
Abstract
The need for greater efficiency in publicly funded mental health services has lead to a search for patient attributes that predict resource use and outcome. Casemix was first developed in 1980 in the USA to define the output of hospitals and provide a basis for funding [1]. Although the Australian health system has progressed towards casemix funding of acute inpatient services, Australian National Diagnosis Related Groups (AN-DRGs) have not gained wide acceptance in the mental health system for clinical and technical reasons. These included their unsuitability for community-based services [2] and the absence of coding for severity or level of functioning [3]. Further issues have been the range of costs within individual DRGs and whether patients who stay in hospital for less than a day, or more than an arbitrary period, should be included in the analysis [2].
Internationally, a number of studies have investigated possible predictors of outcome in inpatients, but not those receiving community care [4–8]. A community-based study in Scandinavia was concerned only with subsequent admission to hospital as the outcome of interest [8].
Because of variations in methodology, predictors and outcomes, there have been conflicting results. In some studies, diagnostic groups such as DRGs have emerged as predictors of outcome [4,5,8], while in others they have not [6]. The aim of this study was to assess the effect of sociodemographic factors, diagnosis and disability on a range of outcomes including length of treatment, successful discharge from care and psychiatric improvement as measured by the Health of the Nation Outcome Scale (HoNOS).
The study used data collected for the Mental Health Classification and Services Cost (MH-CASC) Project. The project covered all States and Territories with the aim of developing a classification that was based on diagnosis, severity, level of functioning and other clinical and social demographic characteristics such as stage of illness and age [3].
The project collected detailed clinical, sociodemograhic and service use data on approximately 18 000 patients attending specialised mental health services in the public and private sectors. Mental health services provided by general hospitals without specialist psychiatric units and by GPs were not included in the study. Twenty-two sites participated in the study and were selected to represent 25% of the Australian mental health sector in terms of inpatient beds, workforce numbers and expenditure. Sites were broadly representative of services nationally [3].
Data collection centred on episodes of care received by all patients in contact with the service. Movement to a new treatment setting was defined as a new episode of care requiring a new set of data collection. Within each episode, data were collected at the beginning of the episode, at 14-day intervals during the episode and at the end of the episode.
Service-use data were provided by staff who kept the diaries of all activities over the 3-month period from 1 September to 30 November 1996. Daily activities and costs were divided into those for direct patient care and those for other purposes, and standardised to control for variations in salaries between sites.
The MH-CASC Project only considered costs. The aim of this paper was to use data from the two Western Australian sites in the project, Bentley and Fremantle Mental Health Services, to investigate predictors of a wider range of different outcomes using a care pathways methodology. Both services are in the public sector, and located in the south metropolitan area of Perth.
Care pathways studies (CPs) can be used to describe patients' experiences of specialist services such as the length of time in treatment, episodes of care they received and whether they have been successfully discharged. Studies have been undertaken in the areas of myocardial infarction [9], primary care [10], orthodontics [11], stroke [12] and psychiatric services [13,14].
The aim of this study was to investigate predictors of outcome and cost for all patients treated by Fremantle and Bentley Mental Health Services using logistic regression to adjust for potential confounding factors. These services provide inpatient, day-patient and community psychiatric care in the south metropolitan area of Perth, covering a population of just under half a million.
Ethics approval for this study was given by the Fremantle and Bentley Hospitals and Mental Health Services.
Method
Data were collected over 3 months on the 2691 subjects (47% male, 53% female) who attended Fremantle and Bentley Mental Health Services. Outcomes included: (i) length of care in both community and/or inpatient settings with subjects divided about the median into short and long episodes; (ii) standardised 3-month cost per day divided about the median into high and low cost; (iii) clinical response as assessed by improvement in HoNOS score and discharge from services. Discharge was defined as having completed treatment with no further follow up being arranged with specialist psychiatric services. Discharge did not mean transfer to another specialist service for treatment or being lost to care. Table 1 shows the possible predictors of outcome that were investigated.
Possible predictors of outcome
The effects of the presence or absence of each variable under investigation on outcome were examined using adjusted odds ratios. These were derived using forward stepwise logistic regression to determine the relative importance of clinical and sociodemographic variables on outcome. The significance of each variable entered into the model, compared with the model without the variable, was assessed using the likelihood ratio statistic. This has a χ2 distribution with one degree of freedom and is a measure of the relative contribution of each independent variable to the outcome or dependent variable under investigation. Data were analysed using the Statistical Package for Social Sciences (
Results
The average age of subjects was 44.3 years. Nearly 80% of subjects (n = 2128) received care in community settings, inpatient care being reserved for acute emergencies. The most common diagnosis was schizophrenia accounting for one-third of the sample (n = 902). A further 29% had a mood disorder (n = 785). Other diagnosis included 223 patients with organic disorders (8%), 295 with adjustment disorders (11%), and 111 with personality disorder (4%). Within the study period, 88% of patients had only one episode of care (n = 2361), and a further 8% two (n = 223). A small minority within the study period of 3 months (4%) required up to seven episodes of care (n = 107).
Thirteen per cent of the sample (n = 359) were discharged from the service during the course of the study (Table 2), generally to the care of their general practitioner. The median length of care was 70 days (Table 3). Patients with schizophrenia were one-third as likely to be discharged from care (Table 2) and 30% as likely to have longer episodes of care (Table 3). Patients with personality or substance-use disorders spent less time in treatment (Table 3) and were more likely to be discharged (Table 2). Those with organic or adjustment disorders also spent less time in treatment (Table 3).
Factors associated with discharge from care
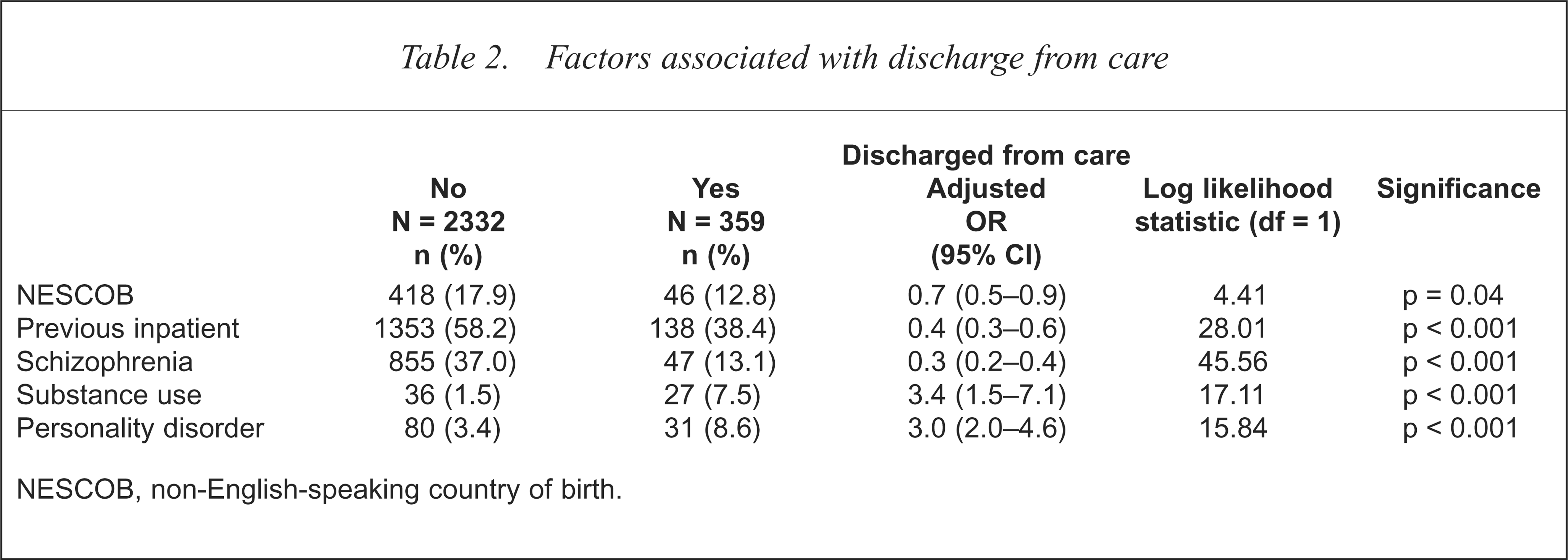
NESCOB, non-English-speaking country of birth.
Factors associated with length of care
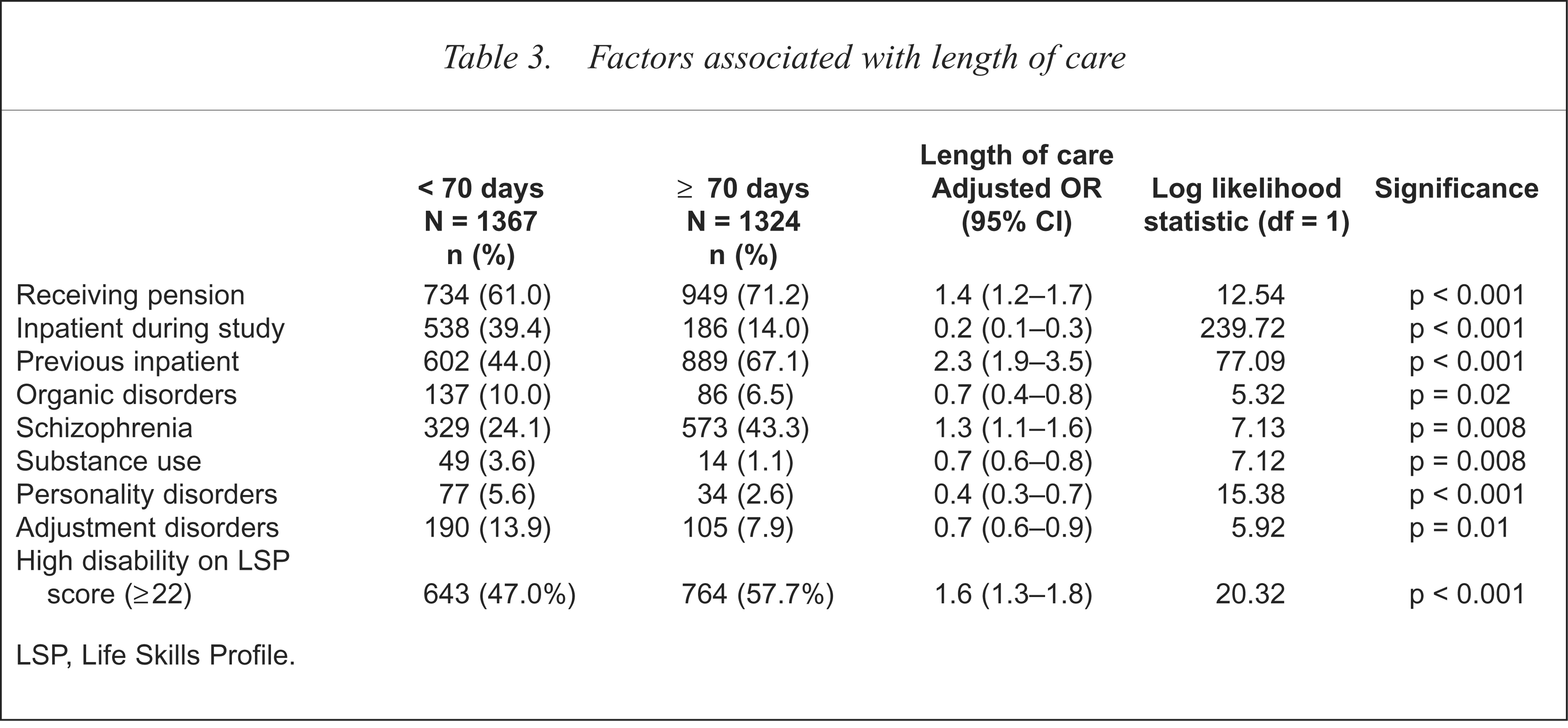
LSP, Life Skills Profile.
A past history of inpatient care was associated with a worse outcome in terms of length of care or not being successfully discharged (Table 2 and 3). By contrast, a spell of inpatient treatment during the study was associated with a shorter period of overall care (Table 3). Measures of illness severity that were investigated included involuntary treatment, HoNOS and disability on the Life Skills Profile (LSP). One or other of these measures were associated with increased costs (Table 4) and longer periods of care (Table 3).
Factors associated with an increased standardised 3-month cost per day
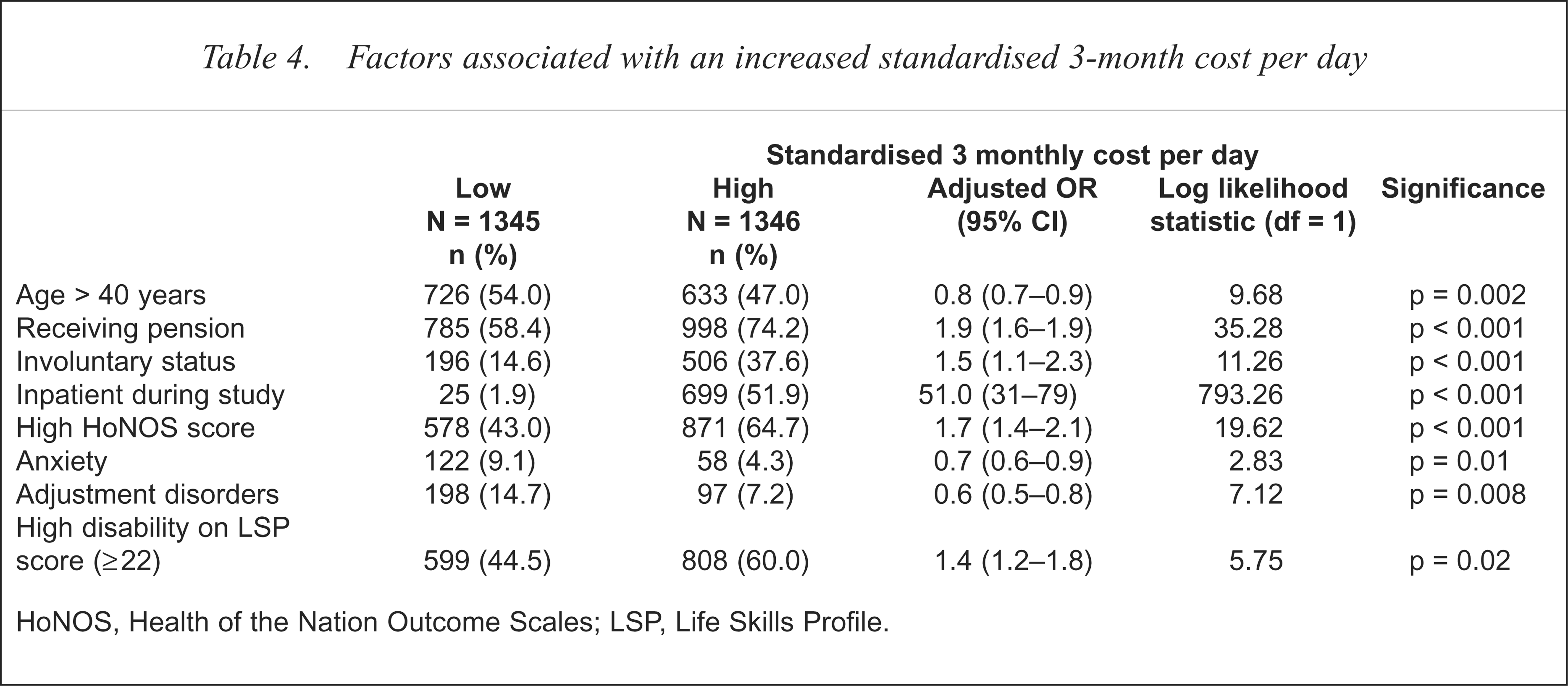
HoNOS, Health of the Nation Outcome Scales; LSP, Life Skills Profile.
Eighty-six per cent of the sample (n = 2319) had improved in the course of the study as measured by HoNOS score (Table 5). Only female sex and a diagnosis of adjustment disorder emerged as independent predictors of improved HoNOS score, once initial severity of score was taken into account (Table 5).
Improvement in HoNOS score
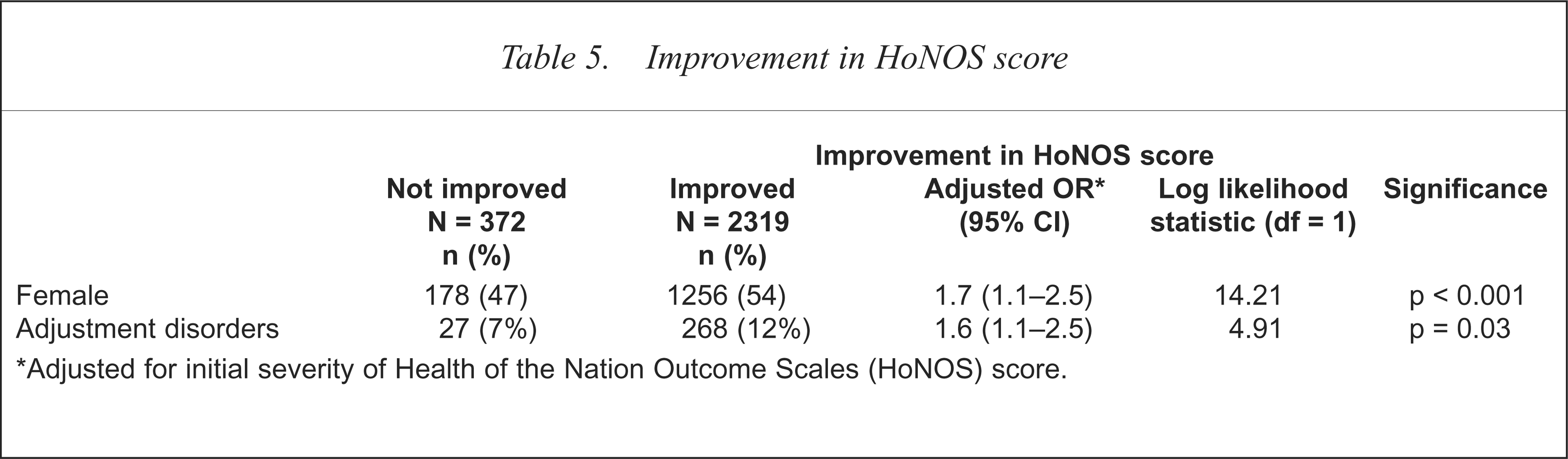
Adjusted for initial severity of Health of the Nation Outcome Scales (HoNOS) score.
The standardised median 3-month cost per day was $9.94 with a minimum of 30 cents and a maximum of $794.75. Sociodemographic factors were as least as important as diagnosis in predicting the cost and outcome of treatment. Patients who were from a non-English-speaking country of birth were less likely to be discharged (Table 2), while those on Social Security benefits or pensions were almost twice as likely to have longer and more expensive periods of care (Table 3 and 4). Younger age was associated with increased costs. Apart from anxiety and adjustment disorder, diagnosis did not emerge as an independent predictor of costs (Table 4).
Discussion
Mapping CPs using MH-CASC data had several advantages including the large number of patients studied, and the use of prospectively collected data that were routinely available. The present work was therefore not subject to recall bias unlike previous studies that relied on a retrospective questionnaire administered to subjects [11,13–15].
Limitations of study
The strengths of the present project also represent some of the weaknesses. In particular the reliance on MH-CASC from two different provider units meant that it was not possible to fully validate the information. There may have been variations in the way questionnaires were administered because of the large number of clinical staff involved and the way information was coded and entered.
The structured instruments used in this study, the HoNOS and LSP, were both designed for use in clinical settings without the need for intensive training of staff [16–19]. Interrater reliability for both instruments varies between acceptable and good, better agreement being achieved for the total rather than some of the subscale scores [16–19]. Both instruments have been validated and are sensitive to change, although in the case of the HoNOS [18,19], the change required is quite large in comparison with other standardised instruments such as the Clinical Global Impression scale or the World Health Organization Schedules for Clinical Assessment in Neuropsychiatry (SCAN).
Previous survey findings
As in inpatients, subjects with schizophrenia or a prior psychiatric history who are attending community-based services have longer periods of care, while those with substance use have shorter care pathways [5]. As in a previous Australian study of inpatients, gender did not predict length of care [5].
A number of additional factors were also associated with increased length of care, such as being an inpatient or receiving a pension. Substance-use and personality disorder were associated with shorter periods of care and, contrary to expectation, so was being an inpatient during the course of the study. These diagnoses were also associated with whether patients were discharged from care. Being from a non-English-speaking country of birth was also associated with not being discharged from services.
As in the larger MH-CASC study [3], inpatient treatment and severity of illness as determined by involuntary treatment, elevated HoNOS or disability on LSP were associated with increased costs in patients of Fremantle and Bentley Health Services. Surprisingly, younger age was also associated with increased costs. However, the larger MH-CASC study did report that while older age equated with greater costs for completed inpatient episodes, younger age was associated with increased costs for ongoing in-patient episodes [3]. Unlike the MH-CASC study, where schizophrenia and organic disorders were associated with reduced costs, only anxiety and adjustment disorders predicted a lower cost in this sample.
The finding that demographic factors are at least as important as diagnosis in determining outcome is similar to a study of inpatients in the UK [6], and raises the question of whether diagnostic-related groups are only likely to be useful if they include information on demographic features. However, it is also possible that some demographic variables such being on social security benefits or a pension may actually be proxies for severity of illness.
This study also suggests that predictors of costs and outcome will differ, depending on the outcome under investigation, and that it is important to consider a range of indicators when evaluating services. All units participating in the MH-CASC project were provided with their respective dataset and it may be appropriate for other centres to analyse their data in a similar way, either singly, or in combination with other sites.
Conclusions
Illness severity and demographic factors may better predict increased health service use than diagnostic casemix. Since sociodemographic variables contribute at least as much to outcome as diagnosis, comparing units is likely to be misleading unless these factors are also considered.