
Abstract
Keywords
Advances in the phenomenology and neurobiology of posttraumatic stress disorder (PTSD) have emphasised the unique aspects of this disorder and have provided empirical support for the differentiation of PTSD from other psychiatric conditions with shared symptomatology [1–4]. These studies have lent even further support to the idea that PTSD requires specialised treatments. This argument has been accepted by the Food and Drug Administration in the USA with the registration of sertraline as a specific treatment for PTSD [Pfiser Pharmaceuticals: personal communication].
A major dilemma was posed for clinicians by the definition of PTSD in 1980 with the accompanying recognition that trauma survivors presented a unique range of reactions that could not be addressed using prevailing models of treatments or explained by existing knowledge. The lack of information at the time presented a major quandary for clinicians as to how to best manage patients, and still remains an important issue in clinical practice. Clinicians must therefore both ideally have an ability to function in the face of uncertainty and also to shift and prioritise information, as it emerges, which may reasonably inform assessment and treatment [5]. This uncertainty does not diminish the important work which has been done in investigating and demonstrating the effectiveness of several forms of treatment for PTSD as summarised in the treatment guidelines of the International Society for Traumatic Stress Studies [5]. This dilemma about the limited scope of current empirical knowledge raises a series of questions about how clinicians use information in planning treatment and what information might be of assistance.
There is a variety of knowledge which may be of use to a clinician. Of greatest practical utility is the literature which describes a technique and shares the experience of an experienced colleague [6,7]. Second, the increasing scrutiny of treatment interventions which have emerged in the last 30 years for a variety of reasons has lead to the treatment outcome literature [8,9] which is derived from clinical trials using control groups, random allocation of subjects and independent assessment. The other body of information which has a role in developing treatments is the descriptive literature about the epidemiology, aetiology and phenomenology of the disorder. The relationship between this descriptive literature and treatment practice is a complex dialectic which is seldom subjected to critical scrutiny in psychiatry. Very few treatment developments have followed on from descriptive findings about the aetiology of psychiatric disorders. More frequently, the dialectic is in the reverse direction where the discovery of an effective treatment intervention leads to the development or refinement of theories of aetiology. This has also occurred in relation to the aetiology of PTSD, for example the hypotheses that exist about the role of serotonin in obsessive–compulsive disorder have followed the apparent clinical benefits that are derived from the use of clomipramine in contrast to imipramine.
Having defined the potential sources of information and knowledge, what knowledge does a clinician require and how might information be of use? The politics of defining the ideal treatment of a disorder are considerable as the issue brings to life many conflicts about the relationship between psychotherapy and psychopharmacology. As well, boundaries and ownership of particular treatments are contested between professions. The role of cognitive–behaviour therapy is not neutral because academic psychology has partly tied its identity to this intervention, even though many of the pioneers in the field were psychiatrists such as Marks and Beck. There are further controversies with a treatment like eye movement desensitisation reprocessing (EMDR) which challenges some of the basic theoretical tenants such as prolonged exposure.
To date there is no ‘gold standard’ treatment program of PTSD, nor has any particular treatment approach received universal acceptance among clinicians. Although treatment outcome studies have found that some approaches do lead to symptom reduction, there appears to be a consensus among clinicians that treatments are not effective in addressing the full range of clinical problems observed in traumatised patients who present for treatment. Descriptive information about PTSD and its treatment may help define both the general aims of treatment and the choice of approach in individual cases. Knowledge may also assist the clinician to critique the treatment literature more effectively. Concepts about the aetiology of a disorder may also influence the attitude of the clinician to the patient and therefore play an important role in influencing the countertransference about trauma victims [6,10]. The latter issue is of particular interest in the trauma area given the stigma that has long been associated with the victims of trauma which played a substantial role in undermining the acceptance and recognition of the effects of trauma. In this regard, the idea that PTSD is a normative stress response has done much to modify attitudes to trauma victims [10].
In this paper we will examine some of the background assumptions in the treatment literature about the nature of PTSD and discuss these in the light of the descriptive literature about PTSD. One critical issue is that clinicians see a very limited spectrum of the victims of traumatic events, yet often make generalisations about the general nature of the psychological response to trauma. The skewed nature of clinical samples has become increasingly apparent from epidemiological studies which show that over 50% of the adult population have been exposed to these events [11,12]. Furthermore, general psychiatry continues to use treatments and develop aetiological theories which ignore the finding that in most psychiatric patient populations, PTSD is a cormorbid disorder in many patients and that the rates of severe traumatic experience is even greater than in the general population [13,14]. In this regard, ideas generated from experience with identified treatment-seeking populations can not automatically be used to describe the nature of traumatic reactions in community samples. Furthermore, the populations involved in treatment studies are often not representative, with many of the more complex and challenging patients either refusing to participate in these studies or not being accepted into the study on the basis of the exclusion criteria.
The limited efficacy of PTSD treatments [15] may be, in part, explained by the results of recent studies that have provided unanticipated information about the nature and aetiology of posttraumatic symptoms [16]. These studies have tended to challenge the original theoretical propositions that resulted in the acceptance of PTSD as a distinct diagnosis [3], and as a result, have challenged the conceptualisations upon which clinical treatment approaches are based. Data showing the relative rareness of PTSD following exposure to trauma [17], the atypical rather than normative nature of the posttraumatic stress response [16], and the prevalence of pre- and posttraumatic comorbidity [11,18] compel us to re-examine the utility of original treatment formulations and progressively modify them in the light of emerging information.
Historical perspective in the treatment of posttraumatic stress disorder
The development of psychotherapeutic approaches to mental illness has historically occurred in the absence of definitive knowledge concerning aetiology. This need for intervention in the face of limited knowledge results in the application of treatment approaches that are derived from general, often hypothetical, constructs about the possible origins of psychiatric illness and/or from post-hoc analyses of cases in which successful symptom reduction has been achieved. The diversity of philosophical perspectives, and the fairly modest cure rate produced by any single treatment modality, likely account for the various views concerning appropriate treatments for mental illness, as well as for the lack of resolution concerning this issue.
Posttraumatic stress disorder stands in contrast to most psychiatric disorders because the major precipitating factors leading to symptoms are assumed, that is, PTSD occurs in response to severe and unusual stressful or traumatic situations [19]. In early formulations, the effect of trauma was described as being a state of information overload in which the individual experienced a series of trauma-related sequelae (e.g. intrusive thoughts, cognitions, emotional representations) as a direct result of the extreme novelty and intensity of the traumatic experience [7]. An underlying premise of this approach was that the traumatic event could not be fully mastered and integrated because its magnitude was too great to be accommodated by the individual's prior meaning systems [20]. Thus, the symptoms of PTSD were considered a continuation of normal acute traumatic phenomena, or rather, the failure of restitution following this process [21,22]. What evolved in the psychiatric nosology was an increased emphasis on the universal pattern of response to trauma, with a de-emphasis on differences that may be related to the type of trauma sustained [23] or the developmental stage at the time of exposure, even though these latter factors have been shown to be relevant to an individual's clinical picture [11,24].
The acknowledgement of trauma as a major aetiological antecedent of PTSD, and the formulation that PTSD was essentially a normative process, led to the conceptualisation of an optimal treatment approach. The ideal interventions would be those that saw PTSD within the framework of psychological posttrauma adaptations, and which were accordingly directed [6,25]. This perspective was markedly different from most psychiatric approaches which had their origins in the psychoanalytical approach that views current psychiatric problems as manifestations of conditions with earlier origins, most likely earlier than those being considered by the patients themselves. Indeed, it is interesting that some of the more polarised psychiatric approaches (psychoanalytic vs molecular genetic) share a concern with issues that predate the current or recent environmental stressor that may be producing immediate symptoms. Specialised treatment approaches for PTSD have generally been designed to be effective in situations where the trauma sustained by the individual accounts for the major variance of current symptoms. The focus on the impact of the traumatic event is what serves to differentiate specialised trauma work from more classic psychotherapeutic treatments [26]. While CBT has provided cogent explanatory models for the existence of the patient's current symptoms, there is a paucity of empirical information which ascertains the initial cause of the patient's disorder.
Specialised therapeutic approaches to the treatment of PTSD
The primary aim of specialised PTSD therapy is to allow the individual to quell the distress and arousal associated with the recurrent and involuntary reminders of the trauma and to minimise the accompanying behavioural and affective constriction [27]. This can be accomplished using any of a variety of modalities that have the goal of helping the patient move away from the persecution and ongoing suffering resulting from the event and its aftermath to a focused examination of, and participation in, the present and future [28]. The cardinal symptoms of PTSD are dealt with as the normative consequences of exposure to events of abnormal magnitude [29].
Trauma-focused therapy is typically described as progressing in a series of steps [21], although in clinical reality there is often a complex process of induction into treatment. First, the patient defines the magnitude and scope of the damage done by the trauma. This process requires the individual to recover and dissect their traumatic memories into different layers of meaning, and confront any unique dimensions about the traumatic experiences, including exploring the meaning of the event in the context of their prior and current experiences, or owning responsibility for actions taken during the event. This is part of the process of reactivating the fear structure associated with the trauma and developing a narrative of the experience [30]. The therapist assists the patient by helping him or her overcome the avoidance both of internal cues and external reminders of trauma and regulating mood states during the therapeutic processes [7]. Once the individual gains a sense of mastery over his or her intrusive recollections and mood states [27], he or she works to initiate intimate and rewarding social relationships in place of the progressive withdrawal and detachment that ensues following a traumatic event [31].
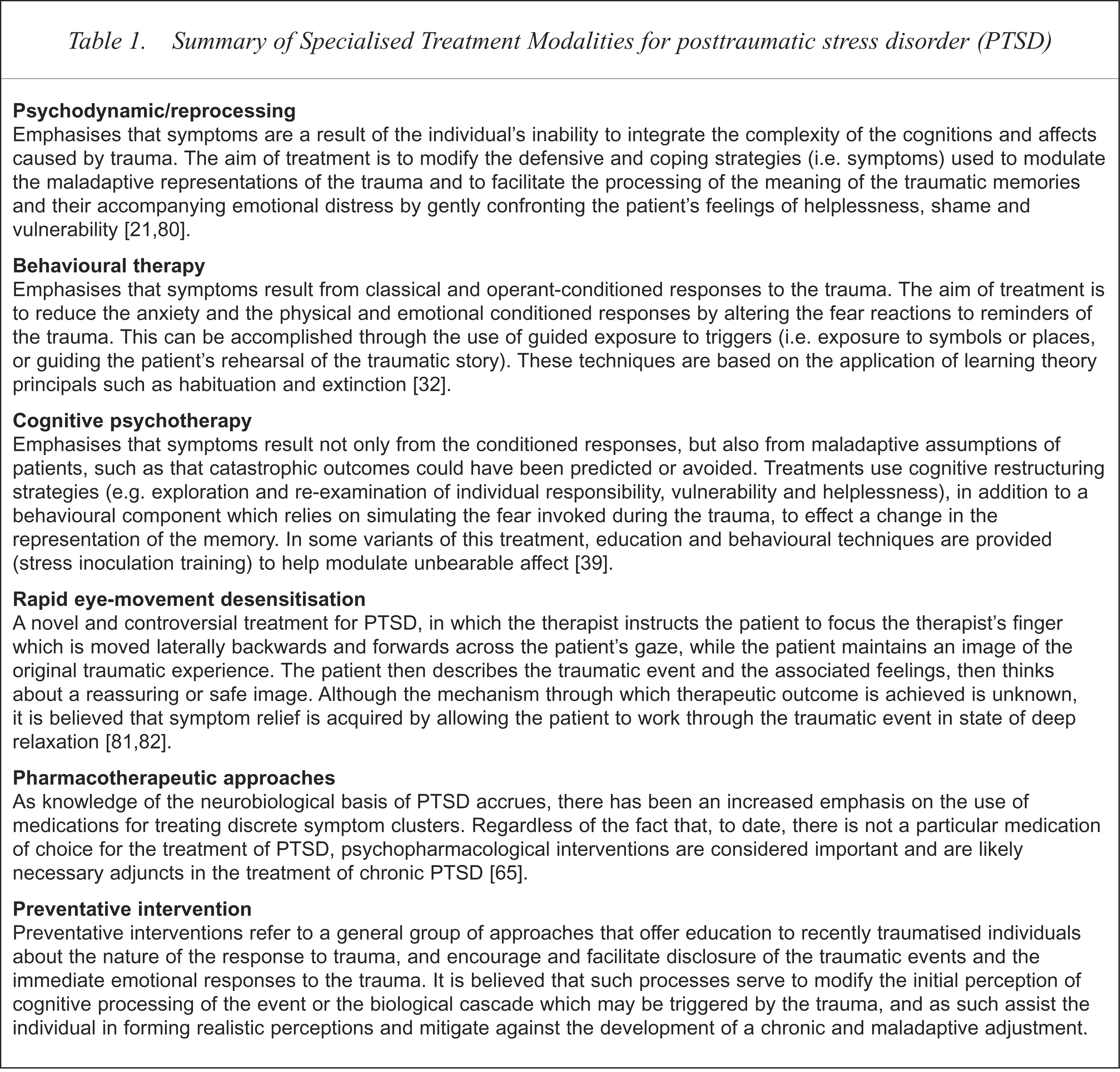
A summary of selected modalities appears in Table 1. Essentially, these treatments differ primarily in the techniques that are used by the therapist to provide safe environments that are conducive to recollecting the trauma and managing reactions to the remembering and working through of the memories. Two types of cognitive–behavioural approaches have been developed for use in the treatment of PTSD. In exposure treatments the patient is confronted with the feared memory or triggers using a variety of techniques [30,32]. Anxiety management techniques train the patients in a range of skills to control the anxiety of daily life. Affect modulation can also be addressed using pharmacotherapy in conjunction with more psychodynamic approaches [33,34].
Summary of Specialised Treatment Modalities for posttraumatic stress disorder (PTSD)
Regardless of which modality is ultimately chosen, there is usually some type of dialectic that occurs in trauma work of alternating between emphasising the more objective sequelae of trauma and exploring the unique aspects of the individual's psychological structure and personal history. In all types of specialised trauma-focused therapy the clinician and patient maintain an awareness of how this dialectic impacts on the way posttraumatic adaptations are interpreted and worked through in the therapy. Additionally, there are a series of other non-specific elements of the treatment process such as patient education, provision of hope, the context of a caring, non-judgemental relationship, which are central parts of the treatment process even though they are seldom described [35].
The issue also remains about the acceptability of these approaches to the patients. For example in one of the most rigorous and informative studies which investigated the use of exposure and stress innoculation therapy, approximately half of the women scheduled for assessment did not attend, with 19% of those offered treatment declining. There is also a significant dropout rate in the course of these interventions. Thus while treatments which have a primary focus on confronting the fear memory of the trauma have been demonstrated to be particularly useful, this is an approach which a significant proportion of patients will not consent to engage in.
Studies of treatment outcome in posttraumatic stress disorder
The treatment outcome literature, which focuses on the efficacy of specific PTSD treatments is still rather limited and confined to CBT, EMDR and medications, but it has generally suggested that specialised treatments do reduce symptoms in the majority of individuals [9,15,5]. However, there are numerous methodological issues which still require clarification in evaluating these outcomes. For example it is difficult to ascertain the biases involved in recruitment for treatment studies, and to know the impact of prior treatments on those being directly studied. Second, treatments studies often do not describe a range of issues that may be important contributors to outcome such as the role of education, the quality of the therapeutic relationship, and other non-specific factors. A significant number of patients in these psychotherapy trials are on medications. Therefore the actual efficacy of treatment may depend on a range of the factors [36].
It is difficult to know whether the results of these clinical trials would be sustained in everyday clinical practice with less experienced and sophisticated clinicians than those conducting the studies. For example, one of the conundrums is the clinical reality that while significant resources continue to be devoted to the treatment of trauma survivors such as Vietnam veterans, the need for services by these veterans has not perceptibly diminished. The ‘Koach’ project in Israel demonstrated that a program designed using the full range of current therapeutic knowledge by international experts led to a worsening of symptoms in Lebanon combat veterans [37]. The objective outcome measures in fact contradicted the claimed improvement by the therapists and patients. These examples reflect the reality of the complexity of the treatment of PTSD.
Furthermore, the specificity of the effect of different approaches is still unclear. Foa et al. [38,39] have been instrumental in demonstrating the clinical value of prolonged exposure. The careful examination of their data indicates that the gains dependant upon the confrontation of the fear memory structure are not essential to effective treatment. The 1991 study found that stress inoculation therapy which focused on current stresses was the most efficacious at immediate post-treatment. Supportive counselling was also as effective as CBT, although this was not demonstrated in Bryant et al.'s [40] study of the treatment of acute stress disorder where the benefit of exposure was clearly demonstrated. The long-term follow up of Foas et al.'s (1991) patients did not demonstrate a statistically significant advantage to any group [39]. When CBT and stress inoculation were combined, there was no demonstrable benefit statistically [39] suggesting that there may be a general degree of improvement that can be gained, rather than an additive effect, by focusing on different elements of the patients adjustment.
Statement of the problem: the conceptual and clinical conundrum of posttraumatic stress disorder
The currently advocated treatments for PTSD focus on working through the trauma and examining its profound impact on the individual's life. In this light, one of the relatively unexplored dilemmas may be how much to examine the syndrome as a reaction to the focal trauma versus as a consequence of pre- or posttraumatic factors.
This question arises not only as a result of the conflicting information from treatment outcome studies, but also because of several conceptual issues that have been raised by the findings of more descriptive research studies. For example, it is now clear that, although PTSD can occur in response to a traumatic event, the majority of individuals do not develop chronic PTSD following exposure to trauma [11,41–43], as reviewed below. The fact that only a proportion of individuals develop PTSD following a trauma indicates that there are risk factors for PTSD other than trauma exposure. Currently, the exploration of such risk factors are not an important component of specialised PTSD treatment. Second, the limited prevalence of PTSD raises the question of whether this condition should be treated as simply a manifestation of a normative response to trauma. In fact, there is now converging evidence showing that the direction of alterations in stress-related neuroendocrine systems such as the hypothalamicpituitary-adrenal [16] and catecholamine systems [1] in chronic PTSD are distinct from those that have been typically associated with the normal stress response. The lack of resemblance of some of these biological changes to those that have been typically associated with stress (e.g. low basal cortisol levels in PTSD vs the classic augmented cortisol levels observed in individuals undergoing stress) further support the idea that at least some aspects of the syndrome reflect an atypical stress response [16]. The difference in information processing of non-trauma related stimuli may necessitate the treatment of this problem [44,45] as this suggests a disruption of working memory. The affectively laden nature of the traumatic memory may be indicative of this more general abnormality of an inability to define the salience of current stimuli. The disruption of the individual's capacity to use language and to create an intervening narrative which buffers the affect of both the traumatic and other life stresses, may be the critical issue [46,47].
However, the numerous reports of a relationship between the severity of trauma and the severity of PTSD symptoms support the idea that exposure to trauma should remain the focus of treatment, and other more traditional factors should remain in the background [48]. It is particularly problematic, both conceptually and socially, to dismiss the effect of a trauma as the true cause of symptoms in individuals in favour of other ‘non-traumatic’ factors, simply because others who have suffered a similar plight did not develop as many symptoms. This is especially true for individuals who have been exposed to particularly brutal and horrific atrocities. Furthermore, in individuals who do develop PTSD following extreme trauma, the lack of success of traditional psychotherapeutic is well accepted, and has been directly attributed to a failure by the mental health field to adequately address the psychological consequences of the exposure [19].
The conceptual dilemma of how to appropriately evaluate the response to trauma and the proper treatment of this response will ultimately be resolved by acquiring a deeper understanding of the true underlying cause of symptoms, as well as a consideration that this disorder may have several aetiological roots and manifestations. It is likely that issues relating to different aetiological pathways and modifiers of post-traumatic states have important implications for the selection of specific treatment modalities. Moreover, factors such as the longitudinal course of symptoms and psychiatric comorbidity may modify the characteristics that need to be addressed in treatment at different points in the course of the disorder, regardless of the type of trauma originally sustained. There is also a range of contextual issues, such as the specific characteristics of treatment seekers, which will influence the application of generic treatment approaches. What follows is a description of aetiological, phenomenological and other considerations, and the way these factors may serve to modify the structure of treatment interventions.
Role of the stressor and longitudinal course
It was probably not anticipated by the initial advocates of the diagnosis of PTSD that the occurrence of this disorder would be relatively low compared with the prevalence of trauma. However, in a study sampling 1007 young adults from the Detroit community, Breslau et al. [42] found a lifetime exposure to a ‘criterion A’ traumatic event of 39%, while the rate of PTSD in individuals exposed to a traumatic event was 23.6% [42]. Further follow up of this sample has indicated even higher rates of traumatic exposure but similar rates of PTSD [49]. The National Comorbidity Study found that 60% of men and 50% of women had had a traumatic exposure with the lifetime prevalence of PTSD being 6.7% [11]. Other studies, particularly of non-treatment seeking samples, have also supported the observation that the presence of PTSD following a traumatic event is the exception rather than the rule [50].
Another important observation has been that approximately 60% of individuals who do develop PTSD following a traumatic event experience a significant decline in the prevalence of full-blown symptomatology with the passage of time [11]. For example, a longitudinal study of rape victims demonstrated that although 94% satisfied the diagnostic criteria for PTSD, only 47% of the same subjects studied met the criteria for PTSD 3 months after the assault [51]. Grace et al. [52] found that approximately one-third of those who developed a PTSD after a natural disaster continued to have significant symptoms 14 years later. Similarly, Kulka et al. [43] found that 15% of Vietnam Veterans continued to have a diagnosable syndrome 19 years after the end of the war. Thus, with the passage of time, a significant percentage of patients' symptoms tend to subside.
The above studies suggest that exposure to a trauma does not provide a sufficient explanation for the development of the chronic syndrome present more than 5 years after the exposure to the event. Therefore, it is reasonable to question what proportion of the treatment process for those with chronic PTSD should be focused on issues relating to the stressor and what else should be addressed. It may be that, although the trauma has activated other aetiological variables, modification of the cognitive and affective representations of the trauma will not necessarily neutralise their pathogenic influence. Furthermore, the more time that has elapsed since the original trauma, the more it is that subsequent events have shaped the significance and impact of the initiating event.
Given the diminished importance of the role of the stressor in producing long-term symptoms [53,54], it may be anticipated that efficacious therapeutic interventions are those that focus on a range of variables as well as the trauma exposure. These factors include: vulnerability factors, the occurrence of events subsequent to the focal trauma, the interpersonal disruption caused by the withdrawal, numbing and hyperarousal, as well as the disruption caused by the ‘retraumatising’ effect of the illness itself. This is not advocating a return to the more traditional perspective, however, of emphasising the relevance of earlier developmental events to subsequent responses to trauma and minimising the importance of the focal trauma, including a history of prior traumatisation. Rather, the role of the trauma in producing an individual's symptoms would optimally be explored in the context of the relative sensitivity or resiliency of the individual to the focal trauma. Such an assessment would consider the nature of the trauma, and the amount of time that has elapsed since the focal trauma, and inquire about subsequent stressful events. The more severe patterns of adult psychopathology appear to be linked to severe child abuse and neglect [13], rather than the normal demands of development, and these may also need to be the specific focus of attention.
There is also a need to examine, in cases of repeated traumatisation, the extent to which the individual developed a series of adaptive mental states (e.g. dissociation). It may be that the triggering of these mental states by day-to-day affective environmental responses that may be the critical element of the patient's current distress and disability. Being able to modulate this dissociative absorption [55] would have substantial influence on their ability to tolerate intense affect generated by trauma-related memories, and hence would require an examination of supplemental treatment methods.
Because the natural history of the disease appears to be one in which symptoms dissipate in most individuals, it becomes particularly interesting to determine the course of illness in those whose symptoms do not abate [56]. Data regarding the longitudinal course of PTSD are also critical to the conceptualisation of treatment, because they describe the fact that the symptoms of PTSD develop, progress, and worsen over time, raising the possibility that certain treatments may be particularly effective or ineffective depending on the particular stage of the illness.
One of the first studies to systematically evaluate the longitudinal course of PTSD was an examination of 303 non-treatment seeking disaster victims who were followed from 4 months after the disaster until 42 months posttrauma [57]. This study demonstrated a stepwise progression of symptoms from intrusive symptoms to disturbed arousal and avoidance. Using path analysis, a model was generated based on the raw data which described the emergence of symptoms and their interaction with time. Specifically, the model showed that traumatic events only had an indirect link with the arousal via the intensity of the intrusive phenomena. In turn, the avoidance symptoms were only directly related to intrusion. This model has subsequently been confirmed in another group of disaster victims [58]. However, the formative process leading up to this progression may be more complex, as suggested by more recent observations following individuals from the time of exposure [59].
Longitudinal modelling of symptom formation and development of the type described above is essential in trying to estimate which symptoms may require intervention at specific times even though the clinical assessment would likely reveal a more stable conglomeration of symptoms from all three clusters: intrusion, avoidance and arousal [60]. Such knowledge has direct relevance in focusing interventions. For example, a patient with very high levels of avoidance may be unlikely to accept the suggestion of a cognitive–behavioural therapy and similarly may not readily welcome the invitation to talk about their experiences. Thus, the initial management may need to focus on methods of anxiety control, whether this be with a variety of non-specific psychological treatments such as relaxation or the use of medication.
The possibility that the efficacy of different treatment modalities for PTSD may depend on the particular stage of the illness is supported by studies of treatment outcome. For example, Foa et al. [38] compared stress inoculation training, prolonged imaginal exposure, supportive counselling, and waitlist control in 45 female rape victims with PTSD. This study demonstrated a differential effect at immediate follow up and again at the 4-month follow up using the three treatments. Initially, stress inoculation therapy was superior, followed by imaginal exposure. By 4 months however, there was a trend to suggest that imaginal exposure appeared to have an advantage over stress inoculation. If there are differential effects of therapeutic modalities within a 4 month time frame, it is likely that there would be differential effects over longer time spans. Furthermore, it may be that certain forms of therapy might be associated with negative outcomes at particular stages of the illness. For example, exposure therapy using ‘flooding’ techniques have been found to worsen the symptoms of some patients, particularly in those in whom the focal trauma was decades earlier [61]. This empirical finding is consistent with Sargant and Slater's [62] clinical observations that abreaction is a treatment that is most effective early in the course of the illness, and its effectiveness decreases over time.
The differential effects of a treatment as a function of stage of illness might be particularly relevant to the psychopharmacology of PTSD. For example, Post [63] has postulated that there are a series of biological changes which emerge in the aftermath of exposure to traumatic stress. Preclinical studies exploring the phenomenon of kindled seizures have demonstrated that there are specific phases following electrical stimulation of the brain in rats during which a pharmacological intervention may be efficacious in preventing kindled seizures, and certain phases where such treatments would not work [64]. It may be the case that the symptoms of PTSD would respond, or not respond, to a certain medication based on the particular phase in which that symptom occurs in the longitudinal chain of the illness. This theory is further supported by recent observations that different medications appear to affect specific symptom clusters in PTSD [65]. Indeed, it is reasonable to hypothesise the presence of concomitant longitudinal neurobiological changes that give rise to, or accompany, the developmental changes in symptom formation.
In the absence of definitive knowledge of the factors that give rise to a more chronic course of PTSD, it might be suggested that as the amount of time following the traumatic event is increased, the syndrome will become more complex and multitextured and may require a more multidimensional treatment approach to target the array of issues that may have accrued. A specific consideration in regard to evaluating the complexity of the PTSD with time is the fact that there is an unusually high rate of psychiatric comorbidity, particularly of mood and anxiety disorders, substance abuse and character pathology, in patients with chronic PTSD [18,66]. These comorbid conditions have been conceptualised as occurring as either secondary adaptations to the chronicity of posttraumatic symptoms, or as reflecting a more complex syndrome. Regardless, these patients are likely to have a worse long-term outcome which may complicate the possible effectiveness of specific trauma-focused interventions, or require additional consideration.
The process of symptom formation and its implications for early intervention
An important issue is an understanding of how symptoms develop in the immediate aftermath of a trauma and progress into more chronic forms of PTSD [67]. Such an examination provides the key to understanding not only the normative versus abnormal nature of this syndrome, but also the appropriateness of current treatment approaches. Implicit in such an investigation would be a determination of whether there are different subtypes of acute reactions to trauma that might be particularly associated with the subsequent development of a more chronic condition. This is a possibility that has thus far not been explored in longitudinal studies which follow victims over a period of years rather than months. In particular, in some populations there may be less of a relationship between the acute stress response and PTSD as it appears that there are many individuals who develop PTSD despite having apparently coped at the time of the trauma [68,69]. This does not negate the importance of the finding that acute stress disorder after car accidents is a major risk factor for PTSD [70].
Current formulations of PTSD essentially posit that PTSD represents a prolonged, but essentially a normative, stress response. These formulations are based on the original suggestions of Horowitz [7] who proposed that there is a simultaneous emergence of the intrusion, avoidance and arousal symptoms, and that there is a process of oscillation between the states of intrusion and avoidance as individuals struggle to process overwhelming trauma. Although Horowitz's clinical observations were made based on the retrospective descriptions of a treatment-seeking sample with chronic PTSD, and his assumptions have not been borne out by recent studies [58,71] this model continues to have substantial influence on theoretical conceptions of PTSD and its treatment.
An acknowledgement of the above formulation is in the appearance in the DSM-IV called ‘acute stress response’. This diagnosis was included in the DSM-IV in an attempt to differentiate between short-term and long-term responses to trauma [60]. Because the qualitative nature of the acute and long-term responses are essentially the same, it is implicit in this formulation that PTSD is an illness that is defined by the lack of resolution of an acute stress response (e.g. as in bereavement).
The idea that PTSD reflects a prolonged response to stress has had a significant impact on current treatment formulations, but, in particular, has been the major impetus for early preventive interventions. However, in recent years the effectiveness of early treatment interventions has been called into question [72,73]. The few controlled studies that have examined the preventative effect of debriefing immediately following exposure to a traumatic event have suggested that, if anything, there is a poorer outcome following debriefing as compared with no intervention. For example, Kenardy et al. [74] reported that individuals who were not debriefed following the Newcastle Earthquake over a 2 year period showed a more rapid reduction in symptoms. Although preventative interventions such as debriefing are not the same as specialised PTSD treatments, it appears from the above studies that focusing on developing a trauma narrative and identifying the associated affects does not mitigate the development of a more chronic illness. In contrast, a focused treatment in those with an acute stress disorder does appear to stop the progression to PTSD in the majority of cases [40].
It should be mentioned that traumatised individuals who undergo debriefing and other treatments for acute stress responses subjectively report the interventions to be helpful [75]. Moreover, in the case of acute combat stress reactions, immediate treatment in the region of the battlefront resulted in a significant increase in rates of ability to return to combat (e.g. short-term symptom and behavioural improvement), despite the fact that many of those successfully treated for their acute stress reactions actually developed PTSD [68].
The questionable efficacy of immediate interventions in preventing the emergence of PTSD can be interpreted in several ways. First, the response that is being modified during the acute phase may not be a precursor of PTSD. Second, short-term responses to trauma may be heterogeneous in nature, and not necessarily ‘normative’ in all instances. As such, preventative short-term interventions may be beneficial for only a subset of individuals. In individuals who may be showing a normative stress response that would subside with time, interference may actually be harmful. Third, it may be that individuals who are at risk for the development of PTSD show an abnormal acute response to trauma that is actually worsened by interventions targeted in alleviating symptoms that are normative.
These issues can be clarified by more sophisticated observations about the range of acute stress responses and their concomitant biological characteristics at the time of the trauma followed by prospective observation. One such study was recently conducted by Resnick et al. [76]. In this study women were evaluated in the emergency room within hours after having undergone rape, and followed up for 3 months. The results showed that women with a prior history of rape and assault had lower cortisol levels in response to the trauma of rape. These women were significantly more likely to develop PTSD than women without a prior assault history who showed a more normative cortisol response to rape. Studies such as these are important in that they document the presence of heterogeneity of the acute stress response, describe the factors that can lead to heterogeneity in the initial response to trauma, and assess the effects of such responses in predicting the subsequent development of PTSD. Similarly, it appears that individuals who go on to develop a PTSD 6 months after a motor vehicle accident have a lower cortisol rise at the time of the trauma [77].
These data suggest that it may be appropriate to explore whether a maladaptive process which will subsequently develop into PTSD occurs immediately following a trauma, versus a process in which the illness is defined by the lack of resolution of an acute stress reaction (e.g. as in bereavement). Current concepts about posttraumatic treatment do not appear to deal with the transition of symptoms from normative to maladaptive responses [30]. However, if the determinants of a chronic maladaptive response to stress can be dissociated from the acute normative responses to a trauma, this represents a challenge to the prevailing conceptions that see chronic symptoms as a continuation of an acute response. The acceptance of the critical assumption, that the response to trauma is essentially a normative one, may be the most fundamental conceptual issue which needs to be considered in the evaluation and development of treatment strategies in PTSD.
Application of treatment in clinical settings
In addition to addressing issues concerning the complex nature of PTSD, an evaluation of the appropriateness of specific PTSD treatments and the understanding of when they are optimally employed requires an understanding of the variability among individuals who request treatment following a trauma.
Theoretically, it would be expected that the majority of people who seek treatment for PTSD are aware that they have been adversely affected by an environmental event as evidenced by the presence of symptoms such as intrusive thoughts, anxiety, sleep disturbances and nightmares and, ultimately, an impairment in social or occupational functioning. Accordingly, such individuals would be seeking relief from the distressing symptoms of PTSD and a restoration of their level of functioning. Typically, individuals who experience intrusive symptoms often have difficulty participating in their lives because day-to-day experiences become triggers. The focal trauma dominates their perception. Thus, these are the individuals who might best benefit from specific therapies that are targeted towards working through the trauma and, ultimately, symptom relief. On the other hand, many trauma survivors seek to repair the disruption of relationships due to interpersonal estrangement. In these cases, it is unclear whether focusing on the traumatic event would be the most effective course of action. In reality, it is only a minority of patients who present with such a direct agenda. Many present for assessment of a variety of health complaints such as somatic symptoms, depression or interpersonal difficulties. This sense of confusion and uncertainty is an important issue to clarify and address with the patient.
For a group of patients, symptom reduction may not be the reason for the clinical presentation or the desired goal of individuals seeking treatment for PTSD. For example, some trauma survivors may present for specialised PTSD treatment for symptoms that are not directly related to their having experienced a traumatic event, such as substance abuse, suicidal behaviour, a posttraumatic mood or personality disorder. In a minority, there may be a comorbid primary psychiatric disorder that is exacerbated by exposure to single or multiple traumatic events. Other individuals who may have been exposed to a major traumatic event in the past, may present for treatment following a minor life stress without acknowledgement of the role the focal trauma in contrast to their more current difficulties. There is a small group of traumatised individuals who may seek treatment for PTSD even though they do not wish to rid themselves of their PTSD symptoms, but present for treatment to validate and reify their status as victims. Finally, some individuals may see PTSD treatment as a prerequisite for obtaining compensation, and may be resistant to treatment that might restore their occupational functioning. The clinical issues raised by the fact of these patient subgroups are not insurmountable treatment problems; rather, the diverseness of the clinical treatment presentations and agendas must be considered in selecting proper treatments and/or in evaluating the relative success or failure of these interventions.
The heterogeneity among treatment seekers described above has not been a consideration in studies that have evaluated treatment outcome, nor has it been particularly considered in descriptive or biological studies. However, it is easy to see how individuals fitting these different categories would be dramatically different on the variables that predict course of illness and therapeutic efficacy. Furthermore, a critical point that deserves consideration is the fact that individuals who seek treatment for PTSD, as heterogeneous as they are, appear to be a unique subset of trauma survivors [43]. It has been estimated that only a small percentage of individuals exposed to trauma seek treatment for their symptoms [78]. Thus, in trying to evaluate the conceptual origins of PTSD and the efficacy of specialised treatments, it is important to maintain an awareness of who has been studied. There is need to systematically evaluate all the issues that have been raised in this review with a consideration that clinical formulations of the response to trauma and its treatment may be true for some trauma survivors, but not others.
Conclusions and future directions
Most conceptions of the treatment of PTSD were made when knowledge of the aetiology, phenomenology and natural history of PTSD were in its infancy. As our understanding of PTSD evolves, it is imperative to re-examine the relevance of original treatment formulations and modify them based on the information obtained from the descriptive research literature about aetiology, phenomenology and epidemiology. For example, therapeutic approaches must consider the increasing recognition that the trauma is a necessary, but insufficient, cause of PTSD, and that a series of other factors serve to modify the response to trauma. As such, the current emphasis on working through the trauma might best be employed with the expectation that the more complex and chronic cases may not respond. Furthermore, given the emergence of symptoms over time and the fluidity of the chronic symptom patterns of PTSD, it is important to consider using different types of treatment interventions at different stages of the illness, and to critically explore the optimum window in the course of the illness in which to do trauma-focused work [62]. Related to this point, it is necessary to determine which of the acute stress reactions are the prodromal stages of the posttraumatic process, and whether these responses require distinct therapeutic interventions.
At the core of all these issues is the conceptual and methodological problem of determining the spectrum of normative versus anomalous responses to stress, and whether various gradations of stress responsiveness are amenable to similar interventions. The precise biological characterisation of these patterns of response may, for example, allow specific and focused pharmacological interventions. There are also a series of issues above and beyond those discussed above. First, there is a need to focus on the effect of treatment strategies on the different components of the disorder. For example, the acceptance of the trauma-related formulations discussed above, has meant that therapists have often worked with the implicit assumption that all the symptoms in PTSD are equally responsive to the chosen intervention. For example, data from some pharmacological studies have shown that medications may be particularly effective for some symptom clusters, whereas others remain refractory [33]. It may be, therefore, that the symptoms of PTSD exist along several orthogonal dimensions.
A unitary view of PTSD as the response to a traumatic event may result in an underestimation of the long-lasting and disabling quality of some aspects of the disorder. The better characterisations of these dimensions in descriptive research may provide some insights into the types of treatments that are likely to be efficacious. For example, we have identified that the disturbance of memory and concentration in PTSD is a source of prolonged disability even when many of the other symptoms of the disorder have gone into remission. The use of pharmacological agents that improve memory and concentration may therefore be of particular benefit as may the teaching of cognitive and behavioural strategies to manage memory disorders.
Second, there is a need to carefully consider whether different types of traumatic events are more likely to be amenable to the same treatment interventions. In so far as different types of traumatic event are associated with specific sequelae it is necessary to address potential differences in symptoms that stem directly from the discrete aspects of the trauma. For example, dissociation is a much more common response to child abuse than to a disaster, as are the features of complex PTSD which describes the more pervasive disturbance of personality seen in some trauma victims [6,79]. As such, treatment modalities must be adapted to fit these specific considerations. For example, although ultimately reworking and retrieving memories is an important component of treatment of an adult survivor of child abuse, this often needs to be delayed. If the individual is prone to dissociation, this state of mind will determine the way in which exposure therapies must proceed (e.g. premature exposure may provoke an intense dissociative response). Equally, their difficulties with affective modulation require specific attention in treatment. Furthermore, in addition to considering the type of trauma that has induced PTSD, there must also be special consideration to the issue of multiple trauma and the impact of sensitisation to lower grade traumatic and non-traumatic stressors.
In conclusion, the future developments in the treatment and conceptualisation of PTSD depend on a healthy dialectic between the treatment and descriptive literature. This will assist in the development of a better understanding of the components of the disorder which require consideration in the design of treatment interventions. A more precise characterisation of the nature and range of the stress responses in trauma victims has the potential to lead to significant improvements in the effectiveness of the treatment of victims of trauma.