
Abstract
Aggression directed towards psychiatric staff and other patients is a significant problem in psychiatric facilities throughout the world. Aggression is currently one of the primary reasons for admission to psychiatric units with projections suggesting a 25% increase in admissions to psychiatric facilities due to violence by the year 2010 [1]. Research into aggression appears to be hindered by a variety of factors. Specifically, many differences in methodology and design render comparisons problematic. Local research with small sample sizes limits the usefulness of results to other clinical sites. Varying definitions of aggression also confound research [2].
Demographic factors have been extensively researched with difficult-to-interpret and, at times, conflicting findings [3–7]. In many studies the violent patient is typically male, under 45 years of age and has a diagnosis of schizophrenia [5]. Conversely, other researchers have found women consistently displayed more aggressive behaviour than men [6]. In yet other studies a diagnosis of schizophrenia has been associated with a lower risk of aggression, and substance abuse and personality disorders confer a much greater risk [7]. Involuntary patients have been found to be significantly more likely to engage in aggressive acts [4,8].
Recent research suggests the existence of a subgroup of patients who are more dangerous [9] and responsible for a large percentage of the aggression that occurs [7,10]. The likelihood of totally unpredictable assault is relatively small [11]. Specific times that patients are more likely to become aggressive include during admission, change of shifts, mealtimes, visiting hours and any period of change when nursing staff have varied tasks to complete [12].
The most common victims of aggression tend to be staff members. This is possibly due to their availability and relationship to the aggressor [3]. The extent of staff assault has been hard to establish due to the underreporting of incidents [13] and most figures come from single studies in individual hospitals or units, where levels of patient acuity differ both between and within studies.
Various factors may contribute to the development and escalation of aggression, and it is likely that these varied factors reflect the difficulties surrounding aggression prediction. Hallucinations [14], delusions [15], provocation [8], limit setting [8,16], alcohol and drug use [17], medications [8,16], overcrowding [4] and staff attitude [16] among others have been extensively researched. Methodological limitations that have been noted in these studies include small patient populations, coding errors, limited variables and insufficient documentation.
Studies using diagnoses as a predictor must take into account the base rates of that diagnosis in the study population. For example, the finding that patients with schizophrenia are involved in aggressive incidents must be considered in the context of whether they are overrepresented in psychiatric settings with respect to other diagnostic groups [18]. The present study aimed to investigate aggression within the context of the proportional diagnostic picture of the whole inpatient population. It was designed specifically to overcome limitations identified in previous research, and has the following merits: (i) all patients of Mental Health Services within the catchment area who were admitted during the study period were included in the study, providing a very large, representative population-based sample; (ii) the study extended over an 18-month continuous period, far longer than most other studies of this type; (iii) all aggressive incidents (both verbal and non-verbal) were documented on a purpose-designed aggressive incident report form, unlike some studies which use case note counts or staff recall; (iv) details of the aggressive incident were recorded at the time of their occurrence, not retrospectively; (v) aggressive incident report forms were completed by witnesses to the aggressive incident, were reviewed by senior staff, were subject to quality audits and were used in ongoing management planning, helping to ensure the validity, reliability, fidelity and compliance of reports and reporting procedures.
The Illawarra Area Health Service covers a catchment area of approximately 225 000 people [19] and covers an area of the east coast of Australia immediately south of Sydney centred on the city of Wollongong. The rate of admission and readmission to psychiatric units is one of the highest in NSW [Illawarra Area Health Service Strategic Plan For Psychiatric Services 1994/1999: unpublished report]. As part of the organisation's commitment to reducing violence, an Aggressive/Assaultive Incident Report Form was introduced to the facility. Compulsory annual attendance by staff at aggression management training and quality audits were also instigated. Critical incident stress debriefing was provided to victims or witnesses of assaults, and information on the actions taken to reduce the level of violence and what plans are in place was also provided to staff members. Despite these measures, there remained unacceptable levels of aggression within the inpatient units. The present study reviews data on aggression collected from the four acute and subacute psychiatric inpatient units in the Illawarra in order to determine prevalence and potential causal factors. The study aims to characterise patterns and prevalence of aggression within the context of the overall total admission rates, diagnoses represented, age range, gender distribution, date and time of hospitalisation in relation to date and time of aggressive incidents; summarise the nature of aggressive incidents; and identify additional causal factors, including substance abuse and aggression history.
Method
The study was performed on three separate acute psychiatric units, Eloura West, Eloura East and Mirrabrook, and a subacute unit, Lakeview House. Eloura West is a nine-bed, high-dependency locked area for acutely disturbed patients who require very close observation due to the severity of their symptoms. Eloura East contains 25 beds and was a secure unit during the study period. Voluntary patients can leave the unit upon informing staff and involuntary patients must remain in the unit unless the treating doctor grants leave. Mirrabrook is a secure 10-bed unit and caters for patients with less severe general psychiatric problems and is situated at Port Kembla Hosptial. Lakeview House is a 20-bed subacute rehabillitation unit situated close to the Eloura units within the Shellharbour Hospital campus.
Data were collected from the Aggressive/Assaultive Incident Report Form, which is a structured coding form with set check-box categories and guided narrative description. Information obtained from the form included the sociodemographic characteristics of the aggressor; date, time and focus of the assault (staff, self or another patient); causal factors contributing to aggressive episode; type of aggressive behaviour displayed; and any damage and injury that incurred. The form was usually completed by a registered nurse who was the victim of aggression or was a first-hand eyewitness to the incident. For this study an aggressive incident was defined as any act of verbal or physical aggression directed to self or others, irrespective of outcome. All incidents of aggression occurring over an 18-month period on these units during July 1996 to December 1997 inclusive were examined.
Detailed information was also gathered regarding total admissions to the units, specifically, date and time of admission, length of stay, age, gender and diagnoses. This information provided a profile of the general psychiatric population and the prevalence of aggressive incidents from the perspective of total flow of patients through the units during the data collection period. Diagnostic, age, gender and length of stay comparisons of non-aggressive and the aggressive patients are able to be determined from this data, as well as time between admission and any aggressive incident.
Principal diagnoses were made following a semi-structured clinical interview by the intake psychiatrist and were recorded by trained medical record coders in accordance with The International Classification of Diseases (ICD-9CM). The ICD-9CM codes were then collapsed into major diagnostic categories.
A random subset of the aggressive cases (n = 60) were identified for more detailed analysis in order to strengthen the description and prediction of aggressive behaviour. The types of aggressive behaviour displayed were profiled by manually content-coding the narrative descriptions of the incident written on the Aggressive/Assaultive report forms using the categories of Lehmann et al. [20] and Owen et al. [21]. Codings were checked by a second rater to ensure accuracy and consistency in coding. Substance use and aggression history were also located using a chart review. Data analysis involved χ2-analyses, odds ratio,
Results
Profile of the general psychiatric population and the prevalence of aggression
The study conducted over the 18-month period was on all psychiatric patients in the Illawarra Area Health Service admitted to one or more of four inpatient psychiatric units (n = 1269). Of this total patient pool, 174 patients were recorded as being aggressive. Therefore 13.7% of the total inpatient psychiatric population studied were aggressive.
Table 1 compares aggressive patients and non-aggressive patients for gender, mean admissions, length of stay and diagnosis. Males and females were equally likely to be violent. From the total population of 606 females, 12.2% were aggressive and 14.9% of 663 males were aggressive. A χ2-test failed to detect any significant differences between sex and aggressiveness (χ2 = 1.99, p = 0.16). A statistically significant difference was found for the mean number of admissions over the 18-month period for aggressive and non-aggressive patients (F = 125.22, p = 0.00). Patients who displayed aggression were admitted on average 3.56 times during the study period, as compared with 1.75 times for the non-aggressive patients. Per admission, the aggressive patients displayed some form of aggression on average 1.60 times. The mean length of stay for aggressive patients was 24.9 days. In contrast, the mean length of stay for non-aggressive patients was significantly lower, 12.1 days (F = 68.34, p = 0.00).
Comparison of aggressive and non aggressive patient profiles (n = 1269) over 18-month time frame. Number of patients are given in parenthesis
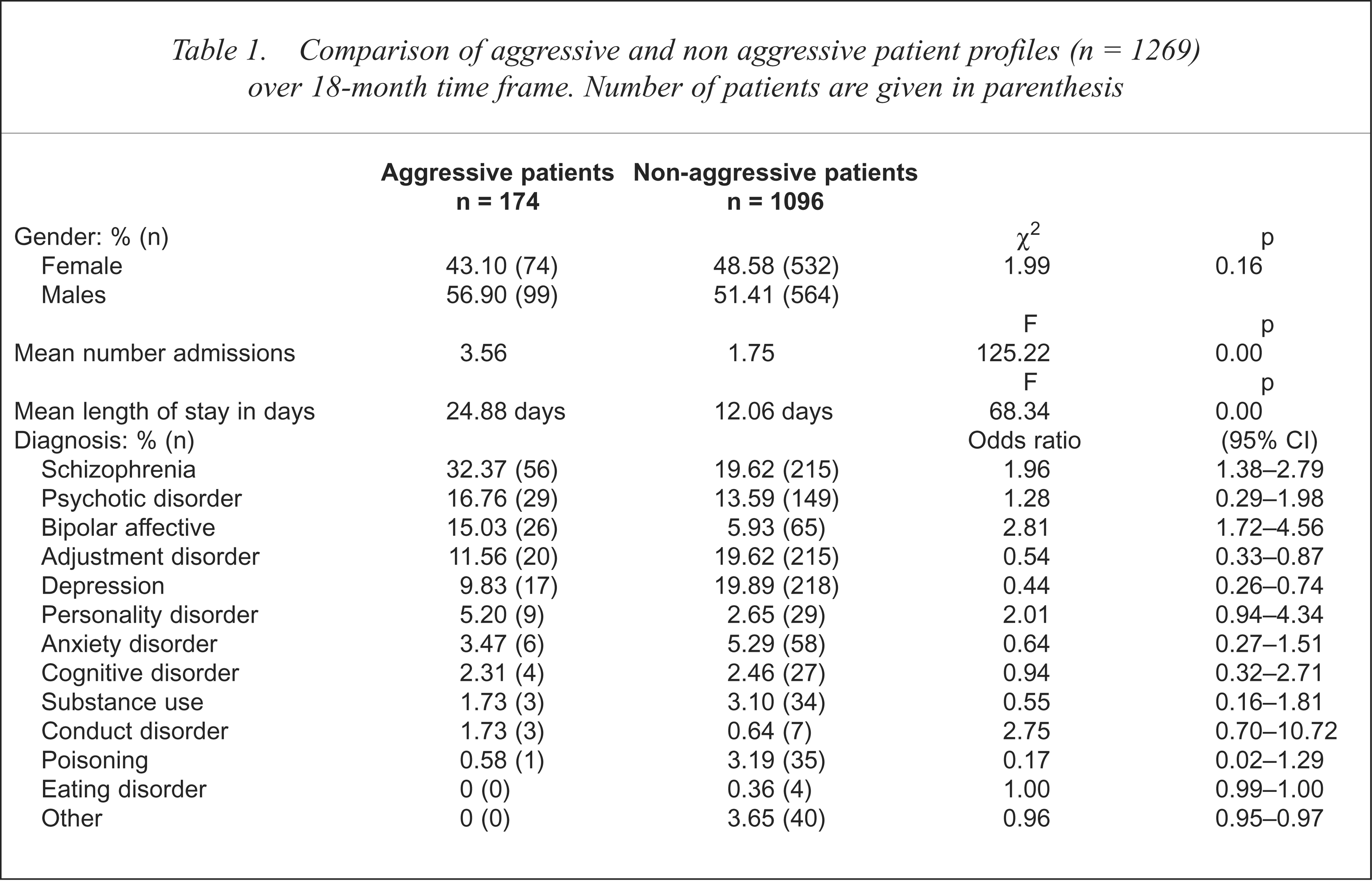
As shown in Table 1, two diagnostic groups, schizophrenia and bipolar affective disorder, were significantly more likely to be aggressive. Patients with schizophrenia incurred a 1.96 times increased risk of becoming aggressive, and patients with bipolar affective disorder a 2.81 increased risk. Conversely, two diagnostic groups, depression (odds ratio = 0.44) and adjustment disorder (odds ratio = 0.54), were significantly less likely to become aggressive, with both having about half the normal risk for aggression. Although the personality disorder and conduct disorder groups had high odds ratios, these were not statistically significant, probably in part due to the small sample size in both groups. It is important to note that these analyses were conducted only on the primary diagnosis, the impact of secondary diagnoses was not able to be investigated as these were not routinely coded.
For the 1269 patients in the sample there were a total of 2536 admissions, indicating that on average each patient was admitted twice. An overall estimate of 9.0% of admissions involved some form of aggression. For the 174 aggressive patients, there were 615 admissions during this period, which accounts for 24.3% of total admissions. Notably, multiple offenders comprised 40.2% of the aggressive population (n = 70) and were responsible for 71.0% of the aggressive acts.
The mean age of all patients was 37 years (range 13–97). However, age was not normally distributed (KSL Test for normality; D = 0.11, p = 0.00) with a higher frequency of admissions at the younger end of the range (median = 33 years). The average age of patients involved in incidents of aggression was 32 years (median = 30.00, range 13–85). No statistical significance was found when age by frequency of aggression was analysed for multiple and single aggressors (F = 1.33, p = 0.25). Most violence had occurred within 2 days of admission and the average time taken until the first aggressive incident was 42.30 h.
Profile of aggressive incidents
A total of 394 incidents were recorded across the four units (Eloura West n = 269, Eloura East n = 92, Mirrabrook n = 30 and Lakeview n = 3). All units except Lakeview had a high percentage of scheduled patients. Of the patients involved in the aggressive incidents, 83.8% were under the Mental Health Act (1990), and 68.0% were hospitalised in a secure unit such as Eloura West. For all units, the highest numbers of incidents occurred during the 07.00 hours to 15.30 hours time period (morning shift, 49.0% of incidents) and a high number of incidents on afternoon shift were also noted (36.0%), with episodes occurring less frequently on night shift (15.0%). On average, there were 5.05 aggressive incidents per week (394 incidents by 78 weeks studied).
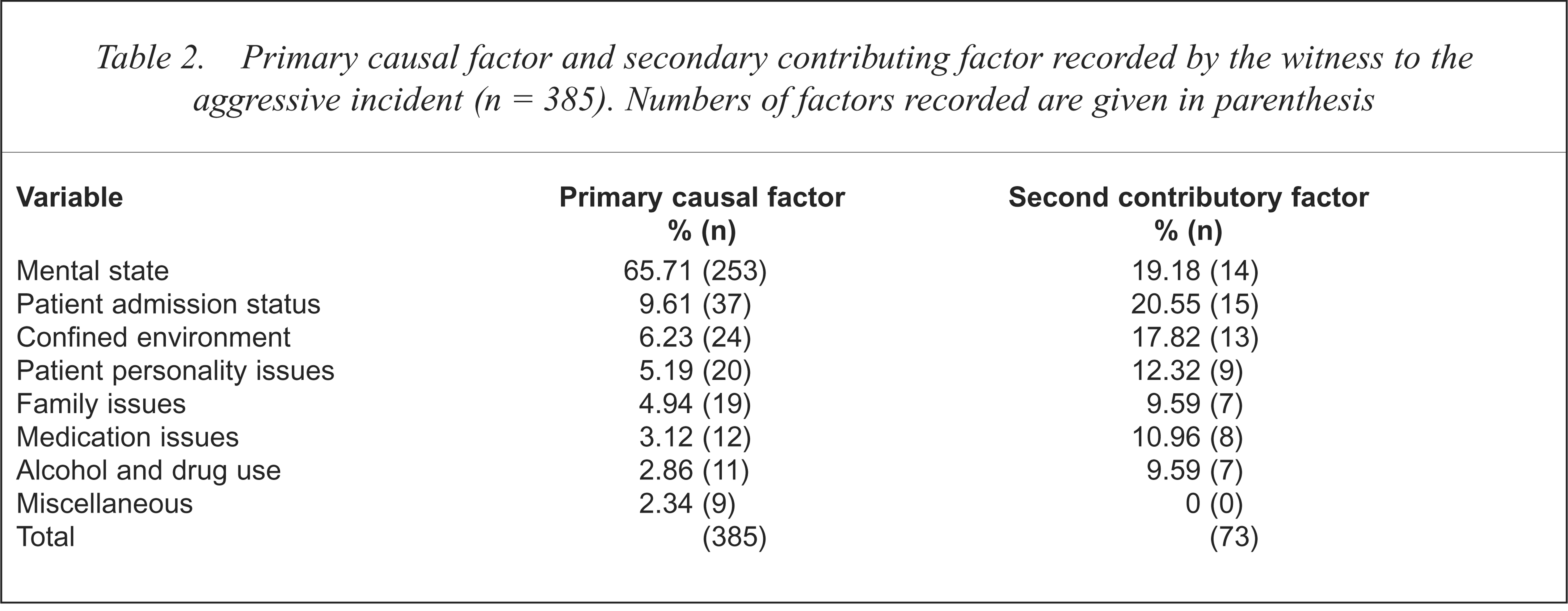
Table 2 shows the most likely causal factor for aggression, as well as the second contributory factor as specifically nominated by the witness on the incident report form. The cause of aggression was most often perceived by the witness to be related to a person's mental state (65.7%). A patient's admission status (9.6%), such as being involuntary and the nature of the confined environment (6.2%) were also considered primary causal factors in some incidents. In 73 (19.0%) of responses a second contributory factor was also nominated by the witness. Admission status (20.6%), mental state (19.2%) and the nature of the confined environment (17.8%) were also perceived as likely contributing factors. The average number of perceived causal factors noted per patient was 1.2.
Primary causal factor and secondary contributing factor recorded by the witness to the aggressive incident (n = 385). Numbers of factors recorded are given in parenthesis
Verbal aggression was evident across most diagnostic groups, particularly those with schizophrenia (72%), bipolar affective disorders (66%) and personality disorders (63%). In general, patients who were physically aggressive were more likely to have a diagnosis of bipolar affective or personality disorder. Verbal aggression was most often directed equally toward other patients or themselves. Patients with schizophrenia were most likely to be verbally, rather than physically, aggressive. However, patients with schizophrenia and cognitive disorders who were physically aggressive were more likely to direct aggressive behaviour to staff. Not surprisingly, nursing staff received the highest rates of injuries and assaults as they were more likely to be permanent staff members on the ward, therefore increasing their opportunity to be involved in incidents. Staff received a total of 45 injuries (across 11.4% of all incidents) and this accounted for 47.4% of the overall injuries incurred.
Profile of a random sample of 60 aggressive patients
A more detailed analysis was made of the types of aggression displayed and the substance abuse and aggression history of a randomly selected subset of cases (n = 60) from the 174 aggressive patients. Most patients had a previous history of aggression (78.3%). Table 3 presents the types of aggressive behaviour reported. Verbal abuse without a direct verbal threat was the most frequently encountered form of aggression (22.8%). Battery of a person or physical assault was common (14.6%) as was specifically directed verbal threats (10.6%), aggressive outbursts directed toward property (11.4%) and loud and demanding behaviour (16.3%). During the coding of the narrative descriptions of the aggressive behaviours displayed, it became evident that the presence of delusions or hallucinations was a very common causal or contributory factor in the incident, and was found in 53.3% of the reports.
Types of aggressive behaviour reported for the randomly selected subset of cases (n = 60)

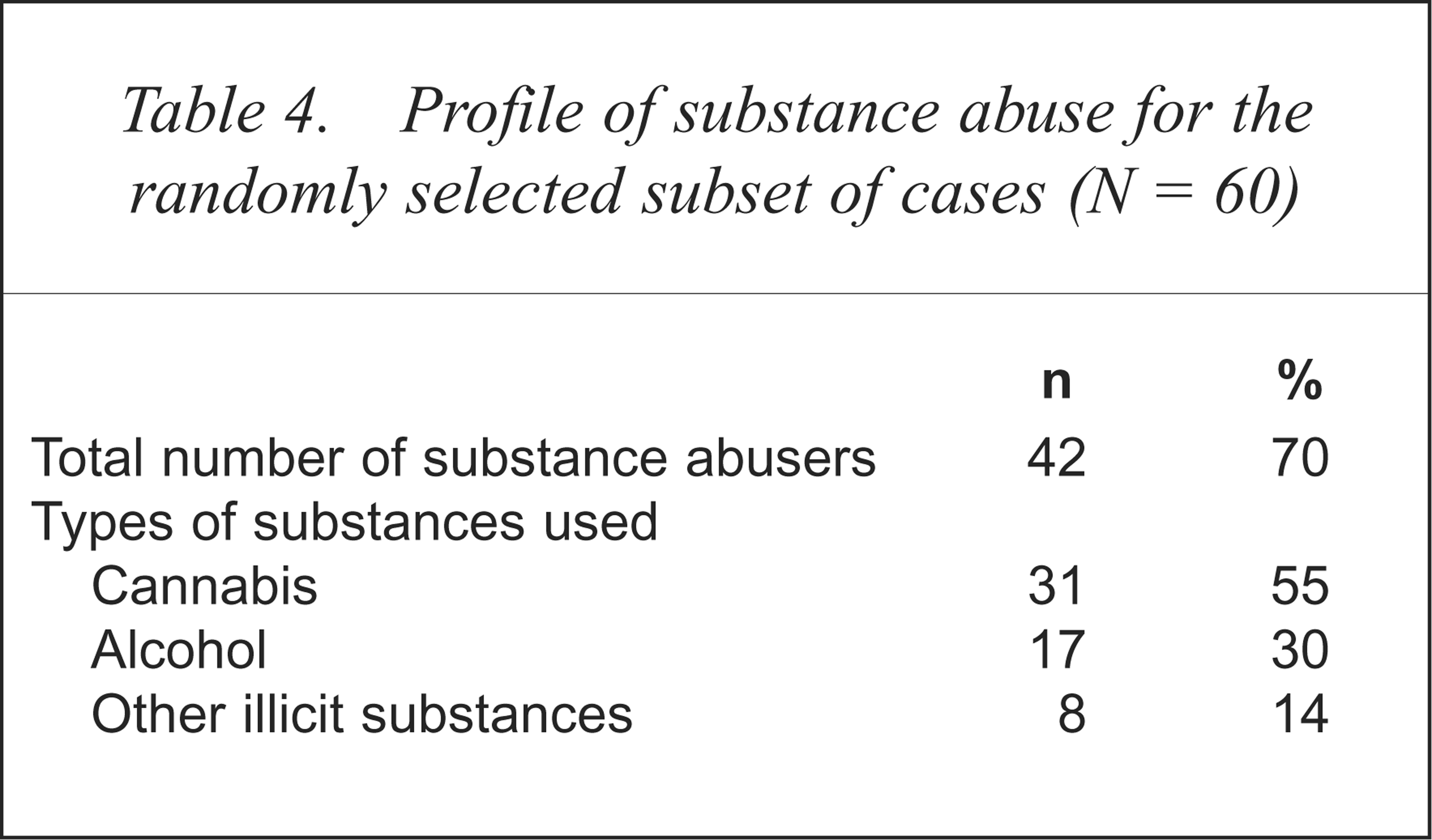
Table 4 presents a profile of substance abusers from the sample of 60 aggressive patients. The regular use of cannabis (55.4%), alcohol (30.4%) and other illicit substances (14.3%) was common. A relatively small percentage of patients (30.0%) either denied the use of such substances or documentation indicated that no history existed. The use of more than one substance was common. The relationship between aggressiveness and substance abuse appears prevalent among the subset of cases. Of the 60 aggressive patients 78.6% were both substance users and multiple aggressors. Being a substance user lead to a 1.83 increased chance for multiple aggressiveness within the time frame of the study.
Profile of substance abuse for the randomly selected subset of cases (N = 60)
Discussion
Most patients admitted to the psychiatric inpatient units did not display any aggressive behaviour (1095 of the 1269 patients admitted), with a total of only 174 (13.7%) patients recorded as aggressive during the 1.5-year study period. Patients with a diagnosis of schizophrenia were the largest diagnostic group, however, the prevalence of aggression was highest in patients with bipolar affective disorder. The finding that patients with bipolar illness are more likely to display aggressive behaviour is consistent with several studies [6,7,22]. It is possible that the irritability and lability characteristic of manic patients makes them more prone to assaultive behaviour compared with patients with schizophrenia.
The finding that schizophrenia also may be causally related to an increased chance of aggression is supported in various other studies [3,5]. Binder and McNeil [23] state that during the first few days of hospitalisation, the risk of physical assault by patients with schizophrenia decreases rapidly, possibly because of their quick response to medication and ward structure. This current study data suggest that during the first 46 h of hospitalisation staff need to pay particular attention to the potential for aggression. In assessing individual cases, clinical judgement must be used. For example, a patient with mania may become violent for the first time after admission, when exposed to the limitations of the ward milieu. In contrast, a person who has been aggressive towards family members in the context of delusions may not be aggressive to staff or patients outside that delusional system after admission [24]. In general, aggression was a daytime phenomenon, and this is congruent with findings from other studies [12,25]. The high number of incidents during morning and afternoon shift compared with night shift may also reflect the increasing demands placed on staff during the day by patients and also the decreased interaction between patients during the night. For those patients who respond to hallucinations of any type, their potential for aggression may escalate due to the increase in stimuli from the various nursing and patient activities during the day.
In this study neither sex was significantly more aggressive, in line with other research [4,24]. In regards to age, aggressive patients were an average of 5 years younger than comparison patients, and were much more likely to repeatedly assault. These results are consistent with previous research showing that dangerous patients were, on average, 4 years younger than comparison patients [22]. This is in keeping with the fact that a larger proportion of younger patients are likely to commit violent crimes, possibly due to their having secondary problems that contribute to aggression such as drug abuse.
The data from this study demonstrate that 40.2% of the aggressive patients were recidivists, and they accounted for 71.0% of the aggressive acts. At least one study suggests that there is a subgroup of patients who are persistently psychotic and resistant to neuroleptics [3]. These clinical characteristics may also explain why the patients displaying aggression have longer length of stays. It also raises questions about how to best identify this high-risk group and whether specialist interventions are advisable. Data from the present study have clearly identified that there is a high-risk, high-frequency aggressive grouping, and we have begun the process of identifying those factors which might be potential targets for therapeutic intervention.
A large proportion of patients displaying aggression had a history of aggressive behaviour. A history of aggressive behaviour has been found in some studies to be the best single predictor of subsequent violent behaviour [26]. Substance-use disorders were not common primary diagnoses in the participants, yet 70% of patients displaying aggression studied in the random subset were recorded as known substance abusers. This is suggestive that substance abuse is possibly predictive of aggression. There is now a need to clarify the nature of the relationship between substance abuse and aggression. For example, given that aggression occurs relatively soon after admission, are patients experiencing increased irritability as a result of withdrawal effects from their substance of choice?
The finding that most patients displaying aggression were likely to be scheduled (83.8%) is consistent with several studies [3,4,8]. The link between aggression and compulsory admission is only to be expected, as dangerousness to others in the context of mental disorder is one of the principal reasons for compulsory admission [24], and risk of harm to self or others is a defining criteria under the Mental Health Act. The present study found that nursing staff experienced the highest rate of injuries and assaults. In keeping with previous findings [7] patients suffering from bipolar affective and personality disorders were likely to display physically aggressive behaviour and patients with schizophrenia were more likely to display verbal aggression.
Descriptive data indicating the perceived causes of aggression suggested that acting-out was viewed primarily as a function of mental state or symptomatology and secondarily as a result of the confined environment characterised by limit setting. Supporting this is the apparent presence of active delusions and hallucinations among more than half of the 60 aggressive cases who received a more detailed analysis. Links have been made between psychosis and aggression [14]. However, several studies have found delusions and hallucinations to be unrelated to violence [27,28]. Several methodological limitations were noted in these studies including the data collection process, the use of untrained informants and the lack of adequately developed scales or questionnaires that assess the presence of command hallucinations. Therefore, results should be considered preliminary until additional research can usefully test associations of the positive symptoms of psychosis and aggression. Other sources of friction identified in previous studies were the patients' wishes to leave the unit, followed by disputes over medications [5,8,16,18].
This study has overcome some of the methodological difficulties of previous research in that it included four varied psychiatric inpatient settings, a large population-based sample size, a standard definition of aggression, the use of a purpose designed Aggressive/Assaultive Incident Report Form which covered both verbal and physical aggression, quality checks on the utilisation of the form to ensure fidelity and compliance in reporting, immediate data collection at the time of the incident rather than retrospectively and an unusually lengthy duration of data collection. Despite these safeguards, it is possible that some discrepancies may have existed regarding the manner in which the form was completed. Witnesses to an aggressive incident (who may also have been participants) may also have perceived the incident from a biased point of view. It is also likely and inevitable that some reports were made when aggression was not directly witnessed by staff because it occurred in an area that had no staff present at the time.
Aggression is a major health concern. Although only a small percentage of the psychiatric population studied was aggressive, within this, the recidivists were responsible for most of the aggression and also a large proportion of the admissions. The examination of such data may guide organisations to adopt additional valuable strategies for reducing the incidence of aggression. Identification, assessment and prevention are necessary to decrease aggression in the workplace. Organisations need to ensure aggression management strategies are in place and periodically identify and assess the level of risk for workers. The results from this current study have already been utilised in an improved aggression management training program (INTACT) in the Illawarra, and has lead to improvements and provided the model Aggressive/Assaultive Incident Report Form which has now been adopted in the New South Wales Centre for Mental Health funded Acute Services Project being piloted in the Illawarra, South-West Sydney and Hunter regions of New South Wales. A further implication of this study is the need to improve documentation of secondary or dual diagnoses, in particular, substance abuse. Substance abuse requires more careful documentation, using standardised interview protocols supported by urine analysis, than has typically been done routinely in psychiatric inpatient units in the past. Also, better assessments of current psychotic symptoms, including hallucinations and delusions, should be routinely be made, especially as this was also significantly implicated in the aggressive incident reports. It is only through improved assessment methods that pinpointing the relative contributors to aggression can be made, with consequent improvements in prediction and hence prevention.
Acknowledgements
The authors thank Professor Irwin Pakula (Director of Psychiatry), Sue Karpic (Director of Nursing), Sue Lampe (Quality Assurance Officer), Melissa Burton (Planning and Information Unit) and staff of the inpatient units, Mental Health Services, Illawarra Area Health Service for assistance in facilitating and supporting the data collection and Frank Deane for helpful comments on a earlier draft. This research was supported by the Illawarra Institute for Mental Health, and by funding to the first author by a nursing honours research scholarship by Mental Health Services, Illawarra Area Health Service.