
Abstract
Study Design
Retrospective review of prospectively gathered data.
Objective
To report the rate and impact of perioperative complications in cervical spine surgery. To our knowledge, no prior study of the cervical spine has analyzed a large prospectively gathered data set for adverse events, based on surgical subgroup.
Methods
The ProSTOS database features prospectively documented perioperative adverse events for 1,269 patients who had cervical spine surgery at multiple centers in North America between 2008 and 2011. We subgrouped patients by approach, whether surgery was a primary or revision operation, and by the number of levels involved. Multivariate analysis with stepwise logistic regression was used to relate complication rates to gender, age, smoking status, body mass index, approach, revision status, and number of levels involved. Follow-up was 41%.
Results
Adverse events occurred significantly more frequently in posterior and combined procedures than in anterior procedures. Revision surgery had significantly more complications than primary surgery. For patients who had anterior surgery, those who had one, two, and three or more levels operated had no significant difference in complication rates. Patients who had posterior surgery had significantly more complications if they had two or more levels operated compared with one level. The lowest rates of complications were for one-level primary surgery (<5%), and multilevel posterior, revision posterior, and revision combined surgery had complication rates over 6 times higher (>28%). Patients who had complications were significantly older than patients who did not. The most common adverse events were dysphagia and cardiac complications. The most severe morbid complications, in terms of increased treatment needs and hospital stay, were paraparesis and seizure.
Conclusions
Perioperative complication rates in cervical spine surgery are significantly lower in younger patients, surgery performed through an anterior approach (compared with a posterior or combined approach), with fewer levels involved (particularly in posterior surgery), and in primary (compared with revision) procedures.
Keywords
Introduction
The goal of this study is to report the rate and impact of perioperative complications in cervical spine surgery. We focus our analysis on which types of complications are associated with certain subgroups of procedures. We reviewed the Prospective Spine Treatment Outcomes Study (ProSTOS) database, which has not been previously utilized for this purpose. To our knowledge, no prior study of the cervical spine has analyzed a large, prospectively gathered data set for adverse events based on surgical subgroups. We present a risk profile of 26 types of perioperative adverse events, stratified by type of surgery (anterior versus posterior versus combined approach, primary versus revision surgery, and number of motion segments involved). This data can inform decision making as clinicians counsel patients about surgical options for cervical spine pathology.
Materials and Methods
The ProSTOS database features prospectively documented perioperative adverse events for 1,269 patients who had cervical spine surgery at multiple centers in North America. The database was compiled by the Association for Collaborative Spine Research (ACSR). Each institution had its own Institutional Review Board (IRB), and this study was granted IRB-exempt status by the lead author's home institution to mine the database (which contained no patient-identifying information). All surgeries in this study were performed between 2008 and 2011. Although seven or eight centers contributed data (depending on the year), the majority of patients came from three centers. To avoid selection bias, a study coordinator at each center enrolled all surgical patients into a database that consisted of fields for patient demographic information, procedural data, and surgeon-reported complications. Data was documented on a ProSTOS questionnaire form. Patients were followed up to 2 years postoperatively, and rates of follow-up were 41, 45, 34, and 18% at 3, 6, 12, and 24 months, respectively. We report only complications that occurred within 3 months of the index surgery (41% follow-up), which we designate the “perioperative period.” This window was selected to encompass the inpatient and postoperative patient encounters in the 90-day global period.
The ProSTOS cervical database includes 2,829 patients who had cervical spine surgery and who were followed prospectively. We included all patients from the database who had adequate documentation to determine what type of surgery they had, leaving 1,269 patients (44.8% of the database). Patients were grouped according to type of surgery (primary/revision, anterior/posterior/combined). Traditional decompression and fusion surgeries (anterior cervical diskectomy and fusion [ACDF], corpectomy, and laminectomy/fusion) were subgrouped according to how many levels (motion segments) were involved. For example, a C5 corpectomy was classified as two levels because it involved fusion across the C4–C5 and C5–C6 motion segments. Likewise, a C4–C5–C6 posterior fusion was classified as two levels because it spanned two motion segments (C4–C5 and C5–C6).
Clinicians reported complications on the Spine Adverse Events Severity System form, which includes check boxes to document the occurrence of several types of intraoperative and pre- or posttreatment medical and surgical adverse events (such as dural tear and pneumonia, among others). The severity of each adverse event was graded on a scale of 1 to 6. Grade 1 represents an adverse event that does not require treatment and has no adverse effect. Grade 2 is an adverse event that requires minor treatment but has no long-term effect. Grade 3 events require invasive or complex treatment (such as intensive care unit monitoring or surgery) and lead to an adverse outcome expected to last fewer than 6 months. Grade 4 events require complex treatment and lead to adverse outcomes expected to last more than 6 months. Grade 5 events include serious neurologic injuries (causing deterioration of one or more grades in American Spinal Injury Association [ASIA] score) and life- and limb-threatening (sentinel) events. Grade 6 adverse events result in death. The Spine Adverse Events Severity System has been previously validated and was found to have excellent interobserver reliability with broad capture of medical and surgical complications. 1 Clinicians then estimated the effect of the adverse event on increased length of hospital stay, which was documented categorically: none, 1 to 2 days, 3 to 7 days, 8 to 14 days, 15 to 28 days, or more than 28 days.
Multivariate analysis with stepwise logistic regression was used to relate complication rates to gender, age, body mass index, approach, revision status, and number of levels involved. A p value < 0.05 was considered statistically significant.
Results
Demographic Information
The average patient age was 59.9 (range 22.9 to 91.6), and 43.7% were men. In this series, there were no anesthesia-related complications, no allergic reactions, no massive blood loss (>5 L in 24 hours or >2 L in 3 hours), and no vascular injuries (carotid or vertebral artery). The lowest rates of complications were for one-level primary surgery (<5%), and multilevel posterior, revision posterior, and revision combined surgery had complication rates over 6 times higher (>28%; Fig. 1). Patients who had complications were significantly older than patients who did not (57 versus 54.4, p = 0.02). Gender and body mass index were not significantly associated with complications. At 3 months after surgery, follow-up was 41%. We accepted any adverse event dated within 90 days of surgery to capture all perioperative complications and all complications that may have occurred during the postoperative inpatient stay. We selected a 90-day window because long-term follow-up in the data set was poor, and we assumed that inpatient adverse events would be more likely to be reported.
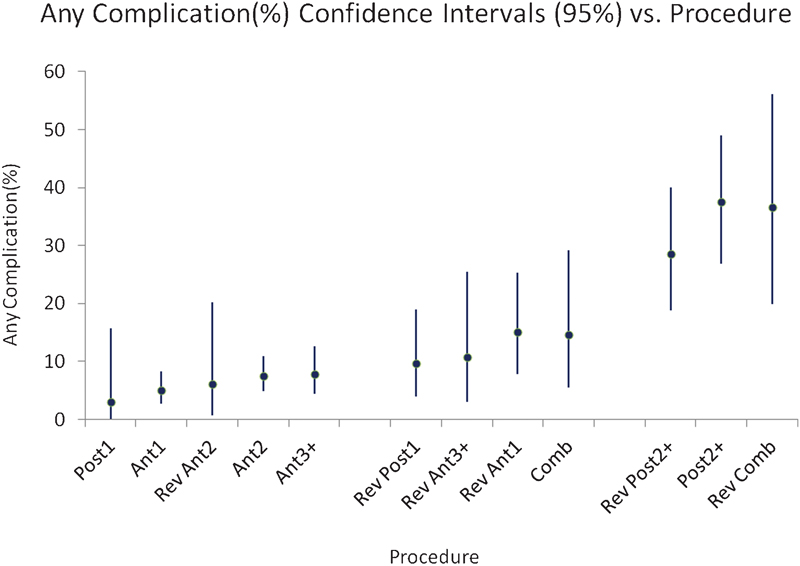
Rates of complications for each type of surgery. This figure graphically portrays data from Tables 1 2 3. Complication rates ascend from left to right. Error bars represent 95% confidence intervals. Abbreviations: Ant1, primary, anterior approach, one level; Ant2, primary, anterior approach, two levels; Ant3+, primary, anterior approach, three or more levels; Comb, primary, combined approach; Post1, primary, posterior approach, one level; Post2+, primary, posterior approach, two or more levels; Rev Ant1, revision, anterior approach, one level; Rev Ant2, revision, anterior approach, two levels; Rev Ant3+, revision, anterior approach, three or more levels; Rev Comb, revision, combined approach; Rev Post1, revision, posterior approach, one level; Rev Post2+, revision, posterior approach, two or more levels.
Effect of Number of Levels
Tables 1, 2, and 3 demonstrate the frequency of each type of complication for patients who had an anterior, posterior, or a combined (front–back) approach. The complication rate was significantly higher with two or more levels (compared with one level) in primary posterior surgery (p = 0.0002) and revision posterior surgery (p = 0.0037). For patients who had anterior surgery, those who had one, two, and three or more levels operated had no significant difference in complication rates. Patients who had posterior surgery had significantly more complications if they had two or more levels operated compared with one level (p = 0.0092). There was no difference in complication rates among the number of operated levels for patients who had a combined approach, although the sample size was small. Of patients who had one-level surgery, there was no approach effect, but of patients who had two- and three-level surgery, there was a significant approach effect (fewer anterior complications, p = 0.016 and p = 0.0002).
Anterior surgery
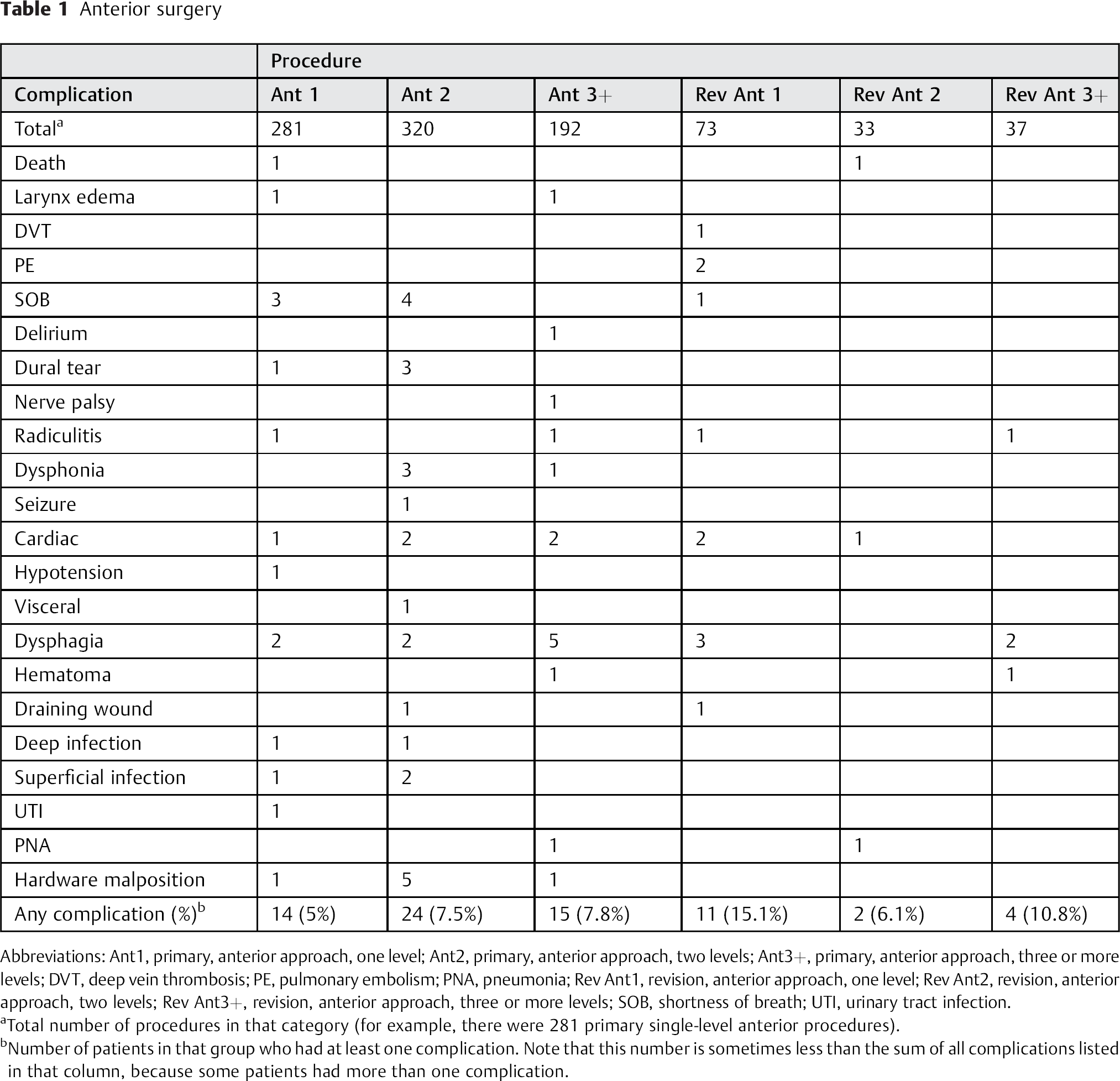
Abbreviations: Ant1, primary, anterior approach, one level; Ant2, primary, anterior approach, two levels; Ant3+, primary, anterior approach, three or more levels; DVT, deep vein thrombosis; PE, pulmonary embolism; PNA, pneumonia; Rev Ant1, revision, anterior approach, one level; Rev Ant2, revision, anterior approach, two levels; Rev Ant3+, revision, anterior approach, three or more levels; SOB, shortness of breath; UTI, urinary tract infection.
Total number of procedures in that category (for example, there were 281 primary single-level anterior procedures).
Number of patients in that group who had at least one complication. Note that this number is sometimes less than the sum of all complications listed in that column, because some patients had more than one complication.
Posterior surgery
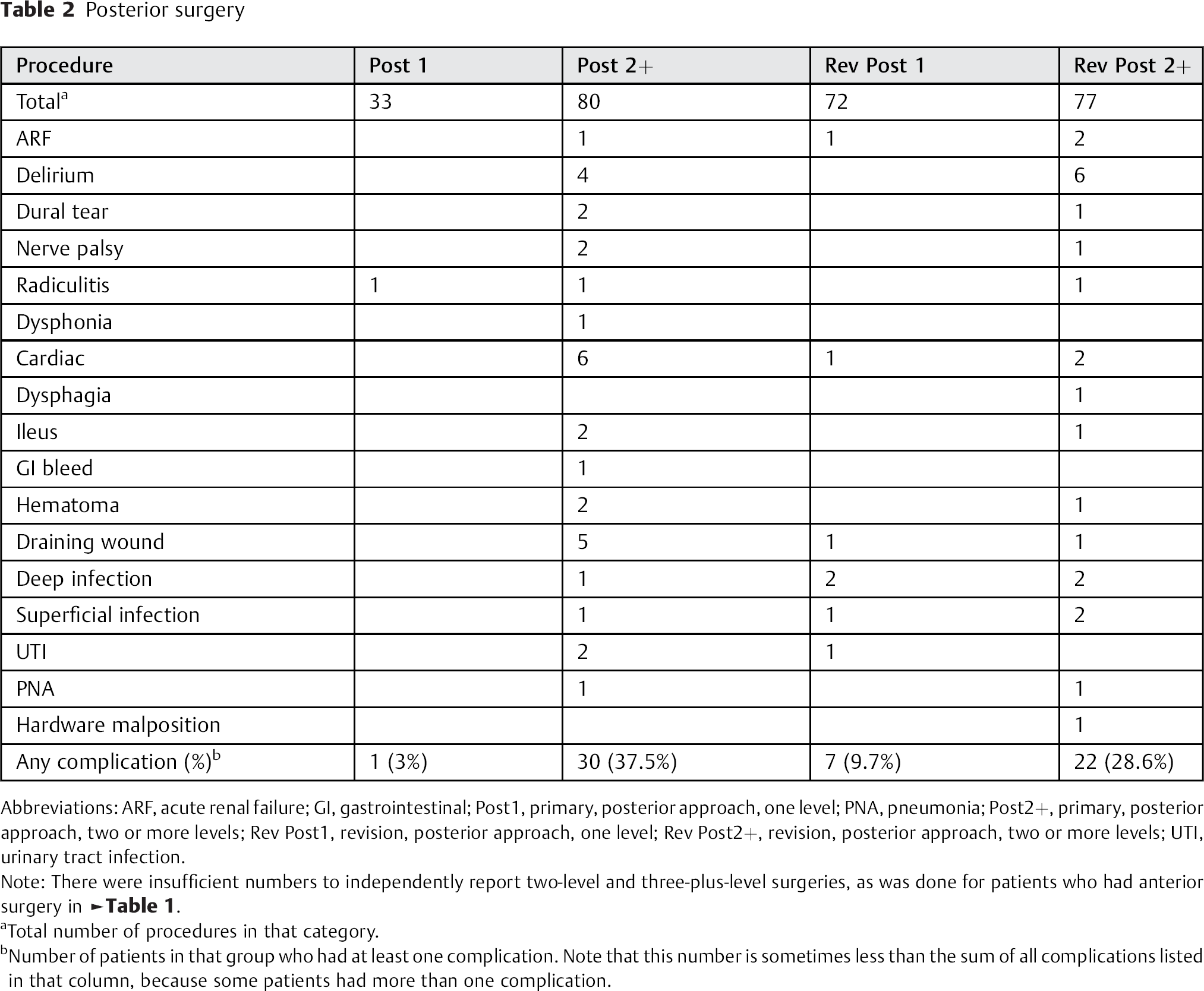
Abbreviations: ARF, acute renal failure; GI, gastrointestinal; Post1, primary, posterior approach, one level; PNA, pneumonia; Post2+, primary, posterior approach, two or more levels; Rev Post1, revision, posterior approach, one level; Rev Post2+, revision, posterior approach, two or more levels; UTI, urinary tract infection.
Note: There were insufficient numbers to independently report two-level and three-plus-level surgeries, as was done for patients who had anterior surgery in Table 1.
Total number of procedures in that category.
Number of patients in that group who had at least one complication. Note that this number is sometimes less than the sum of all complications listed in that column, because some patients had more than one complication.
Combined surgery
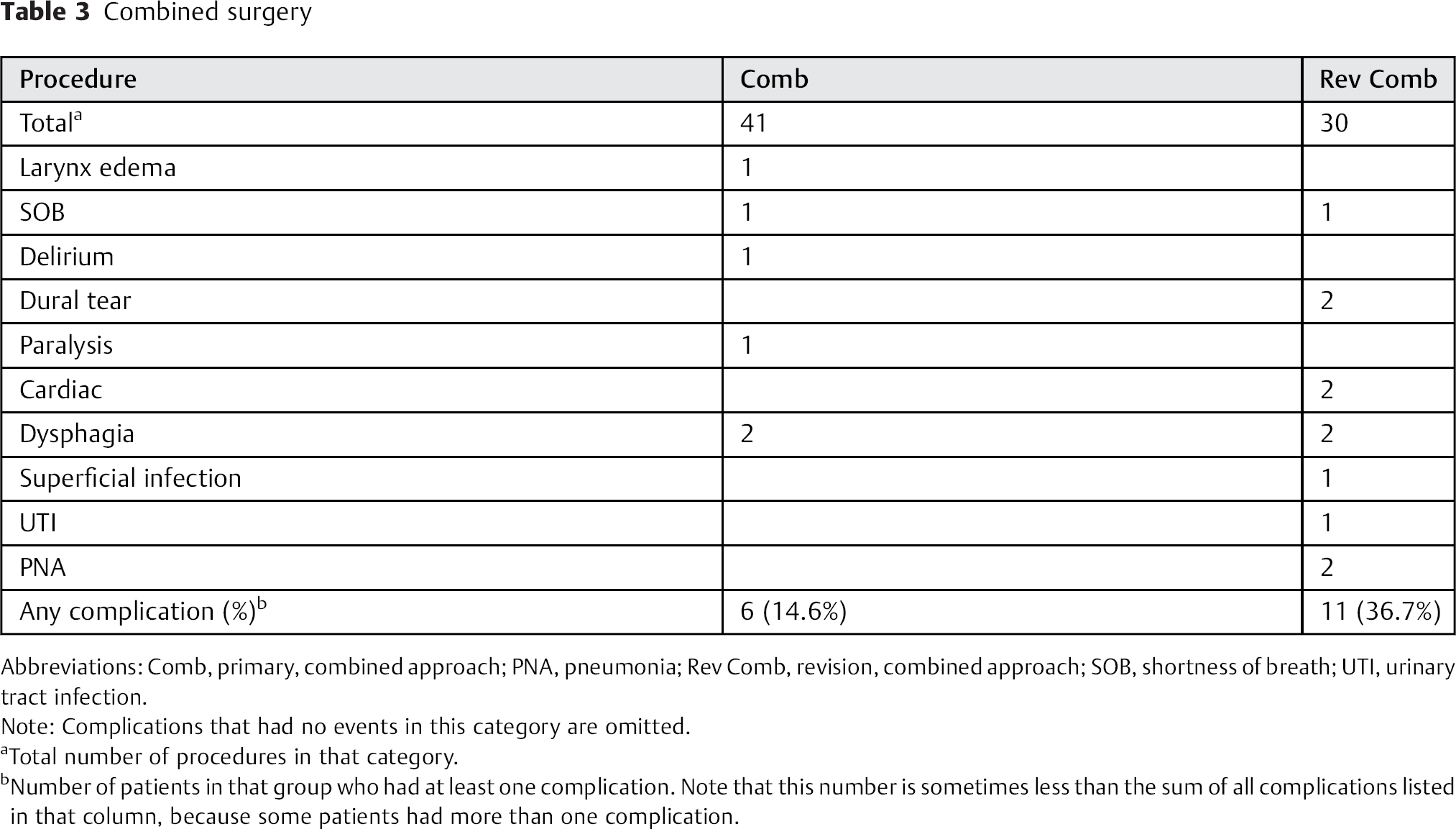
Abbreviations: Comb, primary, combined approach; PNA, pneumonia; Rev Comb, revision, combined approach; SOB, shortness of breath; UTI, urinary tract infection.
Note: Complications that had no events in this category are omitted.
Total number of procedures in that category.
Number of patients in that group who had at least one complication. Note that this number is sometimes less than the sum of all complications listed in that column, because some patients had more than one complication.
Effect of Revision Surgery
Of the 1,269 patients, there were 947 primary surgeries and 322 revisions. Overall, revision surgery had significantly more complications than primary surgery (14.3% versus 7.7%, p = 0.0003). Revision combined surgery had a significantly higher complication rate than primary combined surgery (p = 0.0316). Revision anterior one-level surgery had a significantly higher complication rate than primary one-level surgery (p = 0.0027). The complication rates for revision versus primary surgery in other comparable groups (anterior two levels, anterior three or more levels, posterior one level, posterior two or more levels) were not significantly different.
Effect of Approach
There were 936 anterior surgeries, 262 posterior surgeries, and 71 combined (front–back) surgeries. Table 4 summarizes the frequency of each type of complication for patients who had an anterior, posterior, or combined (front–back) surgical approach. Adverse events occurred almost 3 times more frequently in posterior and combined procedures than in anterior procedures, and this difference was significant (18.3, 16, and 6.5%, respectively; p < 0.0001).
Summary
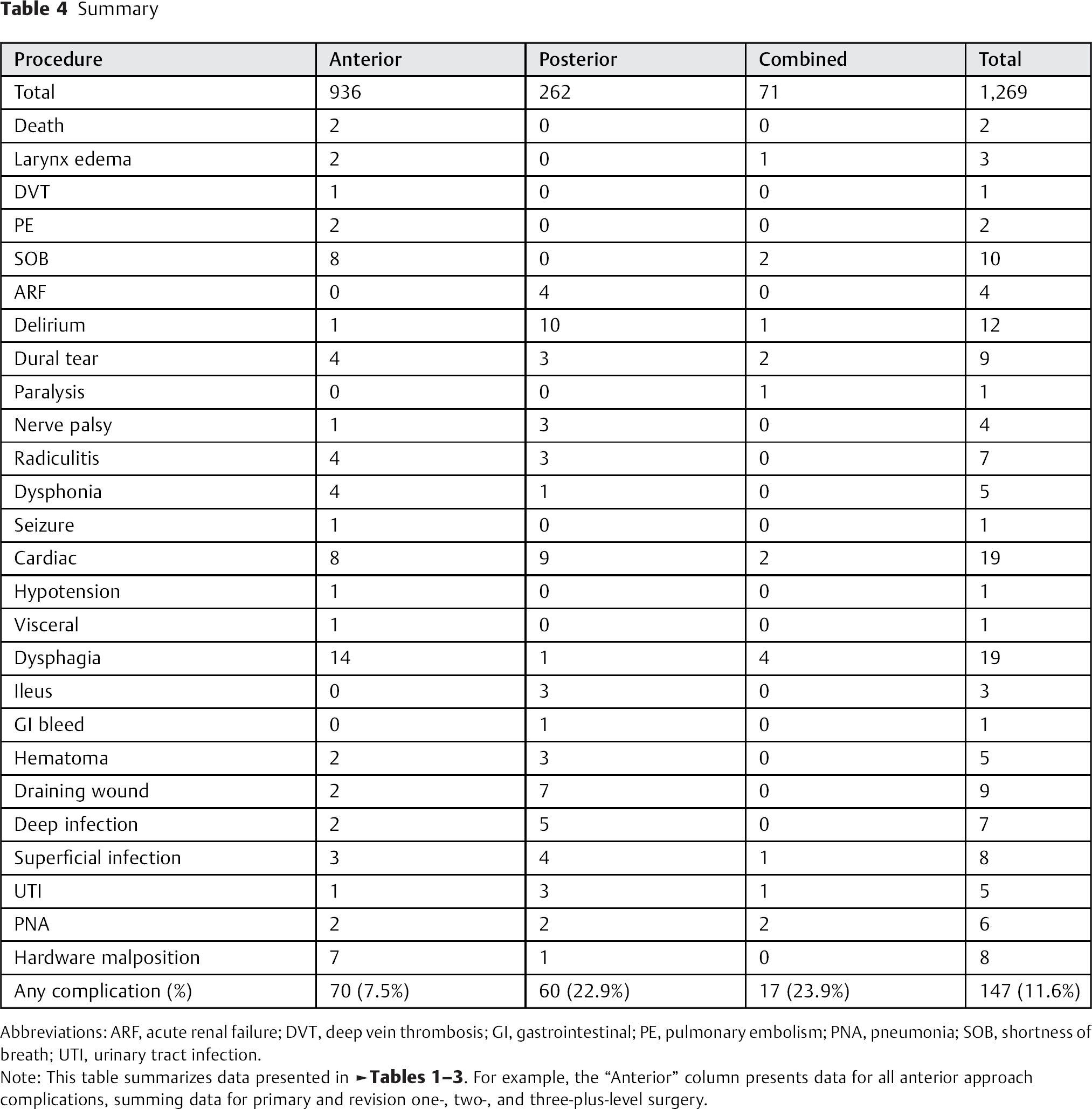
Abbreviations: ARF, acute renal failure; DVT, deep vein thrombosis; GI, gastrointestinal; PE, pulmonary embolism; PNA, pneumonia; SOB, shortness of breath; UTI, urinary tract infection.
Note: This table summarizes data presented in Tables 1 23. For example, the “Anterior” column presents data for all anterior approach complications, summing data for primary and revision one-, two-, and three-plus-level surgery.
Types of Complications
Death
There were two deaths in the data set (Table 1). Both were ultimately attributed to respiratory failure. One was a 57-year-old man who underwent anterior revision C4 corpectomy and had a postoperative cardiac arrest with subsequent aspiration pneumonia, sepsis, and respiratory demise. The other was a 64-year-old woman who underwent primary C3–C4 anterior cervical diskectomy and fusion and died from an intraoperative airway problem.
Respiratory
All respiratory complications (death, deep vein thrombosis/pulmonary embolism, laryngeal edema, and shortness of breath) occurred in patients who had either anterior-only (Table 1) or combined anterior–posterior (Table 3) procedures.
Neurologic
Dural tears were distributed across anterior, posterior, and combined approaches (Table 4). One patient was paralyzed after a primary combined procedure such that he lost at least 1 ASIA grade after surgery (Table 3). There were four C5 nerve palsies, two from primary posterior multilevel surgery, one from revision posterior multilevel surgery (Table 2), and one from primary anterior multilevel surgery (Table 1). Four cases of dysphonia occurred after anterior surgery, presumably due to recurrent laryngeal nerve injury, although a fifth case occurred after posterior surgery, perhaps due to endotracheal intubation. Delirium happened most commonly after posterior surgery (10 posterior versus 2 anterior cases).
Cardiac
Cardiac complications occurred at a rate of 1.5%, making it (along with dysphagia) the most common adverse event. Cardiac complications included myocardial infarction, heart failure, and arrhythmia. As shown in Table 4, these were among the most frequently reported adverse events in the entire series. The rates were relatively higher for posterior surgery (3.4%) and combined surgery (2.8%) than for anterior surgery (0.85%).
Dysphagia
Dysphagia occurred 18 out of 19 times from anterior or combined anterior–posterior surgery. The rate of dysphagia when an anterior approach was involved (including both anterior and combined cases) was 1.8%, compared with 0.38% of patients who had a posterior-only approach.
Wound Problems
As shown in Table 4, there were more frequent wound-related problems (hematoma, draining wound, superficial infection, or deep infection) in the posterior surgery group (7.25%) than in the anterior group (0.96%; odds ratio 5.4, p = 0.06). These wound-related problems appeared in 0.88% of primary anterior procedures compared with 2.10% of revision anterior procedures. Wound-healing problems were reported for 7.96% of primary posterior procedures versus 6.71% of revision posterior procedures, and for no primary combined procedures but for 3.33% of revision combined procedures. All anterior and posterior hematomas requiring debridement occurred after surgeries involving three or more levels (Tables 1 and 2).
Implants
Seven of eight cases of implant malposition resulted from anterior surgery (Table 4). Of these, the majority occurred in primary two-level surgery.
Adverse Event Severity
Table 5 depicts the average Spine Adverse Events Severity System grade (with 95% confidence intervals) for each type of complication. Aside from two deaths, the most morbid complication was one case of motor weakness (conversion of ASIA E to D). The next most morbid adverse events, based on this grading system, were one case of new-onset seizure, one case of gastrointestinal bleeding, and multiple cases of wound problems (draining wound, deep infection, and hematoma) requiring reoperation presumably for irrigation and debridement. The majority of adverse events were graded less than 2.5, indicating that most complications require minor treatment with no long-term consequences. Most complications resulted in either 1 to 2 days or 3 to 7 days of increased hospital stay, although the cases of seizure, paraparesis, and hematoma resulted in longer hospital stays.
Patient morbidity
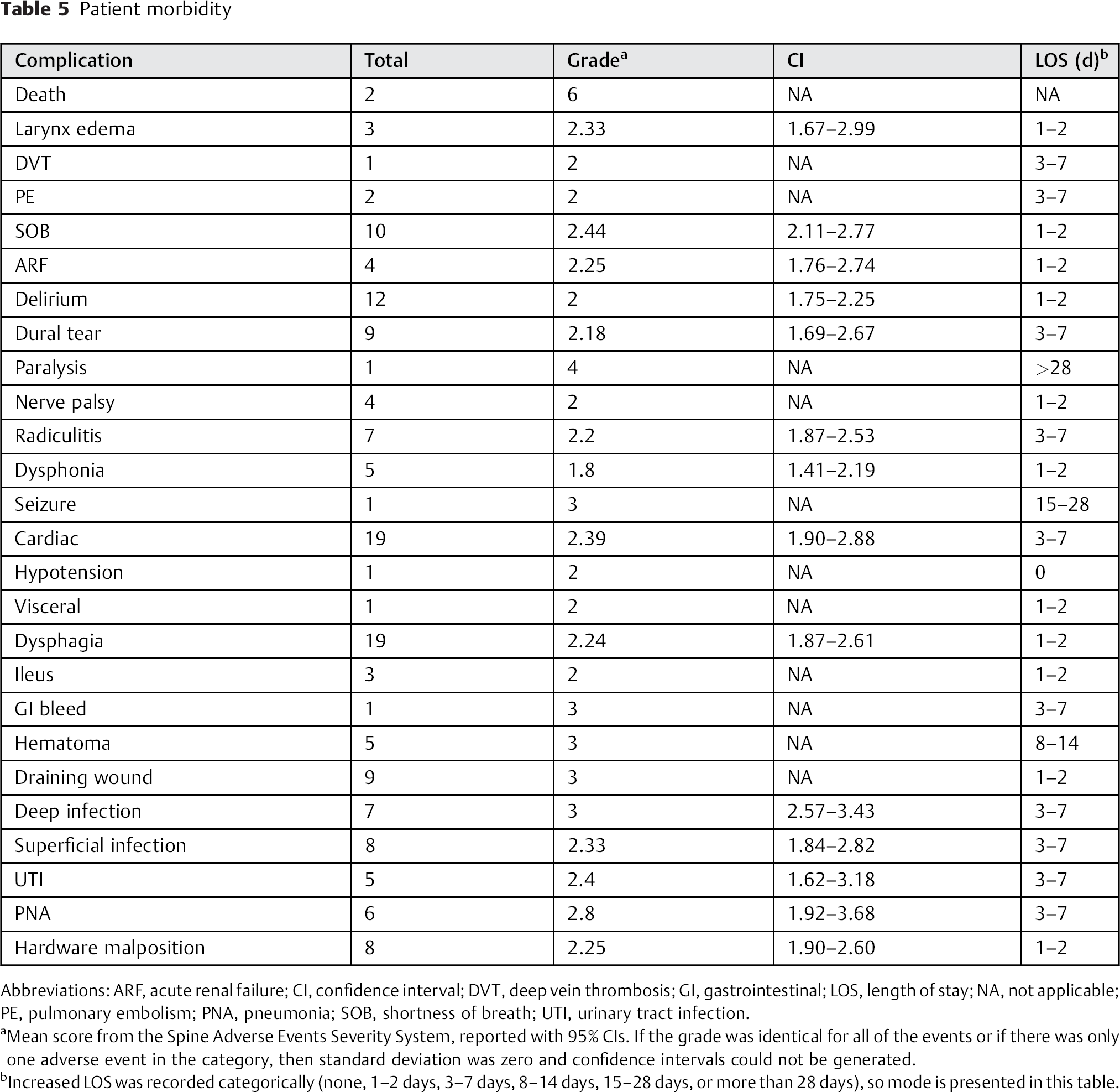
Abbreviations: ARF, acute renal failure; CI, confidence interval; DVT, deep vein thrombosis; GI, gastrointestinal; LOS, length of stay; NA, not applicable; PE, pulmonary embolism; PNA, pneumonia; SOB, shortness of breath; UTI, urinary tract infection.
Mean score from the Spine Adverse Events Severity System, reported with 95% CIs. If the grade was identical for all of the events or if there was only one adverse event in the category, then standard deviation was zero and confidence intervals could not be generated.
Increased LOS was recorded categorically (none, 1–2 days, 3–7 days, 8–14 days, 15–28 days, or more than 28 days), so mode is presented in this table.
Discussion
Types of surgeries can be stratified into low, intermediate, or high risk (Fig. 1). Low-risk procedures (3 to 8% complication rate) included posterior one-level, all primary anterior, and revision two-level anterior surgery. Intermediate-risk procedures (9 to 20% complication rate) included revision one-level posterior, revision one- and three-plus-level anterior, and primary combined procedures. High-risk procedures (21 to 38% complication rate) included multilevel posterior, revision multilevel posterior, and revision combined procedures. Types of complications in the high-risk groups spanned the range of recorded adverse events, with particularly high rates of delirium and draining wounds (Table 2). Rates of complications were generally higher for revision surgery than for primary surgery, which held true for anterior one-level surgery, anterior multilevel surgery, posterior one-level surgery, and combined surgery. In general, the complication rates increased as more motion segments were involved. This trend was noted for primary anterior, primary posterior, and revision posterior procedures but was not consistent for revision anterior surgery.
Patients who have surgery from a posterior approach are more likely to have complications than patients who have surgery from an anterior approach. 2 We detected a three-fold increase in complication rates for patients who had a posterior procedure (22.9%) compared with patients who had an anterior procedure (7.48%). The rate of complications for combined front–back procedures (23.94%) was only slightly higher than the rate for posterior procedures (Table 4, summarized in Fig. 2), which agrees with findings reported by Shamji et al, who retrospectively reviewed a database of 8,548 patients who underwent either multilevel anterior or posterior cervical surgery. 3 Patients in their series who had posterior surgery were generally older and had more medical comorbidities than patients who had anterior surgery. But even when they controlled for population demographics, they identified increased morbidity and hospital resource utilization from the posterior approach.
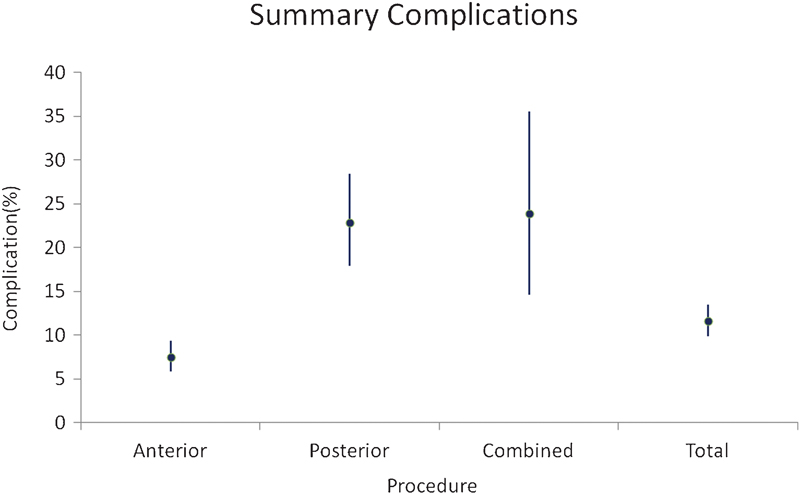
Summary of complication rates. Error bars represent 95% confidence intervals. Anterior procedures had a significantly lower rate of complications than posterior and combined procedures.
The rates of complications in this prospectively gathered series are comparable to those found in other studies. For single-level and multilevel anterior procedures, the rates of dysphagia in this series were 0.71 and 1.37%, respectively. Veeravagu et al reported slightly higher rates of 1.15 and 1.96% in their retrospective database review of 28,777 patients who underwent anterior cervical diskectomy and fusion. 4 Fountas et al retrospectively reviewed 1,015 patients who received primary single- or multilevel ACDF. 5 Their reported rate of death (0.1%) was similar to that found for anterior procedures in this series (0.13%), although they looked only at ACDFs and this study did not distinguish between multilevel ACDF and other types of anterior procedures such as corpectomies. However, compared with this series, Fountas et al found higher rates of dysphagia (9.5 versus 0.13%) and hematoma requiring reoperation (2.4 versus 0.13%), but slightly lower rates of dural tear (0.5 versus 1.6%) and superficial infection (0.1 versus 0.4%). They also reported on complications that were absent in this study: recurrent laryngeal nerve palsy (3.1%), esophageal perforation (0.3%), worsening of preexisting myelopathy (0.2%), and Horner syndrome (0.1%). Complication rates found in this series for dural tear, hematoma, and superficial infection were also very similar to those reported in the retrospective single-surgeon series of 1,576 patients by Nanda et al. 6
The main strength of this database is that the data was gathered prospectively, from multiple centers in North America, over a recent and short period (all surgeries were performed between 2008 and 2011). Twenty-six different types of adverse events were reported by clinicians. There were 1,269 patients who had adequate documentation for inclusion, which is relatively large for a series of prospectively gathered data on perioperative complications. By comparison, Fehlings et al reported on prospectively gathered perioperative complications for 302 patients who had surgery for spondylotic myelopathy, 7 and Campbell et al reported on 119 patients. 8
The main weakness of this data set is the poor follow-up (41% at 3 months). As previously stated, similar rates for certain complications (such as dysphagia 4 ) were found between this study and others, which helps to validate the data. But the relatively low rates of other complications (such as hematoma 5 ) and absence of others (such as esophagus injury 5 ) cast some doubt on the applicability of the data set. Another possible weakness of this study is potential underreporting. Busy clinicians may be more likely to remember to document rare and dramatic adverse events such as dural tears and epidural hematomas but less likely to remember to report complications that seem to be more mundane or common, such as delirium. Despite the size of the study, 12 of 26 types of complications (almost half) had four or fewer events. As a result, we are unable to comment on preoperative risk factors, which have been reported in other recent studies. 9 Furthermore, certain rare “surgery-specific” complications, such as vertebral artery injury and Horner syndrome, do not appear in this series at all. Additionally, not all of the complications may be directly related to the procedure. Without a prospective system to evaluate relatedness, it is difficult to determine the relevance of some of the medical complications. There is also the possibility for bias in follow-up because patients who have problems may be more likely to present for clinic visits than those who are doing well.
This data can be used to counsel patients preoperatively regarding their medical and surgical risks. For example, if a patient is considering a one-level primary anterior procedure, his or her chance of having any complication is 4.98% (Table 1). If a patient is offered a revision multilevel posterior procedure, his or her chance of having any complication is 28.57% (Table 2). Fortunately, the risk of the most severe complications in all of cervical spine surgery (death or paraparesis) is low, at 0.24% (Table 4). Furthermore, patients who have undergone cervical spine surgery and have suffered an adverse event can be counseled regarding the consequences. For example, if a patient has a dural tear after cervical spine surgery, based on Table 5 they can expect that the adverse event will probably require minor treatment but have no long-term effect (grade 2), and their hospital stay will likely be extended for 3 to 7 days.
Clinicians should be particularly vigilant for perioperative complications that occurred in this data set at the highest frequency, such as dysphagia, cardiac complications, shortness of breath, and delirium (Table 4). This information can also be used to inform administrators as they perform internal quality reviews. This data set also serves as a reminder to policy makers and insurance companies who are moving away from fee for service in favor of reimbursement based on “quality” of care. Data from this series was gathered from some of the premiere academic institutions in North America, and there was still an 11.58% overall perioperative complication rate for patients who had cervical spine surgery.
Conclusion
Perioperative complication rates in cervical spine surgery are significantly lower in younger patients, surgery performed through an anterior approach (compared with a posterior or combined approach), with fewer levels involved (particularly in posterior surgery), and in primary (compared with revision) procedures. Anterior surgery resulted in more respiratory problems, dysphagia, dysphonia, and implant malposition, and posterior surgery resulted in more wound-healing problems and cardiac complications.
Disclosures
Steven Leckie, none
S. Tim Yoon, consultancy: Stryker Spine, Meditech Spine; royalties: Stryker Spine, Meditech Spine; grants: AOSpine North America
Robert Isaacs, grants: Nuvasive; consultancy: Nuvasive, Baxano Surgical, Vertera; royalties: Nuvasive, Baxano Surgical, Vertera; travel support: ACSR Research Group, Vertera; board membership: Saferay Spine; scientific advisor: Providence; stock: Providence, Saferay Spine, Safewire, Vilaspine, Vertera
Kris Radcliff, board membership: ACSR; consultancy: Medtronic, Depuy, Globus; grants: Depuy, Paradigm, Medtronic; royalties: Globus; travel support: Globus, Depuy, Medtronic, Stryker
Richard Fessler, consultancy: Depuy, Stryker, Medtronic; grants: Medtronic; patents: Medtronic; royalties: Medtronic
Regis Haid, Jr, consultancy: Nuvasive; payment for lectures: Globus, Nuvasive; patents: Medtronic; royalties: Medtronic; stock: Globus, Nuvasive
Vincent Traynelis, grants: Medtronic; travel support: Medtronic; consultancy: Medtronic; patents: Medtronic; royalties: Medtronic; institutional fellowship support: Globus
Footnotes
Acknowledgments
The authors acknowledge the Association for Collaborative Spinal Research (ACSR) and George Cotsonis, PhD (Emory University Department of Biostatistics).