
Abstract
Keywords
Several cross-sectional studies have documented high rates of depressive symptoms in individuals with HIV/AIDS [1–5]. By contrast, there is a paucity of data about longitudinal changes in depressive symptoms as HIV illness progresses. Prospective studies have provided conflicting results. Some suggest that the rate of depressive symptoms does not change over the course of the illness, until the period prior to development of AIDS when there is a significant increase in depressive symptoms beginning 12–18 months before AIDS diagnosis (‘pre-AIDS depression’) [6–8], while others find stability of mood despite HIV illness progression [9].
Lyketsos et al. [7] suggest both biological and psychological mechanisms may explain the phenomenon of ‘pre-AIDS depression’. In their study an elevated depression score in the earlier stages of infection, a self-report of AIDS-related symptoms, concurrent unemployment, cigarette smoking and limited social supports were consistent predictors of higher rates of depression as AIDS developed.
Understanding the association of depression and HIV/AIDS has important practical implications. Patients with syndromal depression and depressive symptoms have been shown to have substantial impairment in physical, social and role functioning comparable to or worse than that of patients with major chronic medical conditions [10]. Depression may contribute to non-compliance with medical treatment [11,12], to the high rates of suicidal ideation in persons with HIV infection [13] and to the high risk of suicide in persons with AIDS [14].
The introduction of highly active antiretroviral therapy (HAART) in 1996 and 1997 has been shown to reduce mortality [15], and many late-stage complications such as Pneumocystis carinii pneumonia (PCP) [16], cerebral toxoplasmosis [17], cytomegalovirus (CMV) retinitis and mycobacterial lymphadenitis [18], as well as kaposi sarcoma [19]. The effect of HAART on depressive symptoms has not previously been examined.
This study continues previous work examining depression in association with HIV infection [5] and provides longitudinal follow up of a cohort of patients first seen in 1995 and 1996 [20]. The aims of the longitudinal phase of the study were to investigate the stability of depressive symptoms over time, explore possible reasons for the genesis of depressive symptoms, examine psychosocial adjustment over time and examine the effects of the introduction of HAART.
Method
The study was initially conducted at Fairfield Hospital, a 138-bed hospital for the treatment of patients with infectious diseases in Melbourne, Australia. During the course of the study the hospital was closed and patients were transferred for ongoing management to the Alfred and Royal Melbourne Hospitals. In addition, many patients were seen for follow-up treatment in one of several general practice clinics in suburban Melbourne. Details of the study method and data collection have been described previously [20]. Patients were enrolled into the study over a 12-month period (March 1995 to March 1996). Subjects were then followed prospectively over 2 years with assessment of mood, psychosocial and illness related variables every 6 months. Data collection was completed in early 1998. At each time point, the patients were interviewed by the research psychologist and completed the Beck Depression Inventory (BDI) [21], Life Event Inventory (LEI) [22], Core Bereavement Item questionnaire (CBI-17) [23], and the Psychosocial Adjustment to Illness Scale (PAIS-SR) [24].
Ethical approval for the study was given by Fairfield Hospital and the University of Melbourne Research and Ethics Committees. Subsequent approval was granted from the Research and Ethics Committees at the Alfred Hospital and Royal Melbourne Hospital.
Results
Over a 12-month period, 227 patients (212 males, 15 females) were invited to participate in the study; 194 agreed to enter the study. Two of these patients did not complete the baseline interview. The remaining 192 patients (179 male, 13 female) completed the baseline evaluation. Twenty-nine of this group were found to have a depressive illness and so were deemed ineligible for the longitudinal follow-up study and were removed from the study cohort. These patients received treatment for their depression according to usual clinical practice. Thus, 163 patients proceeded on to the 2-year prospective follow-up phase.
Over the course of the study, not all patients were seen at each time point. Of the 163 seen at baseline, 25 were not seen again at any follow-up assessment. Thirteen patients were found to have a depressive illness and having reached an endpoint were removed from the cohort over the follow-up period. Data were available for 91, 74, 70 and 80 patients at 6, 12, 18 and 24 month follow up, respectively. Complete data collection was achieved for 27 patients.
Sociodemographic variables
The 163 patients (151 males, 12 females) were aged 25–62 with a mean (± SD) age of 38.7 (± 8.0) years. The risk category for acquisition of infection for the majority of subjects (n = 118, 72.4%) was homosexual/bisexual sexual contact. Twenty-five (15.3%) had a history of homosexual/bisexual or heterosexual contact and intravenous drug use (IVDU). Half of the patients were on sickness benefits or pension (n = 82, 50.3%), 45 were in full-time employment, and 18 were in part-time employment. At baseline, approximately half of the participants (n = 93, 57%) were in a stable relationship. Most patients were living with another person (family, partner or friend), only 42 (25.8%) were living alone. Relationship and employment status and living arrangements did not significantly alter over the course of the study. Patients had been aware of their seropositivity for a mean (± SD) of 6.1 (± 3.2) years.
Comparison of those who continued in the study and those lost to follow-up showed no differences in mean age, sex, Centers for Disease Control illness stage, HIV risk exposure category or baseline mean BDI, CBI–17, LEI or PAIS-SR scores. More of those who continued in the study were employed (p = 0.53), living with a partner (p = 0.007) and taking antiviral medications (p = 0.014) at the baseline interview than those who were lost to follow up.
HIV illness progression over 2 years
At baseline (1995 and 1996) the majority of patients were well, only 46 (28%) had AIDS. Baseline mean (± SD) CD4 count was 276 (± 249) cells/mm3 (range 0–1328). Treatment at the time of entry to the study included a variety of antiretroviral medications: zidovudine (ZDV; n = 104, 64%), didanosine (ddI; n = 29, 18%), zalcitabine (ddC; n = 24, 15%) and lamivudine (3TC; n = 19, 12%). One third (n = 53) were on monotherapy, 68 (42%) were taking two drugs, only three were on triple therapy and one-third were on no therapy.
During the 2-year follow-up period, 10 patients developed an AIDS-defining illness and 18 patients died. Mean CD4 cell count at each time point is shown in Table 1. Mean viral load is also shown for those time points at which this was available (viral load testing became available during the course of the study). Antiviral medication regimens changed considerably over the follow-up period. The proportion of patients treated with triple therapy over the course of the follow-up period is shown in Table 1. The mean viral load decreased markedly in association with increased uptake of triple combination therapy. In addition, the mean CD4 cell counts for the cohort increased in each subsequent time point.
Illness-related variables
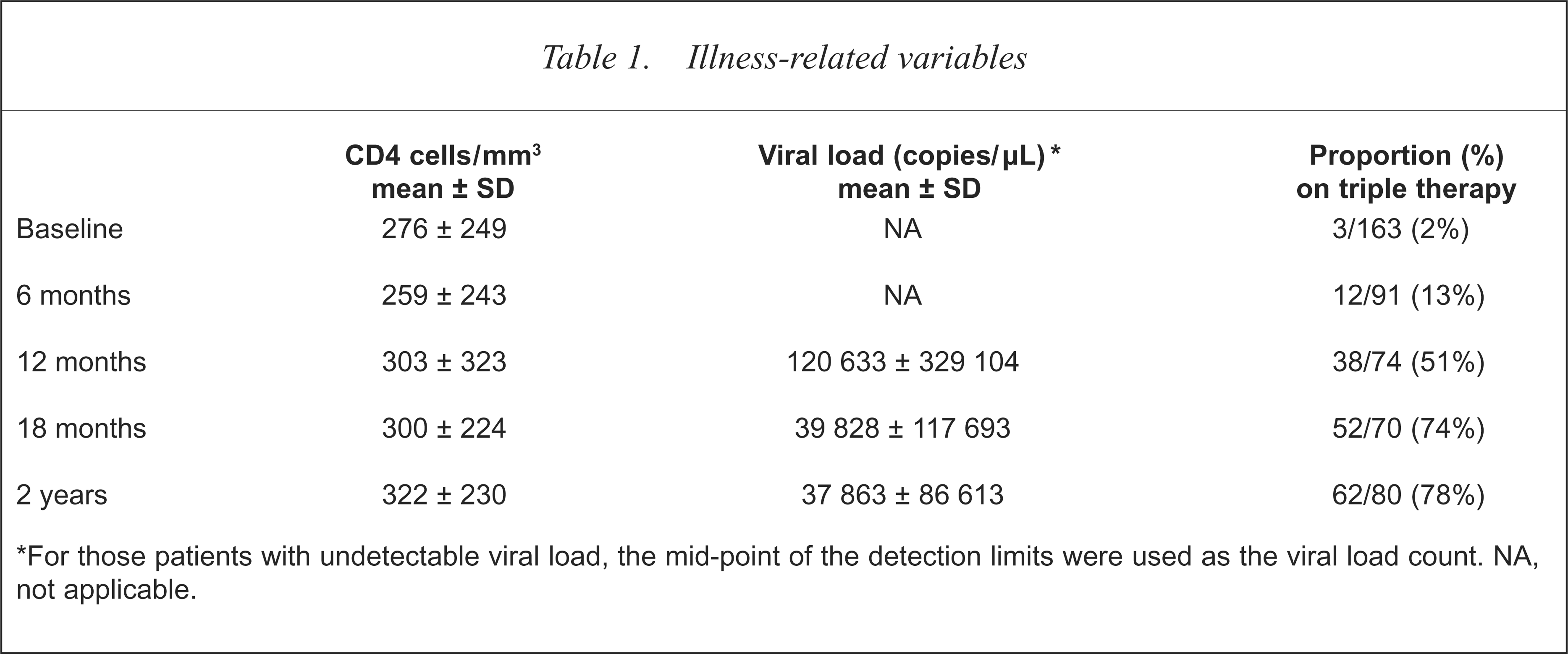
For those patients with undetectable viral load, the mid-point of the detection limits were used as the viral load count. NA, not applicable.
Psychological stressors: bereavement and life events
At baseline 89 (55%) reported they had recently (within the past 6 months) experienced a significant bereavement; the mean (± SD) CBI-17 score was 15.6 (± 10). Over the course of the study, less ‘significant’ bereavement in the 6 months preceding each assessment were reported. At each time point most who reported bereavements had lost a friend or partner. Table 2 shows the number of individuals reporting such losses and the mean CBI-17 scores. The mean LEI distress score at each time point and the proportion of patients scoring above the mean are also shown in Table 2.
Psychological variables
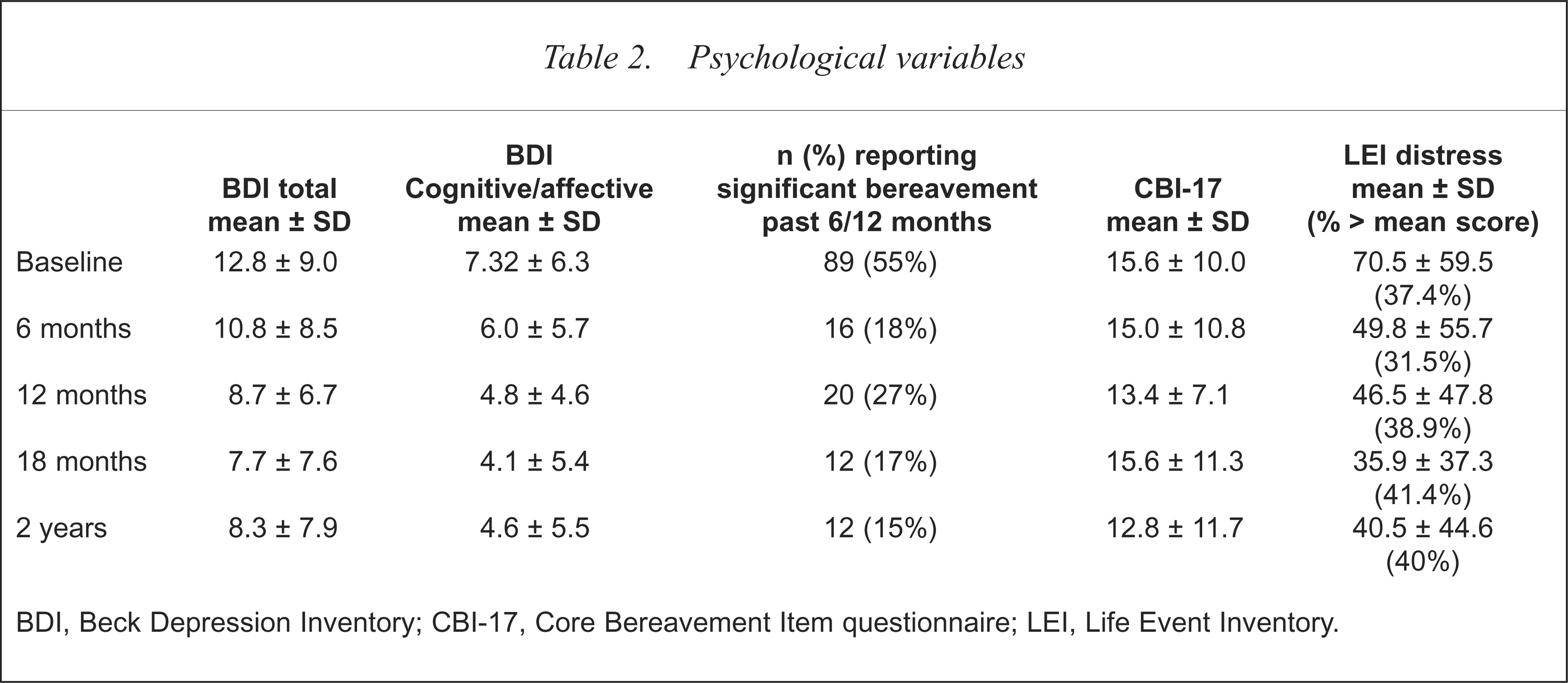
BDI, Beck Depression Inventory; CBI-17, Core Bereavement Item questionnaire; LEI, Life Event Inventory.
Do depressive symptoms change over 2-year follow up?
Baseline mean total score on the BDI for the 163 patients was 12.8 (SD = 9.0). Table 2 shows the mean total and cognitive/affective symptom BDI scores over time. Mean scores decreased after baseline reaching a nadir at 18 month follow up. Examination of individual BDI items indicated that the percentage of patients scoring ‘yes’ (defined as score of 1 or more) decreased over time for all items. The most obvious change was for ‘concerned about health’; two-thirds of patients scored ‘yes’ on this item at baseline, but only one-third scored ‘yes’ at 2-year follow up. Scores for each BDI item at each of the five assessments are shown in Table 3. Figure 1 shows the change over time for four key items: sadness, discouraged about the future, concerned about health and suicidal ideation. By visit three, 51% of patients were receiving HAART. As shown in Table 3 and Fig. 1, the percentage of patients reporting sadness at this time had decreased by 12%, and the number reporting worries about health, discouraged about the future and suicidal ideation had fallen by 7%, 11%, 15% respectively. Examination of the data for the 27 patients who were seen at each follow-up assessment showed the same pattern as that reported for the pooled data. Baseline mean BDI score for this group was 10.0 and mean scores at 6, 12, 18 and 24 month follow up were 7.4, 8.3, 8.3 and 8.0 respectively.
Frequency of Beck Depression Inventory items reported (% at each assessment)∗
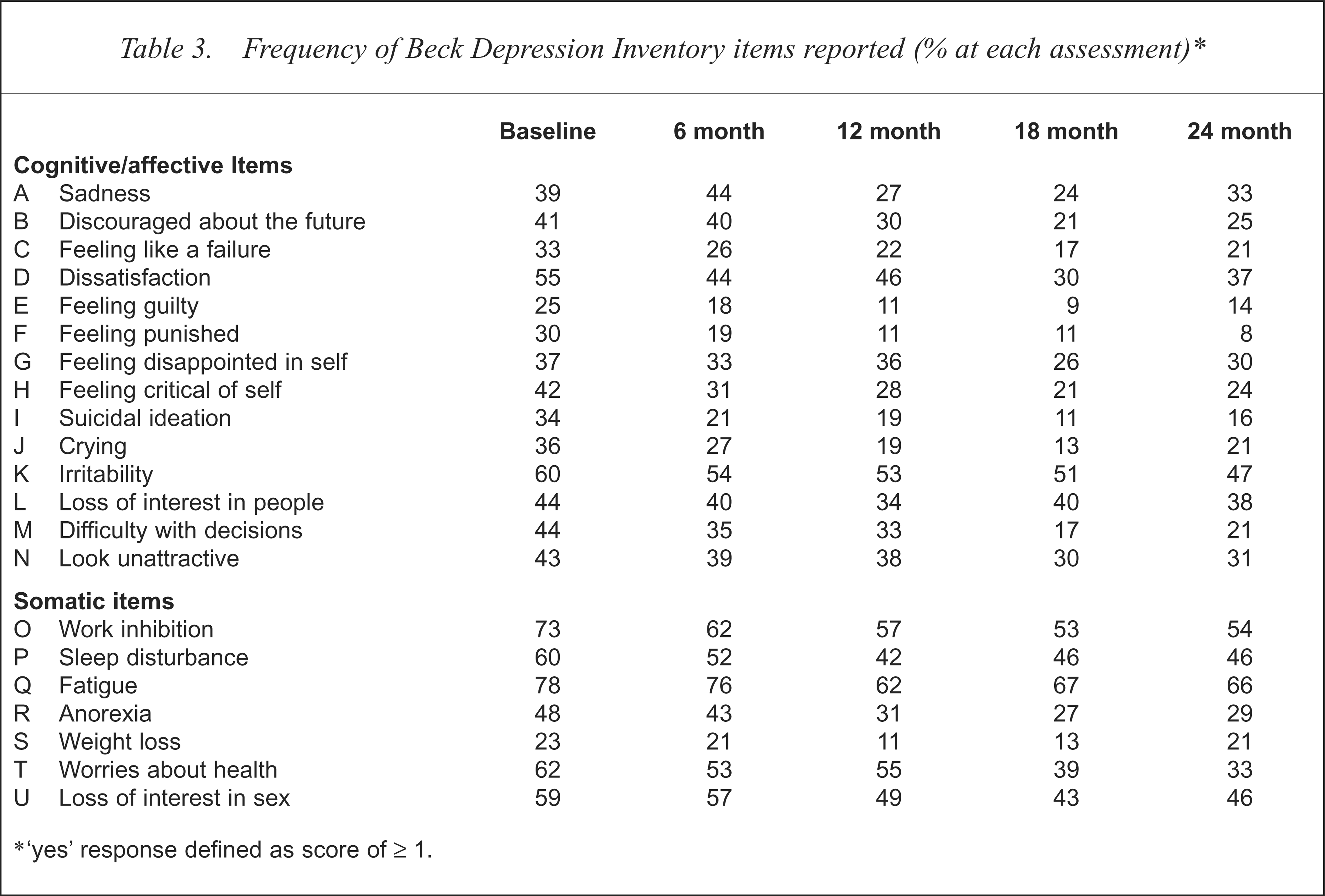
‘yes’ response defined as score of ≥ 1.
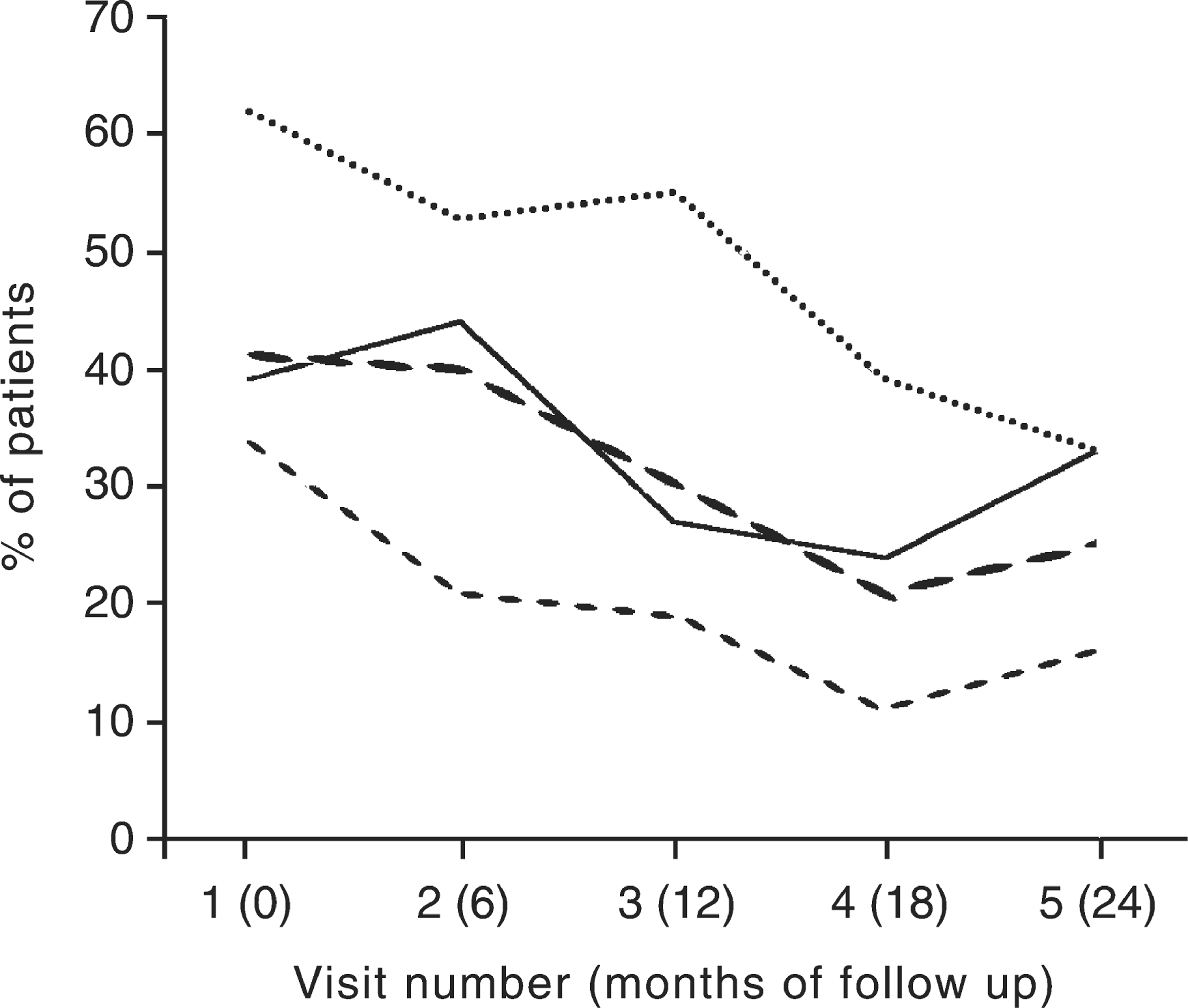
Frequency of Beck Depression Inventory Items over time. —-, sadness; – –, discouraged about future; —–, suicidal ideation; ········, worries about health.
Psychosocial adjustment to illness
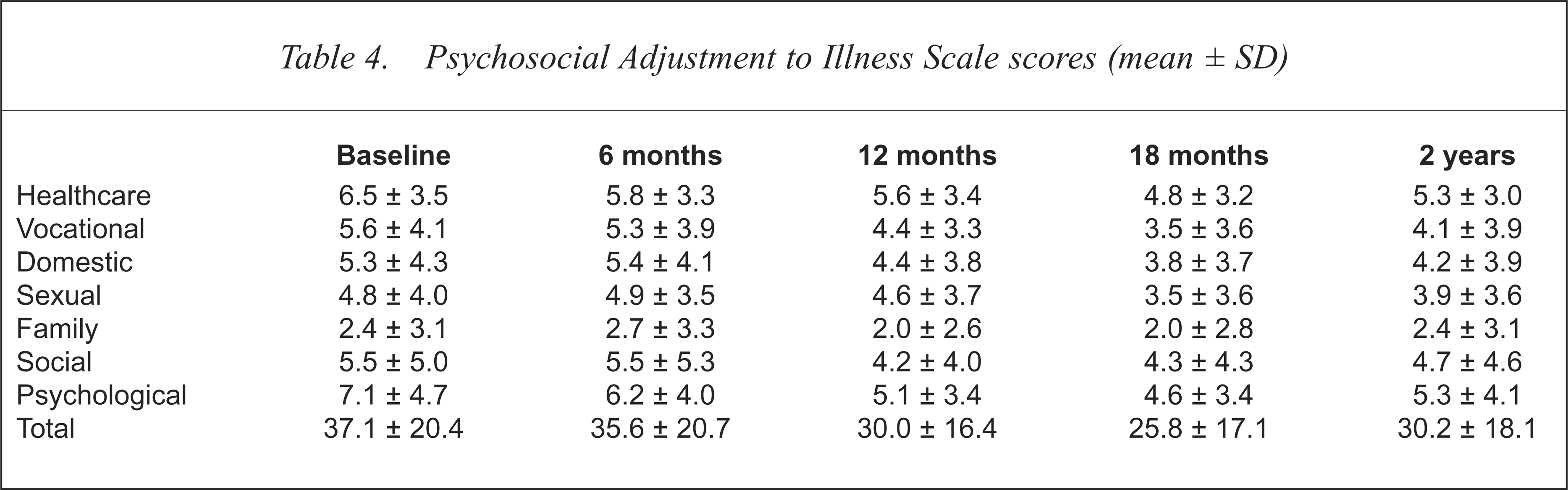
The raw scores on each of the PAIS-SR domains (healthcare orientation, vocational environment, domestic environment, sexual relationships, extended family relationships, social environment and psychological distress) and the total PAIS-SR score for each assessment time are shown in Table 4.
Psychosocial Adjustment to Illness Scale scores (mean ± SD)
Discussion
Participants in this study were patients attending the outpatient clinic of the major treatment centre for HIV/AIDS in Melbourne. The majority of participants were young homosexual/bisexual males; some were also IVDUs. This is consistent with the general pattern of HIV infection in Australia.
Over the course of the study, two major changes affected the cohort: change in site of treatment and change in antiretroviral medications. The closure of Fairfield Hospital in mid-1996 led to major changes in service delivery for patients with HIV/AIDS in Melbourne. Prior to closure, Fairfield Hospital was the major service for management of patients with HIV/AIDS in Victoria, caring for 70% of all patients diagnosed with HIV infection until that time. Following its closure, many patients transferred to the Alfred Hospital for ongoing treatment and some were treated at Royal Melbourne Hospital, while many elected to be cared for primarily by their general practitioner. The change in service delivery had a major impact on this study; many patients seen for baseline assessment could not be traced and were lost to follow up. Thus, unfortunately, there was a marked dropout rate between baseline and the first 6 month follow-up assessment.
The second major change was the introduction of HIV protease inhibitors; combined with previously available antiretroviral medications the use of these drugs led to a new level of treatment efficacy. During the course of the study, combination therapy, typically involving the use of two nucleoside reverse transcriptase inhibitors plus a protease inhibitor (highly active antiretroviral medication, HAART), became standard treatment. Coincident with the availability of the protease inhibitors, the HIV viral load assay became available for use as a clinical marker of HIV illness progression and as a tool with which to make treatment decisions. The use of combination medication regimens guided by viral load assay has resulted in dramatic changes in HIV illness progression; the overall improvement in CD4 cell count, the low rate of development of AIDS (10/163) and low death rate (18/163) in this cohort is consistent with the general pattern seen over this time.
Psychological stressors appeared to decrease over the course of the study. This may reflect the changes to treatment described above. Although half the group reported a recent ‘significant’ bereavement at baseline, this reduced to only 15% at 2-year follow up. Likewise, life event stress, as measured by LEI distress score decreased over the follow-up period.
Previous studies have found stability of depressive symptoms in the early middle phases of the infection, but have varied with respect to findings for the later stages of the disease [6–9]. Those who have found an increase of depression in the later stages of disease [7,8] have demonstrated an association between self-reported AIDS-related symptoms, unemployment, limited social supports and higher rates of depression.
Contrary to previous studies, the mean depression score decreased over the course of the study. Examination of individual BDI items (Table 3) indicates that there were changes in both cognitive/affective and somatic symptoms. Over the course of the study, fewer patients reported worries about their health, and the percentage reporting possible HIV/AIDS-related symptoms such as fatigue and anorexia also decreased. Co-incident with these changes in somatic symptom reporting there was a decrease in the proportion of patients reporting cognitive/affective symptoms of depression. Of note, the frequency of reporting of sadness and suicidal ideation decreased over the follow-up period; the proportion of patients reporting these symptoms at 2-year follow up was far less than that previously reported by our group in a similar patient cohort several years previously (49% sadness in the previous study vs 33% in this study; 40% suicidal ideation in the previous study vs 16% in this study at 2 years) [5].
Given the methodological problems of the study, the change in mean depression score over time must be interpreted cautiously. The large dropout rate between the baseline and first 6 month assessment is of particular concern. While the difficulties in follow up are most readily explained by the changes in service delivery, it is possible that those lost to follow up were more depressed than those seen for assessment. Further, patients found to be depressed over the 2-year follow-up period (n = 13) were treated for their illness and removed from the cohort. The death of 18 patients over this period may also have influenced the mean BDI scores recorded.
Comparison of our findings with previous studies is problematic. These studies were all published prior to the introduction of HAART. The introduction of HAART has both slowed illness progression and changed individuals' perceptions with respect to HIV/AIDS. The latter is well described by the following statement about the introduction of the protease inhibitors: ‘seldom in the history of medicine has an entire generation of patients with an incurable, progressive and ultimately fatal disease suddenly been offered the prospect of extended survival and even, perhaps, a second life’ [25]. Both the actual change in illness progression and the changed perception of illness resulting from the introduction of HAART might be expected to have an impact on the development of depression.
Although the mean depression score decreased over time, a significant number of patients continued to describe depressive symptoms. As described by Rabkin and Ferrando [25], the potential benefits of the protease inhibitors are not experienced by all those affected by HIV; some cannot tolerate the drugs, some develop resistant virus, some have illness progression despite HAART. For those who do improve, there may be conflicts and crises. Many who do improve have previously left the workforce, spent their savings and prepared themselves for a shortened life. Adjusting to the ‘second life’ may not be easy, especially when it is not certain how long this new phase will last, or what newly recognised toxicities (e.g. lipodystrophy, diabetes, risk of cardiovascular disease) will accompany it.
The reduction in mortality [15] and in late-stage complications of the disease [15–19] has meant that HIV/AIDS is now viewed as a chronic illness. As with other illnesses the level of disability associated with the illness and the treatments used for it may be increased by comorbid depression. This effect is true for both a depressive illness and depressive symptoms or ‘subthreshold depression’ [26]. This study suggests that depressive symptoms may be decreased in patients treated with HAART. Given the methodological problems identified here, further work is required to confirm whether this is indeed the case. The study also shows that patients treated with HAART continue to experience significant depressive symptoms. Further work to identify the cause of these symptoms, to examine the effect of these symptoms on the patient's illness and general level of function and wellbeing, and to identify appropriate and effective ways of managing these symptoms is also required.
Acknowledgements
This study was funded by a Commonwealth AIDS Research Grant. The authors gratefully acknowledge the assistance of the clinical research nurses at Fair-field and the Alfred Hospitals, Jean McCausland, John Lloyd, Andrew Gibbs, and the patients who consented to participate in this project.