
Abstract
Study Design
Systematic review.
Objectives
To determine the incidence of catastrophic cervical spine injuries (CCSIs) among elite athletes participating in contact team sports and whether the incidence varies depending on the use of protective gear or by player position.
Methods
Electronic databases and reference lists of key articles published from January 1, 2000, to January 29, 2016, were searched.
Results
Fourteen studies were included that reported CCSI in rugby (n = 10), American football (n = 3), and Irish hurling (n = 1). Among Rugby Union players, incidence of CCSI was 4.1 per 100,000 player-hours. Among National Football League players, the CCSI rate was 0.6 per 100,000 player-exposures. At the collegiate level, the CCSI rate ranged from 1.1 to 4.7 per 100,000 player-years. Mixed populations of elite and recreational rugby players in four studies report a CCSI rate of 1.4 to 7.2 per 100,000 player-years. In this same population, the scrum accounted for 30 to 51% of total reported CCSIs in Rugby Union versus 0 to 4% in Rugby League. The tackle accounted for 29 to 39% of injuries in Rugby Union and 78 to 100% of injuries in Rugby League. Making a tackle was responsible for 29 to 80% of injuries in American football.
Conclusion
CCSIs are infrequent among elite athletes. There is insufficient evidence to determine the effect of protective gear (e.g., helmets, padding) on CCSI incidence. Scrum and tackle in rugby and tackling in American football account for the majority of CCSIs in each respective sport.
Introduction
A catastrophe creates serious and usually sudden damage or suffering. In the context of the cervical spine in elite contact sports, a catastrophe equates to the risk of significant neurologic injury. The consequences of such an injury are vast, with great personal and financial cost.
Elite contact sports represent a significant business. Players strive to defeat their opponents by skill, strength, and sometimes skullduggery. Within this gladiatorial arena, there comes risk. The training of the players by the coaches, the setting of the rules under inclusion of protective gear by the governing bodies, and the conduct during the game controlled by the referees all serve to reduce injury risk. However, risk cannot be totally eliminated. Natural concerns around the occurrence of such injuries in contact sport have led to calls for the safety of such sports to be improved. In Rugby Union, the Sports Collision Injury Collective—an international group of academics—has recently called for rugby to become a noncontact sport in the under-18 age group. 1
In general, contact sporting events are the fourth most common cause of spinal cord injury in the United States (behind motor vehicle accidents, violence, and falls) and account for ∼9% of the total injuries in 2014. 2 Around the world, sporting accidents account for 3 to 28% of spinal cord injuries. 3 The popularity and type of contact sports played around the world varies enormously.
Hence, to better understand the magnitude of catastrophic cervical injury among elite athletes participating in contact sport, we sought to answer the following questions:
What is the incidence of catastrophic cervical spine injuries (CCSIs) among elite athletes participating in contact team sports?
Does the incidence vary depending on whether the elite athlete is protected (shoulder pads and or helmet) or unprotected?
Within a sport, does the incidence vary by positional activity?
Materials and Methods
Results
Study Characteristics
We identified 14 studies among 16 publications meeting the inclusion criteria (Fig. 1). A list of excluded articles can be found in the online
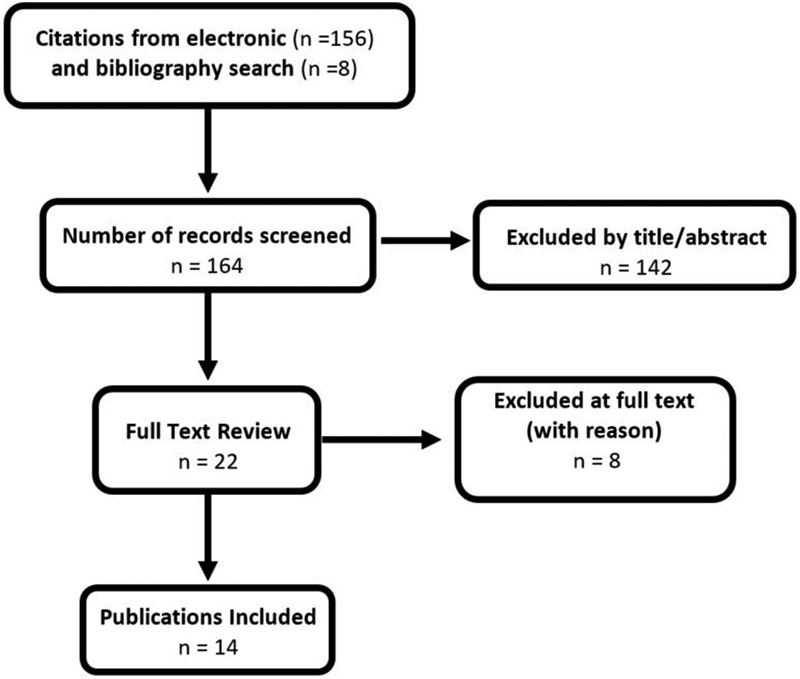
Flow diagram showing results of literature search.
Characteristics of included studies
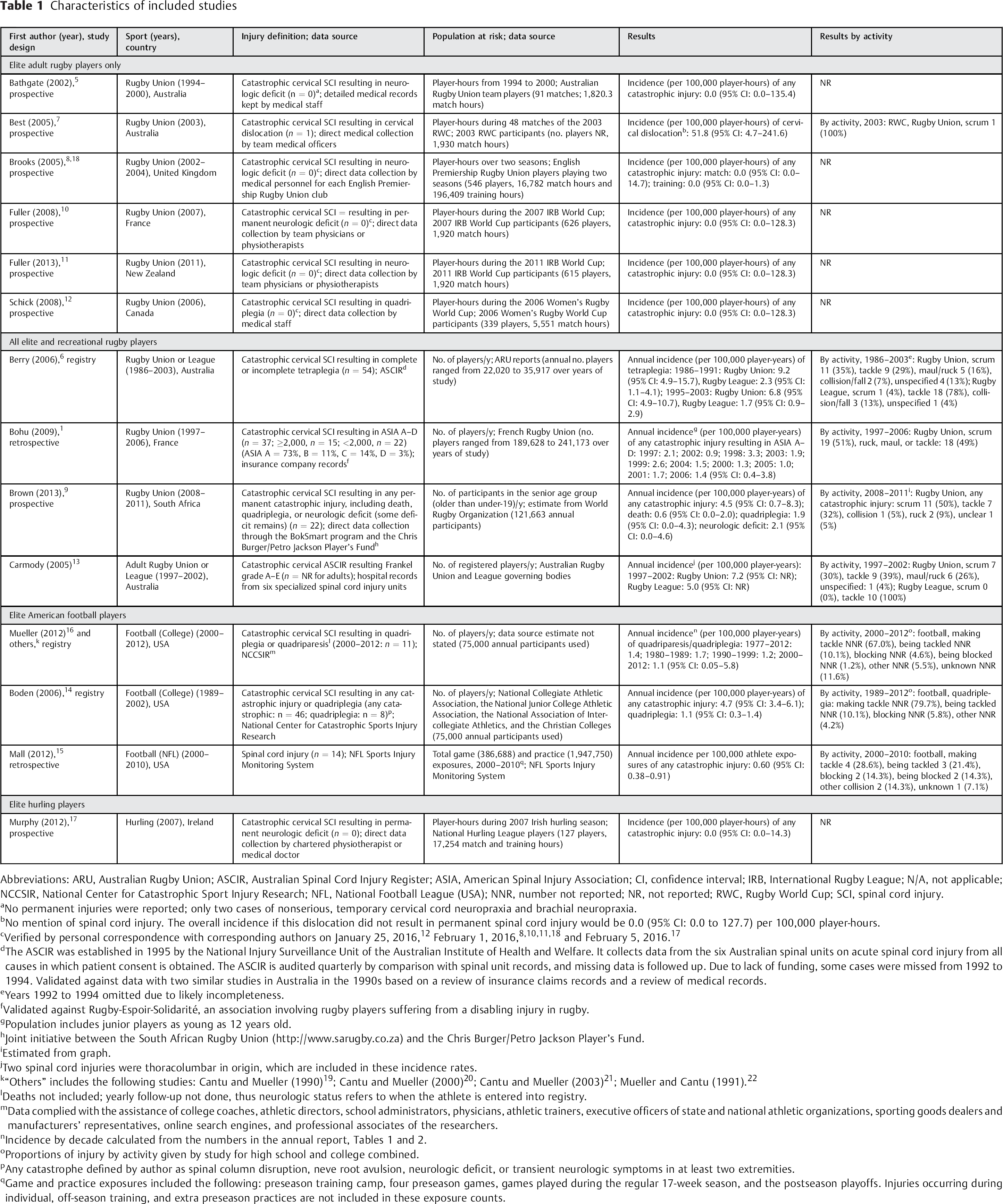
Abbreviations: ARU, Australian Rugby Union; ASCIR, Australian Spinal Cord Injury Register; ASIA, American Spinal Injury Association; CI, confidence interval; IRB, International Rugby League; N/A, not applicable; NCCSIR, National Center for Catastrophic Sport Injury Research; NFL, National Football League (USA); NNR, number not reported; NR, not reported; RWC, Rugby World Cup; SCI, spinal cord injury.
No permanent injuries were reported; only two cases of nonserious, temporary cervical cord neuropraxia and brachial neuropraxia.
No mention of spinal cord injury. The overall incidence if this dislocation did not result in permanent spinal cord injury would be 0.0 (95% CI: 0.0 to 127.7) per 100,000 player-hours.
Verified by personal correspondence with corresponding authors on January 25, 2016, 12 February 1, 2016, 8 , 10 , 11 , 18 and February 5, 2016. 17
The ASCIR was established in 1995 by the National Injury Surveillance Unit of the Australian Institute of Health and Welfare. It collects data from the six Australian spinal units on acute spinal cord injury from all causes in which patient consent is obtained. The ASCIR is audited quarterly by comparison with spinal unit records, and missing data is followed up. Due to lack of funding, some cases were missed from 1992 to 1994. Validated against data with two similar studies in Australia in the 1990s based on a review of insurance claims records and a review of medical records.
Years 1992 to 1994 omitted due to likely incompleteness.
Validated against Rugby-Espoir-Solidarité, an association involving rugby players suffering from a disabling injury in rugby.
Population includes junior players as young as 12 years old.
Joint initiative between the South African Rugby Union (http://www.sarugby.co.za) and the Chris Burger/Petro Jackson Player's Fund.
Estimated from graph.
Two spinal cord injuries were thoracolumbar in origin, which are included in these incidence rates.
“Others” includes the following studies: Cantu and Mueller (1990) 19 ; Cantu and Mueller (2000) 20 ; Cantu and Mueller (2003) 21 ; Mueller and Cantu (1991). 22
Deaths not included; yearly follow-up not done, thus neurologic status refers to when the athlete is entered into registry.
Data complied with the assistance of college coaches, athletic directors, school administrators, physicians, athletic trainers, executive officers of state and national athletic organizations, sporting goods dealers and manufacturers’ representatives, online search engines, and professional associates of the researchers.
Proportions of injury by activity given by study for high school and college combined.
Any catastrophe defined by author as spinal column disruption, neve root avulsion, neurologic deficit, or transient neurologic symptoms in at least two extremities.
Game and practice exposures included the following: preseason training camp, four preseason games, games played during the regular 17-week season, and the postseason playoffs. Injuries occurring during individual, off-season training, and extra preseason practices are not included in these exposure counts.
Incidence Rate of Catastrophic Cervical Spine Injury
Five studies evaluated catastrophic spine injuries based on time at risk for injury during match competition in male elite Rugby Union players during World Cup or season match play (Table 2). 5 , 7 , 8 , 10 , 11 , 18 There was only one cervical dislocation reported in 24,372 player-hours. There was no indication as to whether the cervical dislocation resulted in permanent spine injury. Assuming the case resulted in a CCSI, the incidence rate would be 4.1 per 100,000 player-hours (95% CI: 0.4 to 19.1). If no permanent spine injury resulted from the dislocation, the 95% CI would be 0.0 to 10.1 per 100,000 player-hours. One additional study reported no CCSI among elite female rugby players at a World Cup event (injury rate 0.0; 95% CI: 0 to 128 per 100,000 player-hours). 12
Three studies evaluated CCSI in American football, one at the professional level (National Football League [NFL]) 15 and two at the collegiate level. 14 , 16 The incidence of CCSI in the NFL was reported as 0.6 per 100,000 player-exposures (95% CI: 0.4 to 0.9) where a player-exposure represented a session at the preseason training camp or a regular or postseason game. At the collegiate level, the CCSI rate ranged from 1.1 to 4.7 per 100,000 players per year.
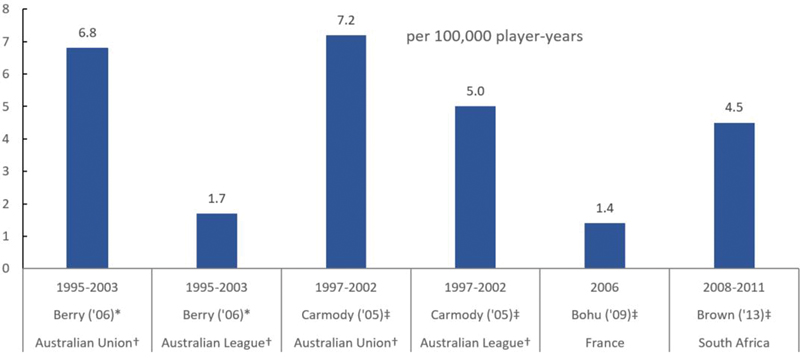
Four studies used annual counts in the denominator from mixed populations of elite and recreational rugby players from Australia, 6 , 13 France, 1 and South Africa 9 (Fig. 2). The incidence varied between 1.4 and 7.2 per 100,000 player-years. Berry et al compared the injury rate between Australian Union and League players and found a fourfold increase in the rate of tetraplegia comparing Union with League players (schoolboy and adult elite and recreational players combined), 6.8 versus 1.7 per 100,000 player-years (rate ratio, 4.0; 95% CI: 1.8 to 9.2). 6 The difference in CCSI rates between Union and League players in a second study of adult elite and recreational rugby players was smaller, 7.2 versus 5.0 per 100,000 player-years (rate ratio, 1.44; 95% CI not reported).
There were no CCSIs in one small study in hurling. 17
Incidence rate of catastrophic cervical spine injury among elite Rugby Union players during match play
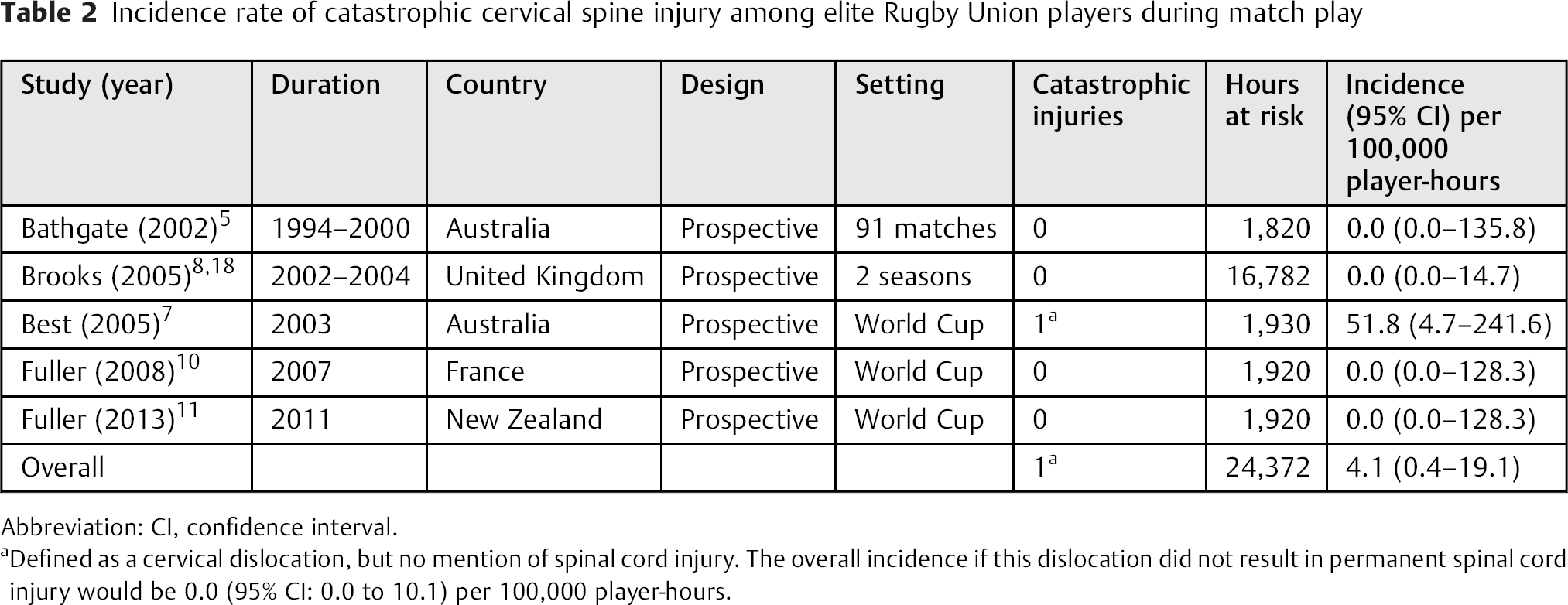
Abbreviation: CI, confidence interval.
Defined as a cervical dislocation, but no mention of spinal cord injury. The overall incidence if this dislocation did not result in permanent spinal cord injury would be 0.0 (95% CI: 0.0 to 10.1) per 100,000 player-hours.
Incidence risk of catastrophic cervical spine injury in a mixed population of elite and recreational rugby players.
Game Activity Associated with Injury
Two studies in Rugby Union 1 , 9 and two studies looking at both Rugby Union and Rugby League 6 , 13 identified the game activity in which each injury occurred (Table 3). Both studies included elite and recreational athletes. In Rugby Union, scrum accounted for 35 to 51% of total reported CCSIs among three studies, which is in sharp contrast to Rugby League, where only 1 CCSI occurred during the scrum across two studies. 6 , 13 Scrum was followed by tackle, which accounted for 29 to 32% of injuries in Rugby Union and 78 to 100% of injuries in Rugby League; then by maul or ruck, which accounted for 9 to 16% of injuries in Rugby Union; then collision or fall, which caused 5 to 7% of injuries in Rugby Union and up to 13% of injuries in Rugby League.
One study in professional football 15 and two studies in American high school or college football 14 , 16 , 19 , 20 , 21 , 22 reported the proportions of CCSI by activity (Table 4). Making a tackle was responsible for 67 to 80% of injuries, followed by being tackled (10%), blocking (5 to 6%), and being blocked (1%). Other activities accounted for 4 to 6% of injuries, and 12% of injuries were indeterminate in origin.
Proportion of catastrophic cervical spine injuries in a mixed population of elite and recreational rugby players by rugby activity
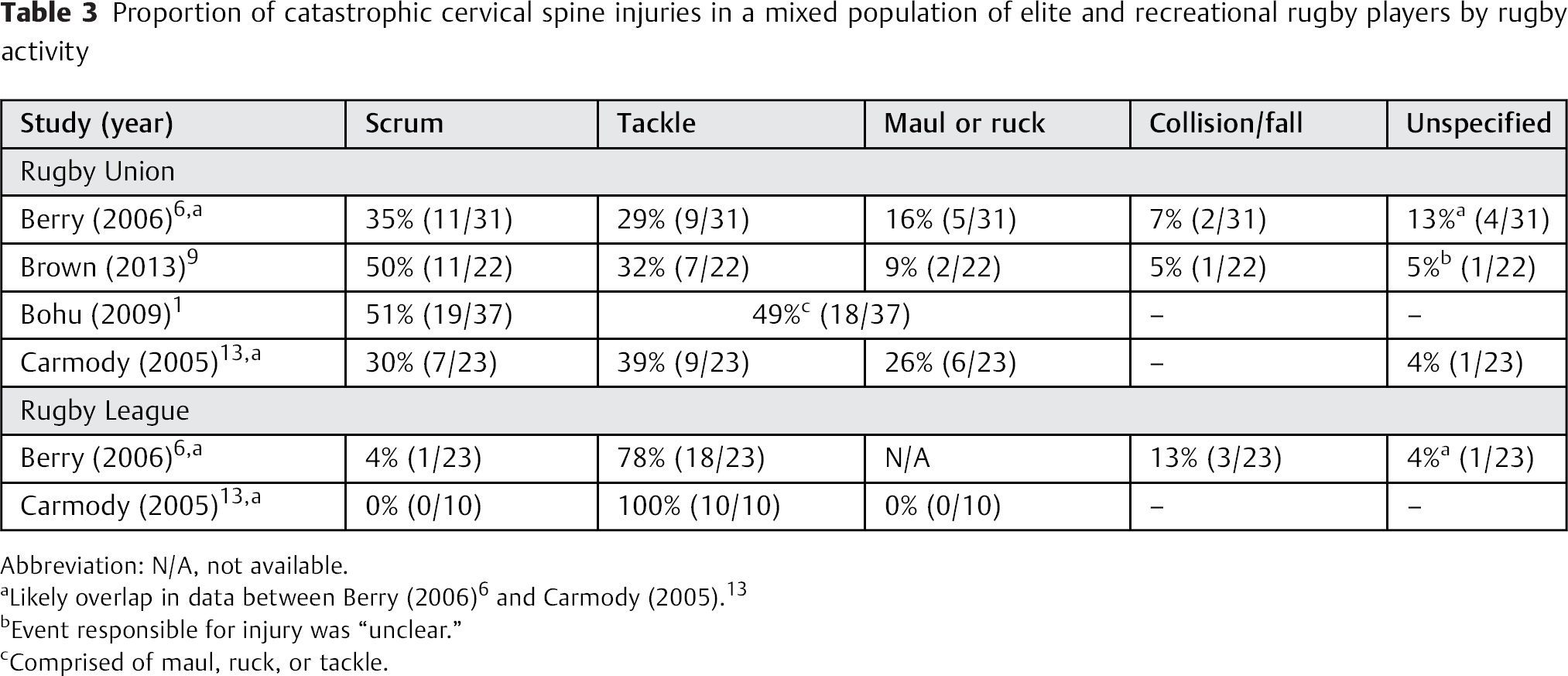
Abbreviation: N/A, not available.
Event responsible for injury was “unclear.”
Comprised of maul, ruck, or tackle.
Proportion of catastrophic cervical spine injuries among American football players by activity

Influence of Protection on Incidence of Catastrophic Cervical Spine Injury
No studies were identified evaluating the influence of protective gear (e.g., shoulder pads, helmets) on the incidence of CCSI.
Evidence Summary
CCSIs are infrequent among athletes participating in elite-level contact team sports (Table 5). There is moderate evidence that the rate among elite Rugby Union players is 4.1 per 100,000 player-hours (95% CI: 0.4 to 19.1); among professional American football players (NFL), 0.6 per 100,000 player-hours (95% CI: 0.4 to 0.9); and among collegiate American football players, from 1.1 to 4.7 per 100,000 player-years. Among a mixed population of elite and recreational rugby players, there is low evidence that the rate ranges from 1.4 to 7.2 per 100,000 player-years among Rugby Union and 1.7 to 5.0 per 100,000 player-years for Rugby League. There are no studies directly evaluating the influence of protective gear on the incidence rate of catastrophic cervical injury. Scrum and tackle account for most of the CCSIs in Rugby Union play, tackle in Rugby League play, and making a tackle in collegiate American football. However, the evidence in determining the rate estimates by activity is low.
Quality of evidence evaluating catastrophic cervical spine injuries
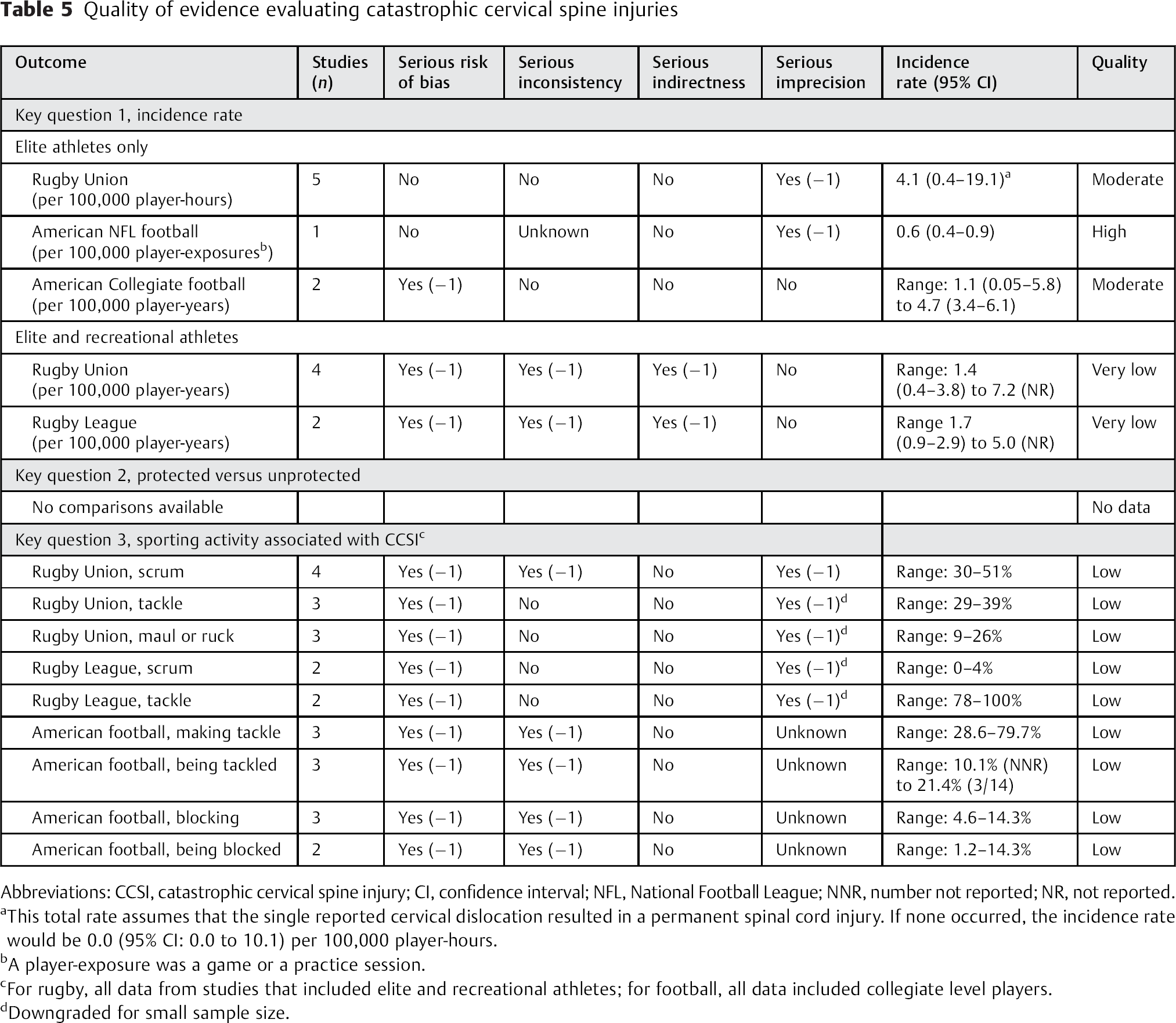
Abbreviations: CCSI, catastrophic cervical spine injury; CI, confidence interval; NFL, National Football League; NNR, number not reported; NR, not reported.
This total rate assumes that the single reported cervical dislocation resulted in a permanent spinal cord injury. If none occurred, the incidence rate would be 0.0 (95% CI: 0.0 to 10.1) per 100,000 player-hours.
A player-exposure was a game or a practice session.
For rugby, all data from studies that included elite and recreational athletes; for football, all data included collegiate level players.
Downgraded for small sample size.
Illustrative Case
American Football
A 19-year-old Division II collegiate defensive back was injured during a practice tackling drill. He had immediate onset of C6 quadriplegia. His injury radiograph revealed a fracture dislocation of the C5–C6 level (Fig. 3). The lateral computed tomography scan at the time of injury showed significant compromise of the spinal canal (Fig. 4). The immediate postoperative lateral radiograph revealed good realignment and fixation of the C5–C6 fracture dislocation (Fig. 5). However, postoperative T1-weighted magnetic resonance imaging (MRI) revealed significant cord injury at the level of the fracture dislocation, and the T2-weighted MRI image revealed injury to the cord extending from C4 to C7 (Figs. 6 and 7). The lateral cervical radiograph 1 year postoperatively revealed good healing. At that time, he was functioning as a C7-level quadriplegic (Fig. 8).
Radiograph revealed a fracture dislocation of the C5-C6 level.
Lateral computed tomography scan at the time of injury showed significant compromise of the spinal canal.
Immediate postoperative lateral radiograph reveals good realignment and fixation of the C5-C6 fracture dislocation.
T1-weighted magnetic resonance image (MRI) postoperatively reveals significant cord injury at the level of the fracture dislocation.
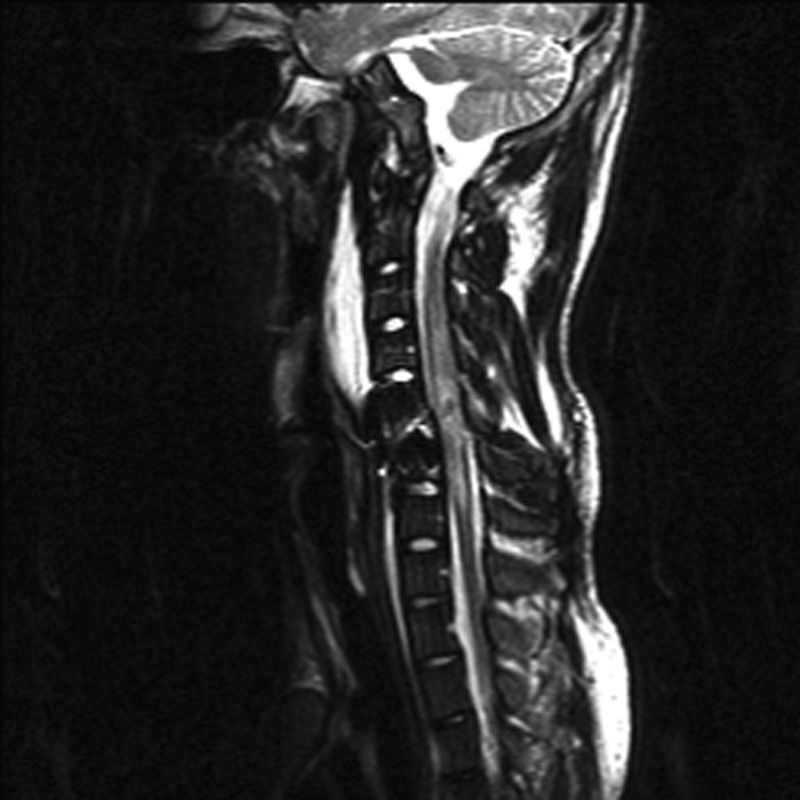
T2-weighted MRI reveals injury to the cord extending from C4 to C7.

Lateral cervical radiograph one year postoperatively reveals good healing.
Rugby
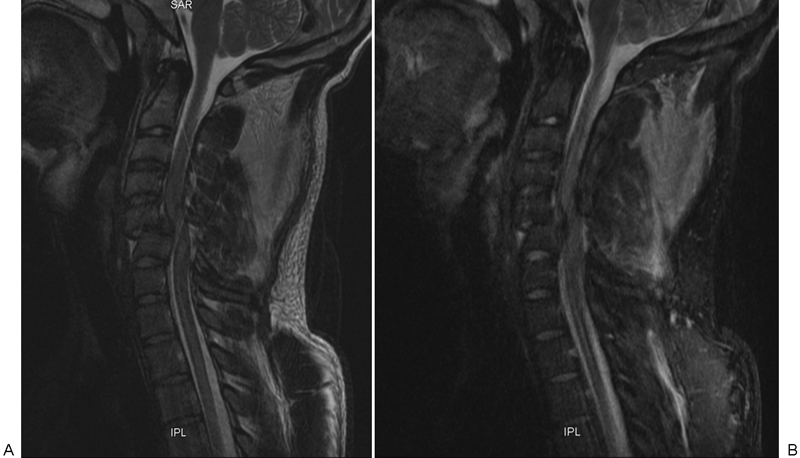
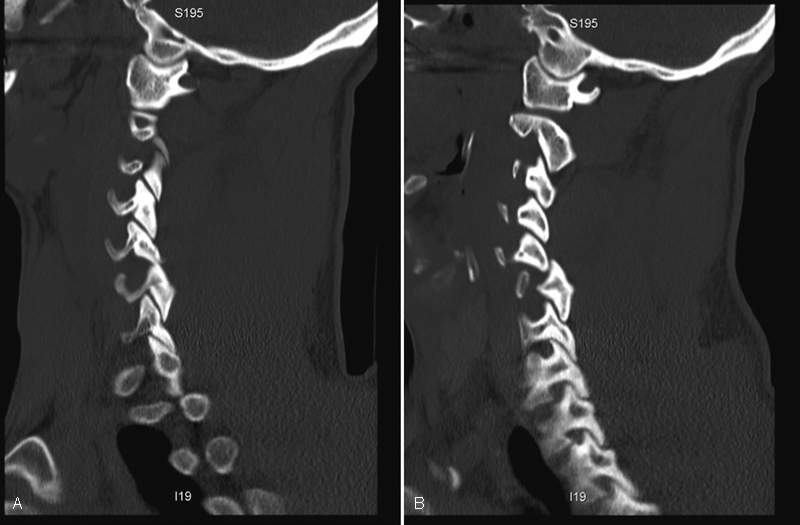
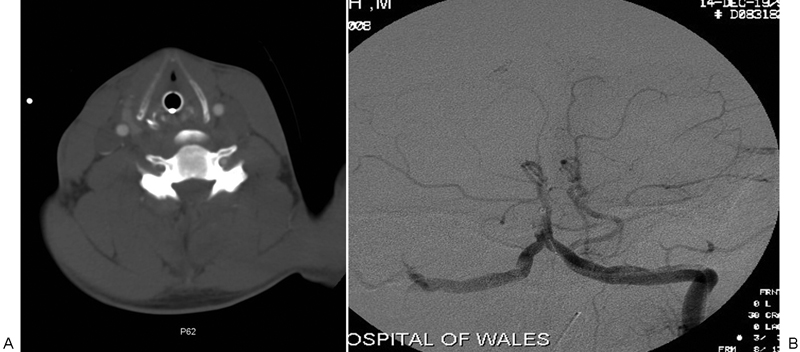
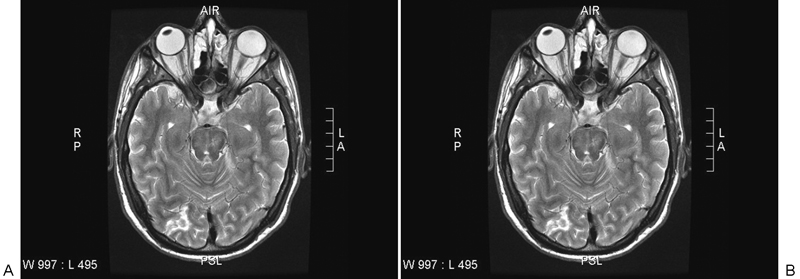
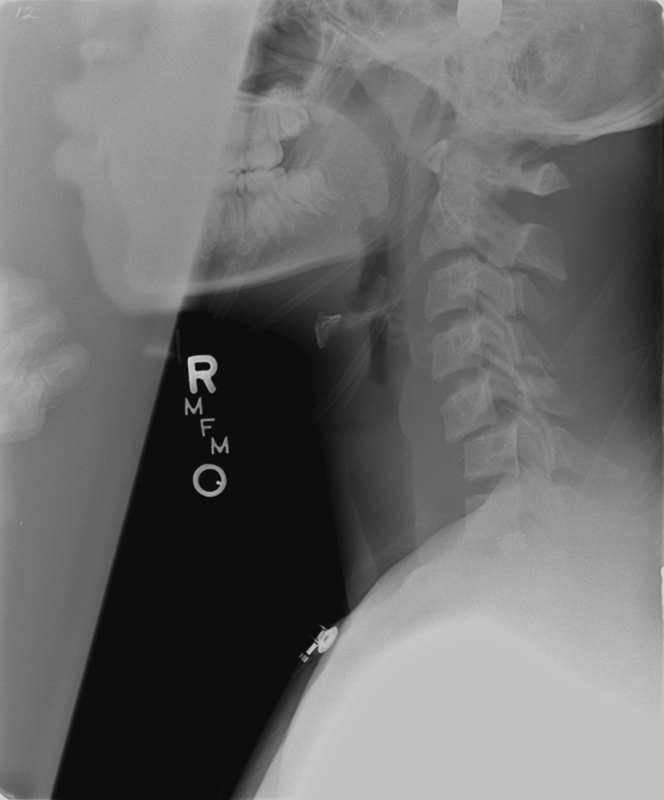
A 20-year-old professional premiership rugby player was bending down at ruck to pick up the ball at breakdown when the opposition forward came through and kneed him accidentally in the head while the head was in the flexed position. On examination, the patient was found to have a Glasgow Coma Scale rating of 15 with an American Spinal Injury Association Grade B status with a motor score of 8, but some lower extremity sensation. Imaging confirmed a bilateral C5–C6 facet dislocation (Figs. 9 10 11 12). After completion of the imaging tests and hemodynamic resuscitation, surgical reduction was planned for the next morning. The patient became increasingly obtunded during the night. Cranial MRI obtained overnight before the planned surgery showed infarcts in the cerebellum and posterior cortex of the right hemisphere (Fig. 13). Clinically the patient fell into a deep coma and despite critical care interventions never recovered brain function. He was declared brain-dead several days later without ever having received spine care.

Lateral cervical spine radiograph confirming bilateral C5–C6 facet dislocation.
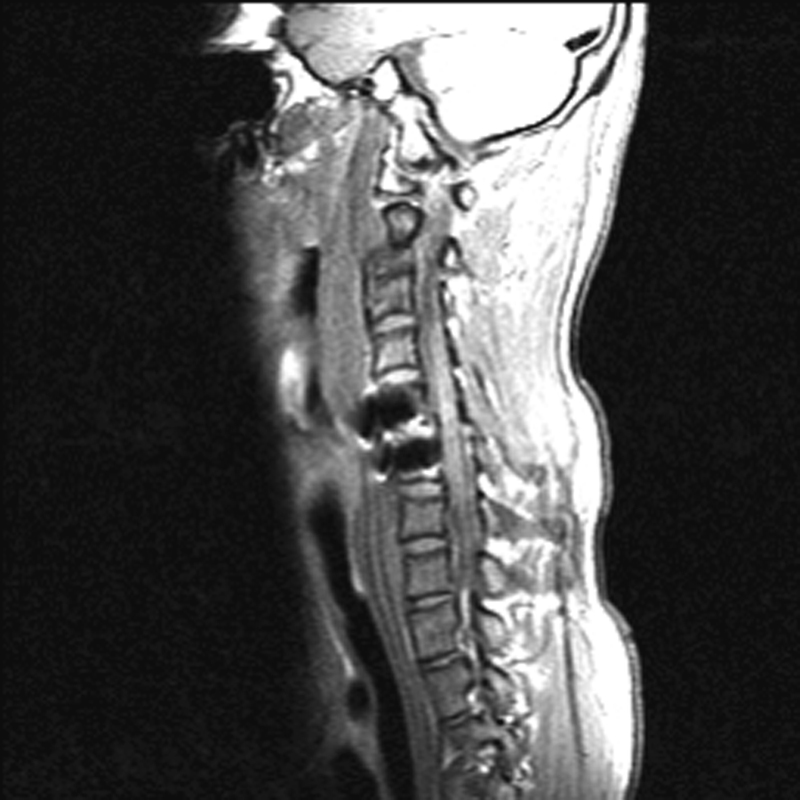
(A, B) A prereduction T2-weighted and short tau inversion recovery sequence magnetic resonance imaging with persistent C5–C6 dislocation leading to high-grade cord impingement with cord signal changes and extensive posterior ligamentous injury.
(A, B) Left- and right-sided parasagittal reformatted computed tomography scans confirm bilateral facet dislocation with a left-sided perched facet and a complete dislocation contralaterally.

(A, B) Axial computed tomography and an angiogram show an occluded right-sided vertebral artery from the C5 level rostrally.

(A, B) Cranial magnetic resonance imaging shows infarcts in cerebellum and posterior cortex of the right hemisphere.
Discussion
Recently, there has been an increased awareness for acute and cumulative head trauma relative to impact sports. The ill effects of repetitive concussive trauma on brain health and its potential association with disorders such as chronic traumatic encephalopathy are being investigated in an unprecedented manner for sports like American football and various forms of rugby, as well as soccer.
Despite occasional high-profile cervical spinal cord injuries in these particular sports, there has been no major systematic effort to explore the association of high-impact contact, elite-level sports with CCSIs considering variables such as sports type, position, or age group, nor a more detailed consideration of the effect of protective gear and rule changes on prevention or causation of serious cervical spine injuries. Given the proximity of the head and the cervical spine, experts have also started questioning the effect of head trauma on the cervical spine.
As a foundational study, an international panel of sports medicine and spine surgeon experts who deal with high-impact, elite-level contact sports from eight countries assessed the recent incidence of CCSI in these sports. In addition, the panel attempted to answer whether protective gear had an effect in either preventing or increasing catastrophic cervical injuries. Gear innovations can result in significant decreases in catastrophic injuries when used properly as exemplified by the mandated wear of the head and neck support (HANS) device for all drivers who participate in elite levels of motorsports such as the National Association for Stock Car Auto Racing (NASCAR) and Formula One. This HANS device locks the head to the body during impact. In the time HANS use has been mandated, there have been no deaths from skull base fractures. Similar results have also been seen with the use of omnidirectional suspension used in motorcycle and bicycle helmets to reduce risk of concussion. The NFL is interested in this technology for use in football helmets. 23 , 24 It is well known that protective gear may induce players to take more risky actions than they would without such equipment. Moreover, those wearing protective gear may use the defensively intended game wear as an offensive impact weapon. The assessment of player position could also allow for some inferences in this regard. In particular, the contrast of American football, with an ever-increasing emphasis on protective gear, and rugby (both Union and League), where protective gear is de minimis by intent, also invites a comparison to this end.
In American football, the antispearing rule was implemented in 1976, which outlawed making a tackle or block by leading with the head or face, essentially using the helmet as a weapon. The antispearing rule reduced the incidence of spine injuries from 20 per year during 1971 through 1975 to 7.2 per year after 1976, and it did not affect the play of the game. 21 Further attempts at inducing a culture change in American Football are currently underway with the Heads up Football campaign, 25 but these changes are too recent to allow for meaningful comparisons. Additional insight may be provided by comparing the very different rules governing Rugby League, with its more fluid game and absence of contested scrums (a lockup involving line players of either side during a restart of play from the field), to the more popular Rugby Union, with its strong emphasis on scrums and different rules regarding mauls (pushing the ball forward within a pile of players) and tackles.
This systematic review revealed that in elite contact team sports, the available body of evidence relating to catastrophic cervical spine literature is mostly limited to rugby and American football. Rugby was further subdivided into its two main rules formats, Rugby Union and Rugby League; for American football, only collegiate leagues organized by the National Collegiate Athletic Association (NCAA) offered prospectively gathered data. From the NFL, retrospective data is available only through the tightly controlled NFL Sports Injury Monitoring System.
Overall, one challenge of any attempt at studying CCSIs is the sporadic occurrence of these injuries in these sports. Although CCSI is devastating for the individuals and their families, rare occurrences like these pose formidable challenges to statistical assessment as they require strict adherence to data gathering and data interpretation.
We reported the rates of CCSI in a standardized format based on the data either as injuries per 100,000 players/y or injuries per 100,000 player-hours, when possible. In general, we found that collegiate-level American football had a similar CCSI rate (1.1 to 4.7 per 100,000 player-years) compared with a mixed population of elite and recreational athletes playing Rugby League (1.7 per 100,000 player-years). However, a mixed population of elite and recreational athletes playing Rugby Union sustained the highest injury rate (4.5 to 6.8 injuries per 100,000 player-years). We postulate that this result may be related to the contested scrum seen in Rugby Union, which has not been seen in Rugby League since 1997. 6 Rule changes have been implemented in Rugby Union as recently as the 2013–2014 season in an attempt to prevent this result, 26 but it remains to be seen if such laws have changed the incidence of catastrophic cervical spinal cord injury. It must be noted that comparing rates across sports needs to be done cautiously, as the exposure time for injury varies between sports. In general, a player-year represents a season, and rugby has more than twice as many games in a season than American football, and each player in rugby at an elite level is likely to see more on-field action than in American football with its alternating three specialized subunits.
Rugby has to date provided a far more detailed breakdown of specific activities that lead to CCSI compared with American football. Again, the impact of a game-specific element—here exemplified by the scrum in Rugby Union—persistently leads to a higher CCSI rate than in Rugby League. In contrast, Rugby League has a disproportionately higher rate of CCSI related to tackling than Rugby Union. This result again could be interpreted as an effect of the speed with which players in a more free-flowing game can impact and thus injure one another. This observation is underscored by the available retrospective NFL data showing that the act of tackling amounts to 50% of CCSI occurrences. Interestingly, a study with solid data gathering in another speed contact sport—the prehistoric Irish national sport of hurling (which is played with a cupped stick and ball)—has not reported any CCSI, likely due to the absence of open field tackling. The same unpublished observation was made in collegiate-level lacrosse.
In general, the data available for CCSI in contact sports allows for several observations:
With the current limited data available, the two preeminent contact team sports at risk for CCSI are American football and rugby (both Union and League formats).
Protective gear, such as that worn in American football, does not appear to be a preeminent factor in the occurrence of CCSI. However, a more detailed study needs to be done that includes the NFL.
Game-specific actions—such as the contested scrum and the ruck and maul in Rugby Union—persistently seem to be associated with a higher CCSI rate compared with other sports, including American football. Rule changes may lead to a desirable decrease in CCSI, but will alter the character of the game and may affect the public's interest.
Tackling in conjunction with open field speed maneuvers remains a leading threat for CCSI in all of these sports.
Despite the life-changing nature for those affected, CCSI remains surprisingly poorly studied by collegiate and professional American football in contrast to organized rugby, where transparent statistical data collection from high school, university, and national and international databases are the norm. Although relatively rare, the serious impact of CCSI on athletes would seemingly prompt systematic independent reporting of spine injuries associated with organized American football at all levels, including youth-level play, to become mandatory, analogous to currently surging efforts to combat traumatic brain injury. This requirement would finally also allow for a better understanding of the effects of the far more common, more subacute, and less severe neck injuries such as sprains, stingers, burners, minor fractures, cervical spondylosis-related disorders such as disk herniations and stenosis, as well as cord-related diseases such as myelopathy and other neurodegenerative spinal cord ailments.
Conclusions
Current evidence, consisting largely of low-quality studies, indicates CCSIs are infrequent among elite athletes in rugby and American football. The majority of the existing literature evaluates CCSI incidence in rugby athletes; more consistent, transparent, and independent data gathering and analysis are needed in other contact sports such as American football, ice hockey, soccer, and lacrosse.
There is insufficient evidence to determine the effect of protective gear (e.g., helmets, padding) on CCSI incidence.
Scrum and tackle in rugby and tackling in American football account for the majority of CCSIs in each respective sport.
More high-quality research, with standardization of injury definitions and reporting methods, is needed to accurately evaluate and compare CCSI incidence within and between sports.
Disclosures
Michael James Hutton: Personal fees (DePuy/Synthes); Nonfinancial support (Lindare Medical, NuVasive)
Robert A. McGuire: Other (President AO North America)
Robert Dunn: Fellowship/speaker stipend (Medtronic, DePuy/Synthes, AOSpine)
Richard Williams: none
Peter Robertson: Consulting (Medtronic, NuVasive)
Bruce Twaddle: none
Patrick Kiely: Nonfinancial support (DePuy/Synthes)
Andrew Clarke: none
Keyvan Mazda: none
Paul Davies: none
Krystle T. Pagarigan: none
Joseph R. Dettori: none
In the context of the recent highly publicized focus on head injuries in contact sports, the Evidence-Based Spine-Care Journal (EBSJ) section of Global Spine Journal (GSJ) welcomes this contribution by Hutton et al regarding impact sports and severe cervical spine injuries as a timely contribution. Following a number of suggestions, our reviewers enthusiastically endorsed publication of this study as an unprecedented comprehensive comparison study of catastrophic cervical spine injuries in major contact team sports. EBSJ/GSJ shares the surprise of the authors that relatively scant attention has been placed in the peer-reviewed spine literature on cervical spine injuries despite sports being one of the leading injury mechanisms for cord injuries. 1 In this preceding article, an international body of recognized sports/spine surgeon experts led by M. Hutton from the United Kingdom performed a thorough review of the available world literature following a formal systematic review approach and condensed findings about catastrophic spine injuries into a common numeric denominator—either a population of 100,000/y or individual player exposure per 100,000 player-hours. This approach also allowed for some unprecedented cross-sports comparisons and further allowed interesting extrapolations regarding the influence of equipment and rules changes on major cervical injury prevention.
Although at first glance the absolute numbers of catastrophic cervical spine injuries seems to be reassuringly low, the individual adverse impact on players and their families cannot be overstated, as shown in the graphic case examples. The low-appearing incidence of serious spine injuries in the past has likely led to an underestimation of this injury entity and certainly has prevented a more structured approach to injury prevention and acute management in the athletic domain. Because organized sports tend to get more competitive and players tend to get bigger and faster, our understanding of trend changes and intervention strategies created early on need to keep in step with this increasing professionalization of sports at all levels, regardless of gender and age of players. An emerging additional concern arising from this study is the lack of recorded injury statistics relative to practices and moreover formally recorded spine injury rates for organized youth and recreational contact sports leagues. In the big picture, it appears that rugby at all levels and its various codes have recently arrived at a far more comprehensive and transparent system of data collection for all age groups, something that North American organized football and other sports disciplines hopefully will take on as a necessary future foundational aspect of conducting business. Other sports like soccer, ice hockey, and Australian rules football may also be underreporting their actual injury rates in absence of effective sportswide registries. One can only hope that commercial interests do not override the safety and well-being of players, especially when injury prevention measures can be effectively instituted with rule changes.
A final crucial question arises out of the analogy to the head injury model: if repetitive traumatic brain injuries can be exacerbated by cumulative effects, could the same hold true for the cervical spine? What are the rates of symptomatic cervical spondylosis (i.e., myelopathy, radiculopathy, syrinx formation, demyelination) and is the cervical spinal cord itself susceptible to recurrent concussive trauma in certain at-risk patients? An epidemiologic study of former professional players and their risk exposure to neck surgery, myelopathy, and even diseases like amyotrophic lateral sclerosis might be a worthwhile next step for investigation on the potential ill effects of high impact contact sports on player health.
In the meanwhile, GSJ and AOSpine congratulate the authors on their data collection from around the world and for their work and hope that the response to their inaugural efforts will lead them to further investigative work in the underexplored realm of sports and spine disorders.
Footnotes
Acknowledgments
Analytic support for this work was provided by Spectrum Research, Inc. with funding from AOSpine.