
Abstract
Study Design
Case series of seven patients.
Objective
C2 stabilization can be challenging due to the complex anatomy of the upper cervical vertebrae. We describe seven cases of C1–C2 fusion using intraoperative navigation to aid in the screw placement at the atlantoaxial (C1–C2) junction.
Methods
Between 2011 and 2014, seven patients underwent posterior atlantoaxial fusion using intraoperative frameless stereotactic O-arm Surgical Imaging and StealthStation Surgical Navigation System (Medtronic, Inc., Minneapolis, Minnesota, United States). Outcome measures included screw accuracy, neurologic status, radiation dosing, and surgical complications.
Results
Four patients had fusion at C1–C2 only, and in the remaining three, fixation extended down to C3 due to anatomical considerations for screw placement recognized on intraoperative imaging. Out of 30 screws placed, all demonstrated minimal divergence from desired placement in either C1 lateral mass, C2 pedicle, or C3 lateral mass. No neurovascular compromise was seen following the use of intraoperative guided screw placement. The average radiation dosing due to intraoperative imaging was 39.0 mGy. All patients were followed for a minimum of 12 months. All patients went on to solid fusion.
Conclusion
C1–C2 fusion using computed tomography-guided navigation is a safe and effective way to treat atlantoaxial instability. Intraoperative neuronavigation allows for high accuracy of screw placement, limits complications by sparing injury to the critical structures in the upper cervical spine, and can help surgeons make intraoperative decisions regarding complex pathology.
Introduction
Atlantoaxial instability can result from congenital malformations, systemic inflammatory conditions, neoplasms, and spinal trauma. C1–C2 stabilization can be challenging due to the complex anatomy of the C1 and C2 vertebrae. The proximity of neurovascular structures, the variability of vertebral artery anatomy, and the degree to which upper cervical pathology can distort normal anatomical structures calls for very precise placement of instrumentation to avoid surgical complications. 1 , 2 , 3 , 4 Various techniques have been developed to accomplish upper cervical fixation.5, 6 , 7 Posterior C1 lateral mass and C2 pedicle screw–rod fixation, as described by Harms and Melcher, is a widely accepted, safe, and effective method to achieve fusion. 8 , 9 , 10 , 11
Traditionally, intraoperative fluoroscopy has been used to aid in instrumentation. 12 , 13 However, just as surgical techniques have advanced through the years, imaging modalities have as well. Three-dimensional intraoperative imaging with navigation has been implemented to help surmount some of the technical difficulties of screw placement in the upper cervical spine. These intraoperative tools increase the accuracy of screw placement in the spine and aid in the surgical decision making. 14 , 15 , 16 , 17
Studies have shown that O-arm usage allows for accurate screw placement in various levels of the cervical spine. 14 , 18 , 19 , 20 When compared directly with conventional fluoroscopy, the O-arm has been shown to increase the accuracy of screw placement in the lower cervical spine. 21 Considering the unique challenges presented by surgically stabilizing the first two cervical vertebrae, we examined the surgical outcomes, radiation exposure, and accuracy of screw placement. Consequently, the purpose of this study is to provide evidence that the use of intraoperative neuronavigation improves the safety and efficacy of surgical fixation in treating instability at the complex C1–C2 region.
Methods
Seven patients (2 men, 5 women) with atlantoaxial instability underwent stabilization from February 2011 to January 2014. The mean age was 55.3 years (range 37 to 76). Patients presented with a range of conditions leading to C1–C2 instability including rheumatoid arthritis, odontoid fracture, C2 fracture, and ligamentous injury (Fig. 1). Table 1 shows the patient demographic data.
Demographics
Abbreviation: SD, standard deviation.
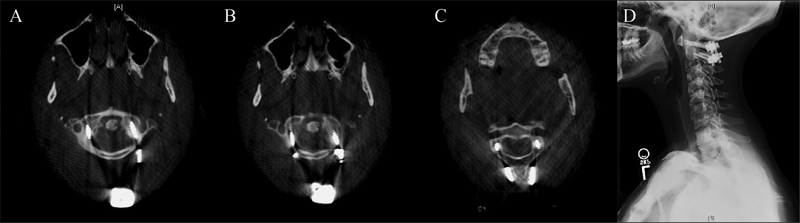
A 43-year-old woman with rheumatoid arthritis, neck pain, and C1–C2 instability. (A, B) Postoperative computed tomography (CT) scans showing placement of C1 lateral mass screws. (C) Postoperative CT scan showing C2 pedicle screws. (D) Lateral cervical X-ray demonstrating C1–C2 fusion 12 months after surgery.
From February 2011 to January 2014, all instances of atlantoaxial stabilization performed at our institution by a single surgeon were included in this study. The case series was approved by the Institutional Review Board at our institution. In all seven cases, O-arm imaging and navigation were used. The radiologic evaluation was performed preoperatively and included plain X-rays in the lateral and anteroposterior planes as well as cervical computed tomographic (CT) scans and/or magnetic resonance imaging. Operative data such as blood loss, complications, and operative time, defined as time from first incision to closure, was gathered from the anesthesia record. Outcome measures included the neurologic status, screw placement, and fusion rates. These clinical parameters were reviewed independently from the radiologic data. Data is reported as averages ± standard deviation or standard error of measure.
Patients were positioned prone on the Jackson table with a Wilson frame. The patient's head was placed in Mayfield pins and aligned in a neutral position. Lateral X-ray was obtained to assess the proper alignment and reduction. After the standard exposure was achieved, the navigational reference frame was attached to the spinous process of C3. Our institution uses the O-arm, a cone-beam CT scanner that, paired with the StealthStation Surgical Navigation System (Medtronic, Inc., Minneapolis, Minnesota, United States), allows for stereotactic intraoperative imaging and navigation in multiple planes. An intraoperative CT scan with the O-arm was performed. The images were transferred to the StealthStation navigation system, and the trajectories were planned in the C1 lateral mass and C2 pedicles. The stereotactic wand was utilized to verify the appropriate trajectory.
Pilot holes were drilled bilaterally in C1 and C2, and O-arm navigation was used to maintain course. Once the drilling was completed, a ball-tip probe was used to verify the integrity of the holes prior to final screw placement. The optimal screw length was calculated and the screws were placed under image guidance so that the appropriate positioning and good purchase were achieved. After screw placement, the screw trajectory was verified, and rods were placed into the screw heads and tightened. Decortication was performed and the bone that was removed during the procedure was morselized and placed along the construct.
The screw placement accuracy was determined from the postoperative CT scans that were analyzed by an independent neuroradiologist. The assessment of radiologic data was blinded from the clinical outcomes. Screw placement was graded based on previously characterized grading systems for C1–C3 lateral mass and C2 pedicle screws. 3 , 22 Briefly, screw position for lateral mass screws was defined as type I for ideal placement without cortical violation, type II for acceptable placement with 50% of the diameter located within surrounding cortex and less than 1-mm protrusion from the anterior cortex, and type III for unacceptable placement with clear violation of the transverse foramen or spinal canal. 22 The medial and lateral displacement of the C2 pedicle screws was defined as previously described 3 : grade 0, no deviation; grade 1, deviation less than 2 mm; grade 2, deviation more than 2 mm and less than 4 mm; grade 3, deviation more than 4 mm. Patients were followed clinically at increasing intervals after surgery with imaging to evaluate the fusion progression.
Results
No complications occurred during surgery, such as vertebral artery, nerve root, or spinal cord injury. The initial intraoperative CT was used to determine the proper cervical alignment of the patient; no patients required repositioning prior to the surgery. The mean operative time was 188.7 minutes (range 155 to 213), and the mean blood loss was 271.4 mL (range 50 to 900). The patients received on average 39.0 mGy of radiation with use of the O-arm. Values from the operative records are shown in Table 2.
Operative characteristics
Abbreviation: SD, standard deviation.
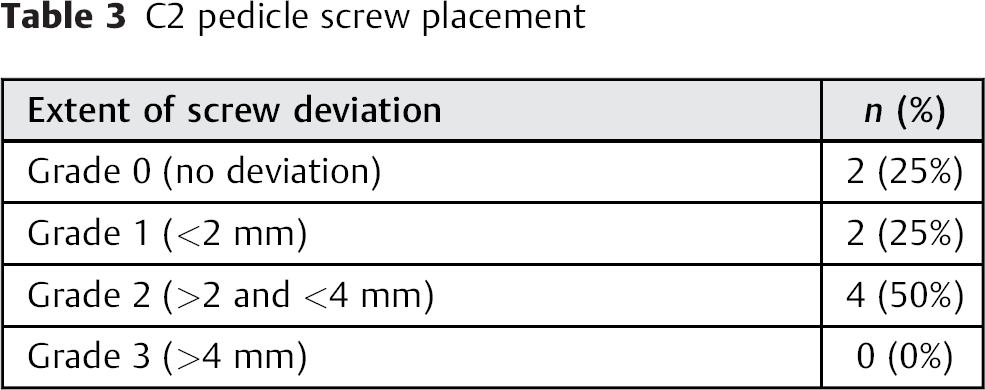
A total of 30 screws were placed in the cervical spine: 14 screws (46.7%) in C1, 8 screws (26.7%) in C2, and 8 screws (26.7%) in C3. In three instances, the C2 anatomy was determined to be not conducive to screw placement, so C3 was used as the site of instrumentation instead. This C2 anatomy was not evident on the preoperative CT. In one instance, it was deemed necessary to place the screws in each of the first three cervical vertebrae. A total of two pedicle screws (25%) were classified as grade 0 (Table 3). Two screws (25%), 4 screws (50%), and 0 screws (0%) were graded as 1, 2, and 3, respectively (Table 3). All C2 pedicle screws deviated medially. The average deviation for all C2 pedicle screws was 1.5 mm, and no screws had cortical violation. The lateral mass screws placed in the first and/or third cervical vertebra had an average deviation of 2.1 mm. All but two were classified as type I or ideal placement (Table 4). No screws required repositioning.
C2 pedicle screw placement
CT findings regarding C1–C2–C3 screw placement accuracy
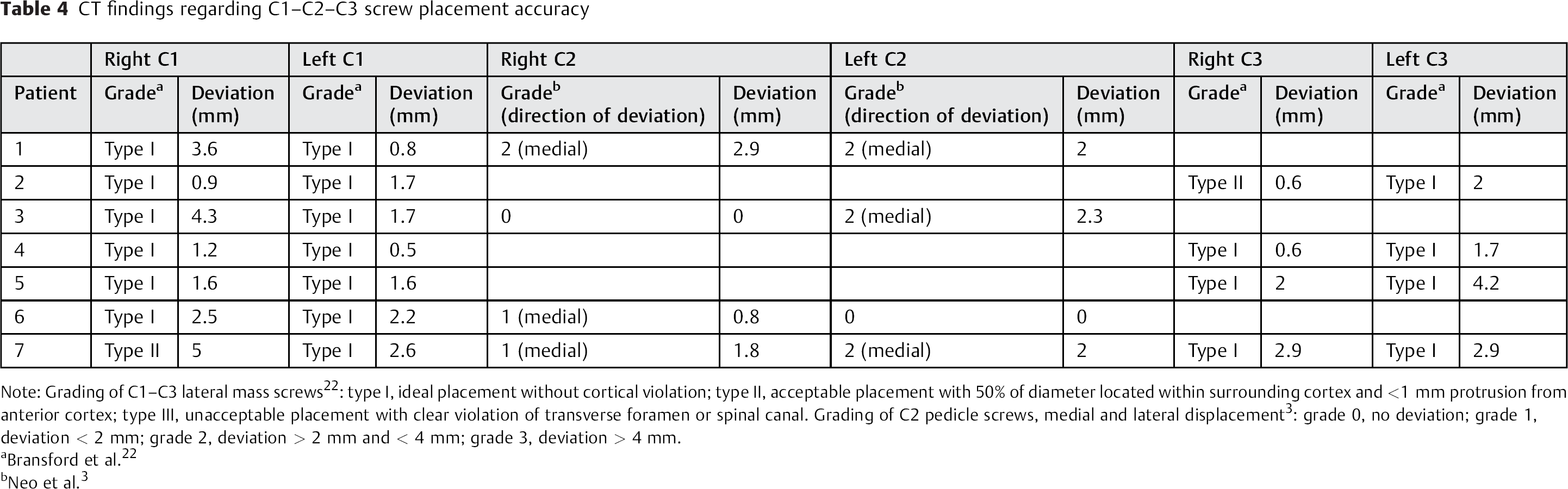
Note: Grading of C1–C3 lateral mass screws 22 : type I, ideal placement without cortical violation; type II, acceptable placement with 50% of diameter located within surrounding cortex and <1 mm protrusion from anterior cortex; type III, unacceptable placement with clear violation of transverse foramen or spinal canal. Grading of C2 pedicle screws, medial and lateral displacement 3 : grade 0, no deviation; grade 1, deviation < 2 mm; grade 2, deviation > 2 mm and < 4 mm; grade 3, deviation > 4 mm.
Bransford et al. 22
Neo et al. 3
The postoperative course was uneventful for all patients. The average length of stay was 2.7 days (range 1 to 6). The mean follow-up was 12 months for patients who underwent atlantoaxial fusion. At follow-up, only one patient showed motion on flexion–extension films, but subsequent CT imaging demonstrated intact instrumentation and solid fusion. The patients largely saw improvement in symptoms and were pleased with the surgery. All patients showed signs of fusion on X-ray performed at 12 months.
Discussion
Intraoperative CT combined with navigation is a useful technology that offers significant advantage in the operating room. It enables the surgeon to precisely track the trajectory of surgical instruments and can improve hardware placement. Intraoperative imaging provides the advantage of capturing the patient's anatomy in the surgical position, which is particularly helpful in cases with complex anatomy or where pathology distorts the normal anatomic structure, as can occur with C1–C2 pathology. In fact, a mounting body of evidence has shown that intraoperative navigation can improve the accuracy of screw placement during spine surgery and the intraoperative anatomical localization and can reduce morbidity. 23 , 24
Although both the O-arm and conventional fluoroscopy are used intraoperatively, the O-arm has an advantage in that it produces a three-dimensional image. As such, it allows the surgical team to ensure that the patient's vertebrae are aligned in the axial plane in addition to the lateral and oblique planes (as provided by fluoroscopy). This multidimensional visualization correlates with the intraoperative findings, which is particularly important because the simple act of turning the patient prone can produce a discrepancy between the preoperative CT imaging and the intraoperative surgical anatomy and alignment. 25
One of the main concerns with screw placement in the superior cervical vertebrae is direct vertebral artery injury. Lateral displacement of the screw can compromise the medial border of the transverse foramen. With the use of intraoperative navigation, the trajectory of each screw can be easily visualized to ensure the vertebra can safely accept a screw, the bony course is able to be maintained, and the surrounding structures including vertebral artery, nerve root, or spinal cord are not injured.
The combination of the O-arm imaging and StealthStation navigation suite allows the surgeon to plan the trajectories in the complicated spinal anatomy. This tool can help navigate difficult cases, as mentioned by Acosta et al, who reported that 24% of their screws could not have been safely placed without intraoperative imaging. 26 In our experience, three patients who underwent treatment for atlantoaxial subluxation had screws placed in C3 instead of C2, because the C2 anatomy was deemed inappropriate for screw placement. This decision about the surgical approach would otherwise not have been made without intraoperative imaging and trajectory planning.
As mentioned earlier, placing screws into the C1 and C2 vertebrae can be difficult, especially when inserting screws into the C2 pedicles. Despite these difficulties, the pedicles are desired targets for screws in the C2 vertebrae because they offer much better biomechanical stability. 27 , 28 , 29 , 30 Relying only on conventional means, meta-analysis has shown a misplacement rate of C2 pedicle screws from 0.9 to 44.7%. 31 , 32 , 33 , 34 , 35 Misplacement in the C1 and C2 vertebrae can be particularly dangerous due to the potential for damage to the surrounding neurovasculature structures. 3
Navigation has been used to mitigate the difficulties of pedicle screw placement with positive results, showing a misplacement rate from 1 to 11.1%. 15 , 17 , 19 , 20 , 35 , 36 , 37 Van de Kelft et al placed 1,922 pedicle screws in 353 patients at the thoracic, lumbar, and sacral levels with a 97.5% accuracy using the O-arm and StealthStation navigation. 17 Also using intraoperative neuronavigation, Larson et al reported a 98.2% accuracy rate in 1,511 pedicle screws placed in adults. 36 At the cervical spine, Ishikawa et al noted that of 108 pedicle screws, 88.9% had no perforation, 8.3% had less than 2 mm of perforation, and 2.7% were between 2 and 4 mm outside of the bone. 19 Ling et al reported that 98% of their screws were placed in ideal positions in 21 patients treated with a Harm's construct or occipital cervical fusion using the O-arm, though 2 of the 20 placed in the C2 pedicle deviated by 1 mm. 20 In our case series, 90% had less than 4 mm of deviation from the ideal trajectory. In our study, no screws required removal and replacement. The ability to correct screw placement if necessary in the operating room is advantageous and may prevent reoperation for anatomical misalignment and/or poorly placed screws.
Despite the benefits of utilizing O-arm technology, some potential drawbacks do exist. As with any form of CT, radiation doses are a concern with O-arm imaging. Although the operating staff are able to leave the room and avoid virtually any radiation exposure, 38 published numbers show that O-arm patients undergo a higher level of radiation (highest tissue dose = 40 mGy with two O-arm scans) than they would with conventional fluoroscopy (highest tissue dose = 6 mGy). 39 Tabaraee et al investigated the radiation dose to cadavers following exposure by either the C-arm or O-arm. The study found cadavers received higher doses of radiation with the use of the O-arm, even though the cadavers exposed to C-arm radiation also had a postoperative conventional CT scan. 40 The risks of increased radiation exposure must be weighed with the benefits of utilizing the O-arm technology.
One reported limitation of intraoperative neuronavigation includes the increased operative time involved to acquire intraoperative CT images and navigation registration. The mean operative times for atlantoaxial fusion vary greatly in the literature. 25 , 41 , 42 Yang et al compared C1 lateral mass and C2 pedicle screws placed with conventional fluoroscopy to iso-C three-dimensional navigation and found no significant difference in operative times. 42 In our center, we can acquire data in 18 to 20 minutes from the time the O-arm is positioned and draped and the intraoperative CT is completed. This time is comparable to the time it takes us to set up and access images with biplanar fluoroscopy. Further comparisons between intraoperative navigation and conventional methods for screw placement are necessary to determine if any benefit or detriment exists in operative times with newer technology.
Another problem that can arise from O-arm usage is the potential navigation errors. The navigation reference frame has to be attached to a fixed point on the patient, and any movement that dislodges the reference frame will result in a navigational error. Oftentimes the reference frame is attached to the spinous process of C3 or another vertebra, which has the potential for slight movement during procedures. The operating team must take steps to ensure that the reference frame is fixed throughout the entire procedure. Even with the reference frame in the right position, the O-arm is reported to have an inherent amount of error. Oertel et al found a 2.8 ± 1.9-degree difference between the angulation of the actual and virtual pedicle screws. 43 When compared with actual dissection of human cadavers, Santos et al discovered that the overall accuracy of the O-arm images in depicting pedicle screw placement in the thoracolumbar spine was only 73%. 44 Errors related to navigation may lead to inaccuracies during screw placement.
Conclusion
Our experience with C1–C2 fusion shows that O-arm imaging and navigation can offer adequate screw placement accuracy without complications and with good surgical outcomes. This robust technology can assist in the placement of instrumentation during difficult procedures like atlantoaxial fixation. Further investigation may include minimally invasive surgery using intraoperative navigation and performing a cost–benefit analysis comparing the O-arm with other imaging modalities and navigation.
Disclosures
Jacob D. Smith, none
Megan M. Jack, none
Nicholas R. Harn, none
Judson R. Bertsch, none
Paul M. Arnold, Consultant: Medtronic Sofamor Danek, Stryker Spine, FzioMed; Travel/meeting expenses: AOSpine North America