
Abstract
Study Design
Literature review.
Objective
Several studies have shown that the accuracy of pedicle screw placement significantly improves with use of computed tomography (CT)-based navigation systems. Yet, there has been no systematic review directly comparing accuracy of pedicle screw placement between different CT-based navigation systems. The objective of this study is to review the results presented in the literature and compare CT-based navigation systems relative only to screw placement accuracy.
Methods
Data sources included CENTRAL, Medline, PubMed, and Embase databases. Studies included were randomized clinical trials, case series, and case–control trials reporting the accuracy of pedicle screws placement using CT-based navigation. Two independent reviewers extracted the data from the selected studies that met our inclusion criteria. Publications were grouped based on the CT-based navigation system used for pedicle screw placement.
Results
Of the 997 articles we screened, only 26 met all of our inclusion criteria and were included in the final analysis, which showed a significant statistical difference (p < 0.0001, 95% confidence interval 0.92 to 1.23) in accuracy of pedicle screw placement between three different CT-based navigation systems. The mean (weighted) accuracy of pedicle screws placement based on the CT-based navigation system was found to be 97.20 ± 2.1% in StealthStation (Medtronic, United States) and 96.1 ± 3.9% in VectorVision (BrainLab, Germany).
Conclusion
This review summarizes results presented in the literature and compares screw placement accuracy using different CT-based navigation systems. Although certain factors such as the extent of the procedure and the experience and skills of the surgeon were not accounted for, the differences in accuracy demonstrated should be considered by spine surgeons and should be validated for effects on patients’ outcome.
Introduction
Pedicle screw insertion for spine fusion surgery is very common, and accurate screw placement is of utmost importance. Two of the most widely used techniques for pedicle screw placement include conventional or freehand technique as well as computer-assisted surgery (CAS). Conventional methods rely mainly on anatomical landmarks with or without the assistance of radiologic imaging modalities to localize the pedicle. 1 Despite the use of different versions of these techniques, several studies have reported high rates of screw misplacement and cortical perforation.2,3 Screw misplacement can threaten the surrounding neurovascular structures and can also affect the mechanical stability of the entire construct, hence increasing the rate of revision surgery and cost. 4 New methods to improve pedicle screw placement accuracy have led to the development of CAS. Multiple studies have shown that the accuracy of pedicle screw placement significantly improves with the use of CAS as compared with conventional methods.5,6 Several types of CAS systems have been developed including computed tomography (CT)-based navigation and fluoroscopic navigation. 7 The CT-based navigation systems utilize a preoperatively obtained CT data set as the source data and register the patient intraoperatively with a frameless stereotactic system to this data set. On the other hand, the fluoroscopic navigation systems use intraoperative two- or three-dimensional fluoroscopic images for the source data and register the patient with a frameless stereotactic system to these images. 8
The CT-based CAS systems allow precise placement of instruments by providing real-time feedback and anatomical details of the unexposed or partially exposed pedicles, eliminating the exposure to fluoroscopic radiation. 9 However, new concerns about CT-navigated surgery have appeared, including movement of the registration markers, the limited field in multilevel procedures, the excessive preoperative preparation, as well as a steep learning curve. 10 Although several clinical studies have demonstrated high accuracy rates of pedicle screw placement using CT-based navigation, none analyzed the accuracy among different CT-based navigation systems.
The present study is aimed at reviewing the literature on CT-based navigation and comparing the accuracy of different CT-based navigation systems. We hypothesize that the accuracy of pedicle screw placement would be similar between CT-based navigation systems in the literature.
Materials and Methods
Publication Selection
An equivalent search strategy was performed to identify relevant articles in the Cochrane Central Register of Controlled Trials (CENTRAL), Medline, PubMed, and Excerpta Medica Database (Embase). The following keywords and their respective combinations were used in this search: “computed tomography based,” “spine,” and “navigation.” The search was limited to English-language articles.
Two reviewers (A.N. and J.L.) independently screened the titles and abstracts of all retrieved articles for eligibility. In the case of disagreement, the reviewers discussed the inclusion criteria until a common consensus was reached. The two reviewers obtained and reviewed the articles using equivalent data extraction methods.
Study Selection
Only studies meeting the inclusion criteria were considered for analysis. The inclusion criteria used were: (1) all studies (randomized clinical trials, case series, case–control studies) with the exception of case reports; (2) studies using CT-based navigation or cervical, thoracic, or lumbar pedicle screw insertion; (3) studies identify the name of the CT-based navigation system; (4) studies with a clear surgical intervention technique; (5) studies using 2-mm increments to assess the accuracy of pedicle screw placement; (6) human studies; (7) CT-based navigation systems with accuracy reported in three or more articles in the literature; (8) studies published in 2004 and after. Articles depicting in vitro studies, cadaveric studies, or biomechanical studies were excluded.
Data Extraction
Two independent reviewers extracted the data from the selected studies. The final data extracted included number of patients, manufacturer, number of pedicle screws placed in each study, accuracy of the placed pedicle screws, and vertebral levels instrumented.
Statistical Analysis
The publications were grouped based on the CT-based navigation system used for pedicle screw placement. The accuracy of the pedicle screw placement was readjusted based on the 2-mm increments according to the work published by Aoude et al. 11 Screws perforated less than 2 mm were considered optimally placed, and screws perforated more than 2 mm were considered inaccurate. All means were weighted on the number of the screws used to provide a better competitive estimate. The descriptive statistics for screw placement accuracy according to the classification methods included the overall number of screws, the total number of screws for each manufacturer, weighted mean accuracy of pedicle screw placement for each manufacturer, and the standard deviation. The independent-samples t test was performed to assess whether there was a difference in screw placement accuracy between different CT-based navigation systems. A p value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS V.21 (IBM Corporation, Armonk, New York, United States).
Results
The initial electronic search identified a total of 997 articles. Only 92 were relevant to our topic (
Studies that used CT-based navigation for pedicle screws placement
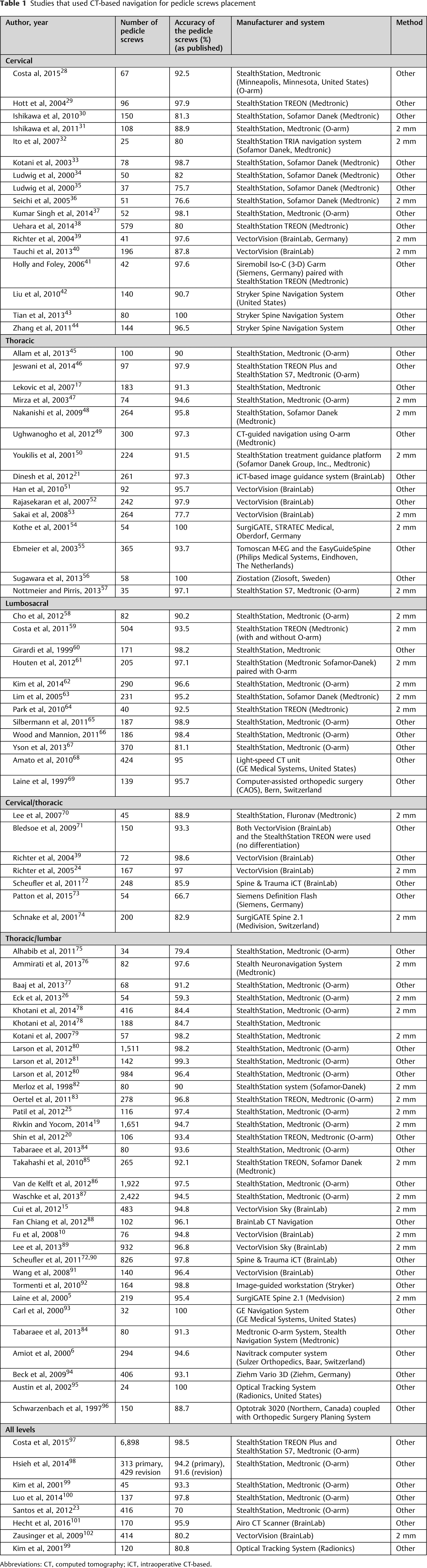
Abbreviations: CT, computed tomography; iCT, intraoperative CT-based.
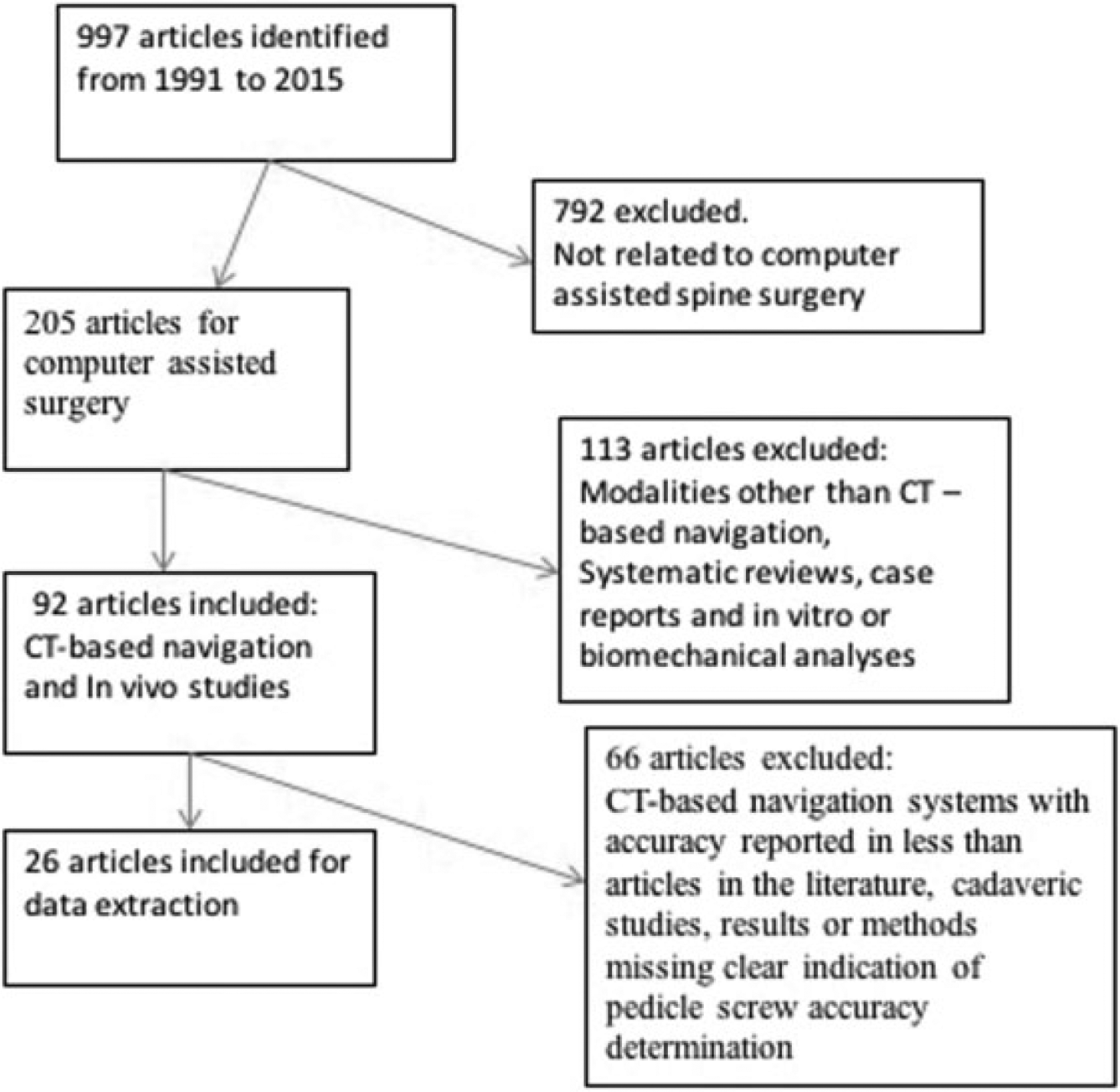
Graphical depiction of the systematic article selection process used. Abbreviation: CT, computed tomography.
Studies using the 2-mm increment grading system based on CT imaging
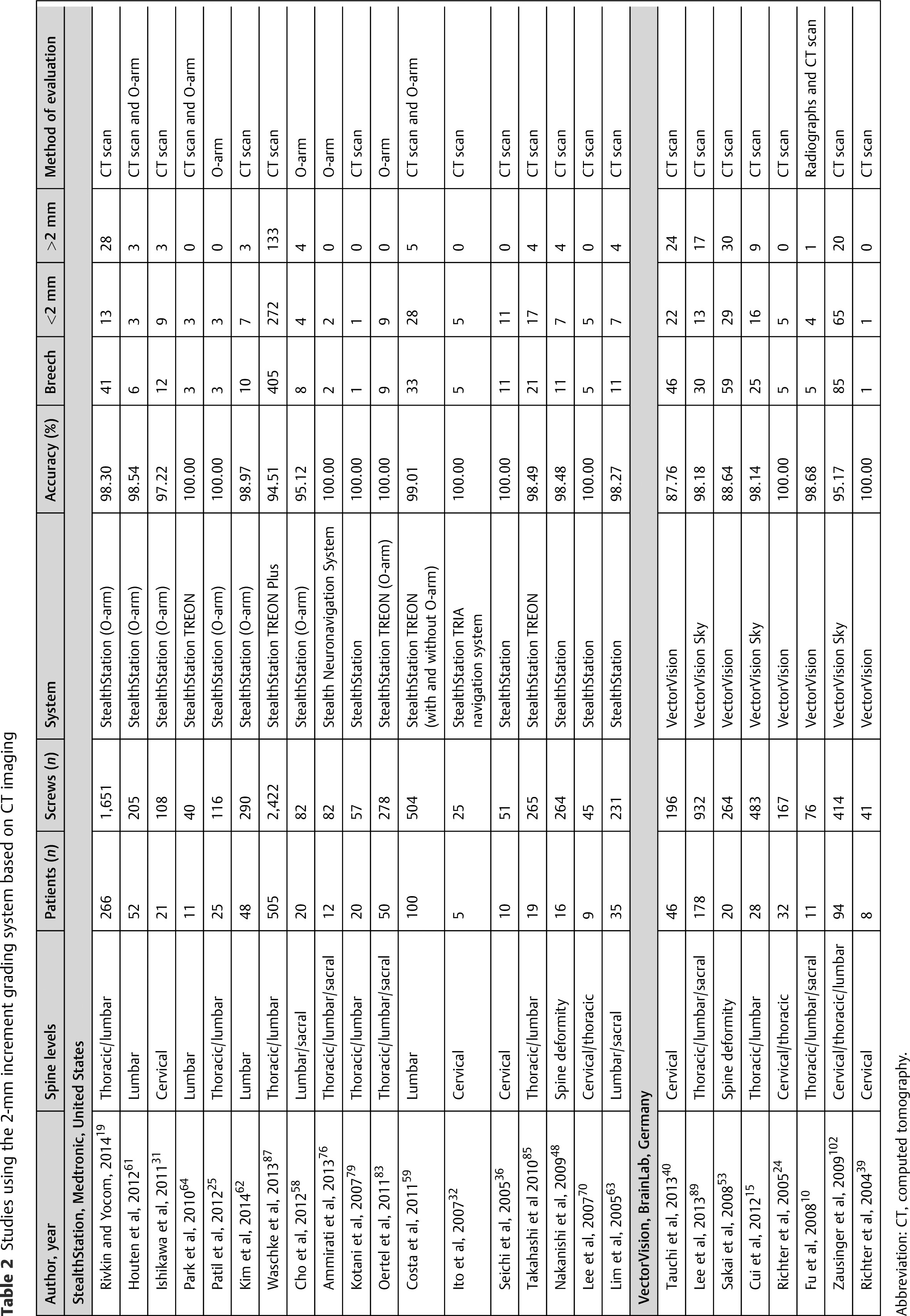
Abbreviation: CT, computed tomography.
Imaging modalities were used to assess pedicle screw accuracy in all 26 articles. The majority of the studies used postoperative CT scan to assess pedicle screw placement accuracy (69.2%). The remainder of studies used O-arm with or without CT scan to assess pedicle screw placement accuracy.
Our analysis showed that 18 of 26 publications used the StealthStation navigation system (Medtronic, Minneapolis, Minnesota, United States) and 8 used the VectorVision navigation system (BrainLab, Germany). For all publications, the screws were classified as “safe/optimal” if they breeched pedicles by 2 mm or less and “unsafe” if they breeched more than 2 mm. In all, 6,716 screws were placed using the StealthStation navigation system and 2,573 screws were placed using the VectorVision navigation system. Of these subgroups, 414 screws were placed in the cervical and thoracolumbar area, 212 in the cervicothoracic area, 6,675 in the thoracolumbosacral area, 421 solely cervical, 1,039 pedicle screws solely lumbar, and 528 for spine deformity.
Our review revealed that of the 9,289 pedicle screws, a total of 853 (9.2%) had reported pedicle breeches. Of these, 561 (65.8%) breeches were less than 2 mm and 292 (34.2%) were more than 2 mm.
Finally, the mean (weighted) overall accuracy of all pedicle screw placements was 96.90 ± 2.7%. The mean (weighted) accuracy of pedicle screw placement based on the CT-based navigation system was 97.20 ± 2.1% in the StealthStation and 96.1 ± 3.9% in the VectorVision. With regard to the 2-mm increment grading system, the results showed a significant statistical difference between different navigation systems (p < 0.0001, 95% confidence interval = 0.92 to 1.23). The descriptive statistics for screw placement accuracy of the two navigation systems using the 2-mm increment are presented in
Descriptive statistics for pedicle screw accuracy comparing different CT-based navigation systems
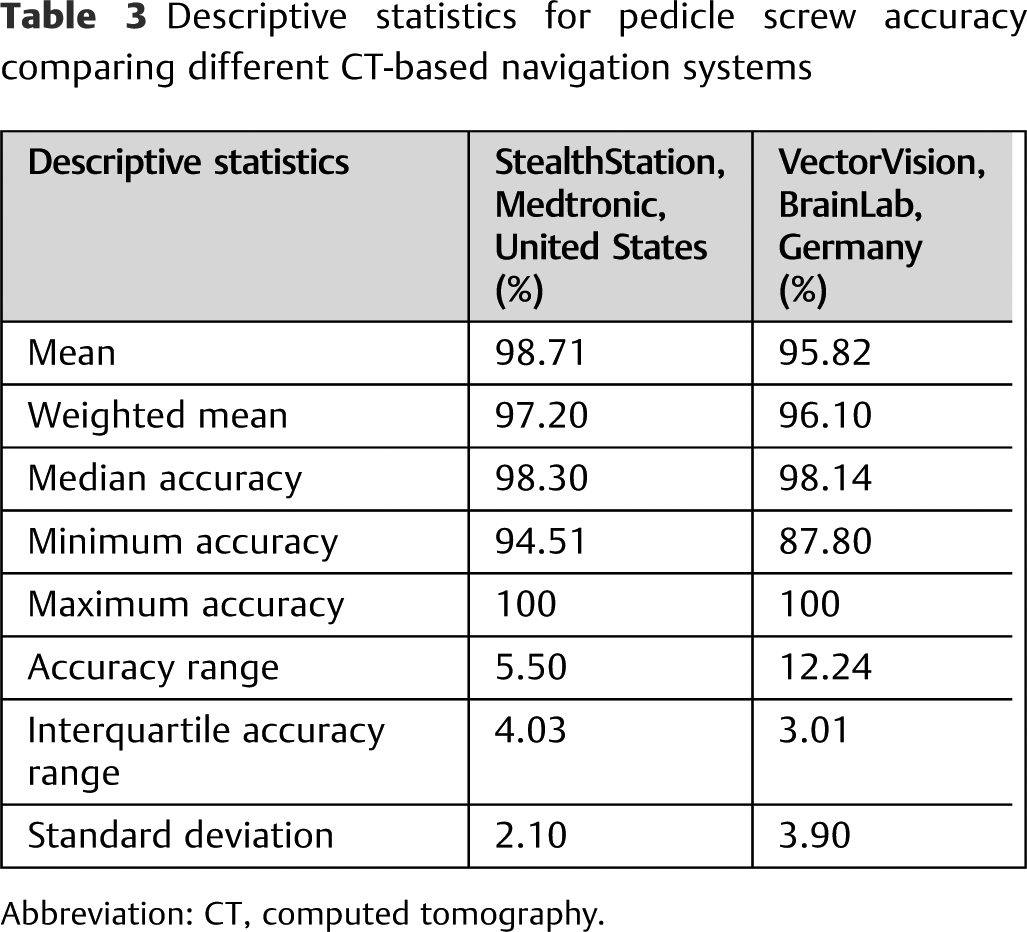
Abbreviation: CT, computed tomography.
Discussion
Comparing computer navigation systems in orthopedics is not uncommon; yet, most are not related to spine surgeries.12,13 Honl et al compared acetabular cup orientation between five different computer-assisted navigation systems for total hip arthroplasty and demonstrated significant differences among them. 12 In addition, Carli et al compared the accuracy of intraoperative measurements to postoperative tibial and femoral alignment in two different computer-assisted systems for total knee arthroplasty and found a significant difference in the outcome as well. 13 Interestingly, several clinical studies have demonstrated high accuracy rates of pedicle screw placement using CT-based navigation compared with other methods, such as freehand technique and fluoroscopic navigation.14,15 However, a critical aspect of the operative procedure was not taken into account, which is the type of computer navigation system being used. The review by Gelalis et al included a total of seven different CT-based navigation systems by different manufacturers that have been used for pedicle screw placement. 14 Nevertheless, the study did not report any comparison in the accuracy of each of the systems. To our knowledge, our study is the first study to compare the accuracy of pedicle screw placement between different computer navigation systems. Our results showed that there is a difference in the accuracy of pedicle screw placement among different CT-based navigation systems. It should be stressed that although the accuracy is significantly different between the CT-based navigation systems, the difference is minimal. Despite that, such a small difference might affect patients’ outcome, especially in spine surgery, where the driving purpose of CT-based navigation is to decrease the incidence of unwanted complications.
The overall weighted mean accuracy in our review was 96.90 ± 2.7% in 9,289 pedicle screws placed in the different regions of the spine. These results are consistent with previous reported results that used different criteria for accuracy assessment.5,14 Gelalis et al did a systematic review comparing the freehand technique, fluoroscopy-guided, fluoroscopy-based navigation, and CT-based navigation. 14 Their overall accuracy of pedicle screw placement using CT-based navigation ranged from 89 to 100%, according to 2-mm increments. On the other hand, Li et al concluded that there is no significant difference between the conventional techniques and CT-based navigation. 16 Interestingly, Lekovic et al concluded that different imaging guidance modalities were not associated with an increased rate of pedicle breakout or the severity of the breakout. 17
Numerous factors have been identified to play an important role in the accuracy of pedicle screw placement without taking into account the type of CT-based navigation system. Of these factors, this technique was reported to be associated with a learning curve, which exists for almost every new surgical technique. Wood and McMillen examined the relationship between the learning curve and the accuracy of pedicle screw placement. The study concluded that the accuracy of pedicle screw placement improves as the surgeon becomes more familiar with the technique. 18 A more recent study by Rivkin and Yocom, who used the StealthStation navigation system in their study, reported a steeper learning curve. They suggested that ∼15 to 30 cases are required to consistently attain breach rates that are similar to what is reported in the literature. 19
Surgical techniques and the dimension of the surgical object is another important factor. Lekovic et al reported that the incidence of unintended screw perforations mainly depends on the pedicle diameter. 17 Several other factors can have a confounding effect on pedicle screw accuracy as well. The extent of the surgery can have an effect on the accuracy. For example, Shin et al explained that using the O-arm in conjunction with the StealthStation navigation system, although reported to provide the largest field of view among intraoperative image-guided applications, is still insufficient to properly perform multilevel surgery. A single scan can only yield images for a maximum of four spinal segments. Therefore, multiple scans are required in multilevel surgeries, which can create longer operative times and can lead to a compromise in screw accuracy. 20
Furthermore, as previously stated, some vertebra segments are more difficult to operate on than others. Thoracic spine surgery has been shown in the literature to be a difficult and demanding surgery.20,21 The anatomical differences between the thoracic and lumbar vertebra lead to different maximal acceptable translational and rotational errors. 22 Another confounding factor in attaining an accurate assessment of the rates of pedicle screw misplacement is the wide variability of assessment tools. Some surgeons undertake routine radiographs postoperatively and others undertake CT scanning and O-arm, which is by far more sensitive to minor screw breeches. 23 Other factors that can be attributed to this difference include the involvement of different patient demographics, different surgical techniques, and the range in the complexity of the surgery. In our review, 69.2% of the articles used postoperative CT scan. However, the rest of the articles used radiographs and the O-arm. Aoude et al concluded that 2-mm increments are the most widely accepted for determining pedicle screw placement accuracy. 11 Using the 2-mm increments, it is possible to compare CT-based navigation systems with one another by assessing the accuracy of pedicle screw placement in each system. This comparison is important, because the more accurate the CT-based navigation is, the more confident the surgeon can be.
Although it is accepted today that intraoperative CT-based navigation systems are more accurate than conventional methods, the significant variations in accuracy of CT-based navigation systems reported in the literature remain ambiguous. Numerous studies even stated that no pedicle breaches occurred. Using the 2-mm increment method, 11 both Richter et al 24 and Patil et al, 25 among several other studies that met our inclusion criteria, reported 100% accuracies. Richter et al used the VectorVision navigation system and evaluated 167 screws. 24 Patil et al used the StealthStation navigation system and evaluated 116 screws. 25 Some studies had much lower accuracy rates, like a study by Eck et al, 26 which reported an accuracy of 59.3% while using the StealthStation navigation system. The present study’s statistical analysis shows that the differences in the weighted mean accuracy rates between different CT-based navigation system manufacturers are significant. The mean accuracy of pedicle screw placement based on the CT-based navigation system was found to be 97.20 ± 2.1% for StealthStation and 96.1 ± 3.9% for VectorVision. Surgeons must keep in mind that despite many other factors, the accuracy of their pedicle screw insertion can be affected by which navigation system is employed. Future studies should consider the technology behind these navigation systems and try to determine how they differ and what permits one manufacturer to be more accurate than the other. Doing so can present the opportunity of providing the best technology in spinal navigation, 27 therefore decreasing the need for revision surgeries and potentially reducing complication rates and negative outcomes. 22
Given all these factors that may influence the accuracy of pedicle screw placement when using intraoperative CT-based navigation systems, the present study shows that accuracy is significantly affected, depending on the company of the navigation system used in surgery. Therefore, despite the steep learning curve and the extent of the procedure, this study is the first in the literature that shows that no matter how experienced a surgeon is, their outcomes can be affected by the navigation system.
The cervical spine has a complex anatomy and a relatively greater mobility when compared with the lumbar or thoracic spine, which may have affected the accuracy of screw placement. The statistical analysis was repeated after excluding the publications that reported screw placement in the cervical vertebrae. The statistical difference remained significant. Additionally, we repeated the analysis after excluding modalities that create CT-like images (image quality lower than the standard CT scan), such as the O-arm, which may have affected the accuracy as well. The results again remained statistically different.
There are several limitations in this study. A certain degree of heterogeneity exists among the studies included in the literature review. Certain patient factors remained unaccounted for when considering statistical difference between navigation systems, such as patients’ age, body mass index, sex, and demographic characteristics. The extent of the procedure, the experience and skills of the surgeon, the indication of surgery, and the length and diameter of the screws also remained unaccounted for. Medtronic’s navigation system models were notably the most prevalent in the literature. This fact is reflected in
Doing a study comparing different technologies can be a difficult task, as technological advancements are constantly being made, especially in the rapidly evolving field of surgery. Another limitation that must be considered is that the software and hardware of these CT-based navigation systems have undergone updates throughout the selected period of this study. This discrepancy of software and hardware is another source of heterogeneity among the studies that met our inclusion criteria. However, the changes in these systems within the period of these studies appear to be subtle enough in their function and performance, such that the accuracy rates were not significantly affected.
Furthermore, it must be noted that to show the actual accuracy of a navigation system, the planned trajectory of a screw should be compared with the final screw position. Nevertheless, the only available information about the accuracy of different CT-navigation systems is the final screw position, which may be misleading in certain situations, because surgeons can achieve optimal screw position by changing the planned trajectory that was proposed by the navigation system.
Also, future studies should look into other perioperative factors, such as blood loss, radiation exposure, operation time, and registration time, and a cost–benefit analysis should be done to justify the use of navigation systems.
We present a systematic literature review of CT-based CAS for pedicle screw placement. This review summarizes the results presented in the literature and compares the CT-based navigation systems to one another, relative to screw placement accuracy. We believe this study to be the first to compare the accuracy of different CT-based navigation systems in spine surgery. Our study shows that a significant statistical difference exists between these navigation systems, which affects accuracy. The goal of this study is to show that differences between systems exist and should be considered when using CT-based navigation systems.
Footnotes
Disclosures
Anas Nooh: none
Joushua Lubov: none
Ahmed Aoude: none
Sultan Aldebeyan: none
Peter Jarzem: none
Jean Ouellet: none
Michael H. Weber: none