledge a possible cohort effect, in which the TTM variables were strongly influenced by peers attending the same treatment group. However, if future studies in this area replicate these results, there may be some implications for treatment programmes. For example, treatment programmes that focus more on readiness to change and behavioural POC usage will produce greater improvements in symptom severity levels following treatment. Thus, it would be worthwhile for programmes to aim to alter attitudes that are typical of the pre-contemplation SOC and increase involvement in behavioural change processes. This may be achieved by increasing participants’ (i) awareness of the effects of PTSD on their lives, (ii) sense of ownership of these effects, and (iii) belief in the possibility of change. The results suggest that veterans who are successful in substituting healthy behaviours, such as relaxation and graduated exposure, for problem behaviours (e.g. avoidance) and who use prompts to engage in such behaviours and reward themselves for doing so will achieve good outcomes. Future research might ask whether an increased focus on these processes will improve outcome relative to standard treatment. Improving treatment remains an important goal, because current treatment outcome in PTSD, especially for veterans, has not been satisfactory.
Footnotes
Acknowledgements
Preparation of this article was supported by grants from the University of Sydney's Postgraduate Research Support Scheme and the School of Psychology's Postgraduate Research Grant. The authors would like to thank staff at the Australian Centre for Posttraumatic Mental Health for their assistance with data entry and provision of valuable information.