
Abstract
Study Design
Retrospective evaluation of prospectively collected data.
Objective
To evaluate infection rates following intrawound vancomycin powder application during spine tumor surgery.
Methods
Patients ≥18 years old undergoing spine tumor surgery and receiving intrawound vancomycin powder at a single center between January 2008 and January 2015 were enrolled. Patient demographics (age, sex, body mass index [BMI]), tumor type (metastatic, primary) and location, surgical data (estimated blood loss [EBL], levels fused, type of decompression, length of surgery and hospitalization, discharge status from hospital), radiation therapy use, and infection rates (surgery to a minimum of 30 days postoperative) were evaluated.
Results
Forty patients (46 procedures) undergoing spine tumor surgery and intrawound vancomycin powder application were identified. Five were excluded because of death less than 30 days postoperatively, and 35 patients (41 procedures) were enrolled: 11 women and 24 men with an average age of 61.4 years (range 19 to 92) and average BMI of 27.3 (range 17.4 to 36.8). Three cases were primary spine tumors. Five were hematologic malignancies, and 27 were metastatic cancers. Twenty-one tumors were in the thoracic spine, 12 in the lumbar spine, and 8 in the cervical spine. Average EBL was 899 mL (range 25 to 3,500), average length of surgery was 241 minutes (range 78 to 495), and average hospital stay was 15.1 days (range 3 to 49). Two culture-proven infections (Staphylococcus aureus, Enterobacter cloacae) were noted in 41 procedures (4.9%). Ten patients (28.6%) had preoperative radiation only; 14 (40%) had postoperative radiation only, 5 (14.3%) had both preoperative and postoperative radiation, and 6 (17.1%) had no radiation. There were no associations between radiation treatment and postsurgical infections (p = 0.19).
Conclusion
In this first study evaluating intrawound vancomycin powder for spine tumor surgery, we report an infection rate of 4.9%. We found no correlations between radiation treatment and postsurgical infections.
Introduction
Superficial or deep surgical site infections (SSIs) are risk factors of spine surgery. Once SSIs develop, expenses associated with patient care can significantly increase. 1 SSIs are metrics followed closely by insurance carriers, and Medicare does not cover the extra costs associated with SSIs. For decompression procedures (laminectomy, diskectomy), infection rates as low as 0.7% have been reported. 2 However, rates of SSI greater than 30% have been reported in the surgical management of primary or metastatic spine tumors. 3
Recently, the application of intrawound vancomycin powder has led to decreased infection rates following surgery for spine deformity, spine trauma, and degenerative conditions of the spine. 4 , 5 Animal studies have also shown the efficacy of intrawound vancomycin powder in eradicating infections. 6 In addition, a growing body of evidence supports a large cost benefit associated with the use of intrawound vancomycin powder when compared with the cost of reoperation. 7
To our knowledge, no studies to date have specifically evaluated the infection rates following intrawound application of vancomycin powder for spine tumor surgery. Our objective was to evaluate infection rates following intrawound vancomycin powder application during spine tumor surgery.
Materials and Methods
The study was a retrospective evaluation of prospectively collected data. Institutional Review Board approval was obtained for the study. Patients 18 years of age and older undergoing spine tumor surgery with application of intrawound vancomycin powder from January 2008 to January 2015 were identified and enrolled. Two surgeons from a single tertiary care academic center participated in this study. All patients enrolled had either primary, hematologic, or metastatic tumors of the cervical, thoracic, and/or lumbar spine. Patients with sacral tumors were excluded because a multidisciplinary team operates on these patients at our center. Patients with postsurgical survival of less than 30 days were also excluded from the study. All patients received a standard dose of first-generation intravenous cephalosporin for surgical prophylaxis prior to the skin incision in addition to 1 g of intrawound vancomycin powder prior to closure of the deep fascia and subcutaneous tissue. In anterior cervical spine surgeries, we used 250 mg of intrawound vancomycin powder. Patients with penicillin allergies received 900 mg of intravenous clindamycin instead. Perioperative parental antibiotics were continued for at least 24 hours according to institutional policy. Subfascial drains were placed in all patients and were removed at the discretion of the operating surgeon.
Our primary outcome was SSI within 30 days of surgery. We also collected perioperative complications including postoperative infection (0 to 90 days postoperatively), length of hospital stay, and discharge status (home versus rehab). For each procedure, wound complications or suspected wound infections were further scrutinized and the causative organisms were identified by Gram stain and/or culture-positive data.
Patient demographics including age, sex, body mass index, significant comorbidities (hypertension, diabetes, and obesity), tumor type, and location were identified. The following surgical data was collected: levels fused, preoperative/postoperative radiation therapy use, blood loss, intraoperative complications, duration of procedure, surgical approach (anterior only versus posterior only versus combined anterior and posterior), and use of operative microscope. We also evaluated patient survival at the latest follow-up.
The Student t test and Fischer exact test were used with significance set at p < 0.05.
Results
Demographics
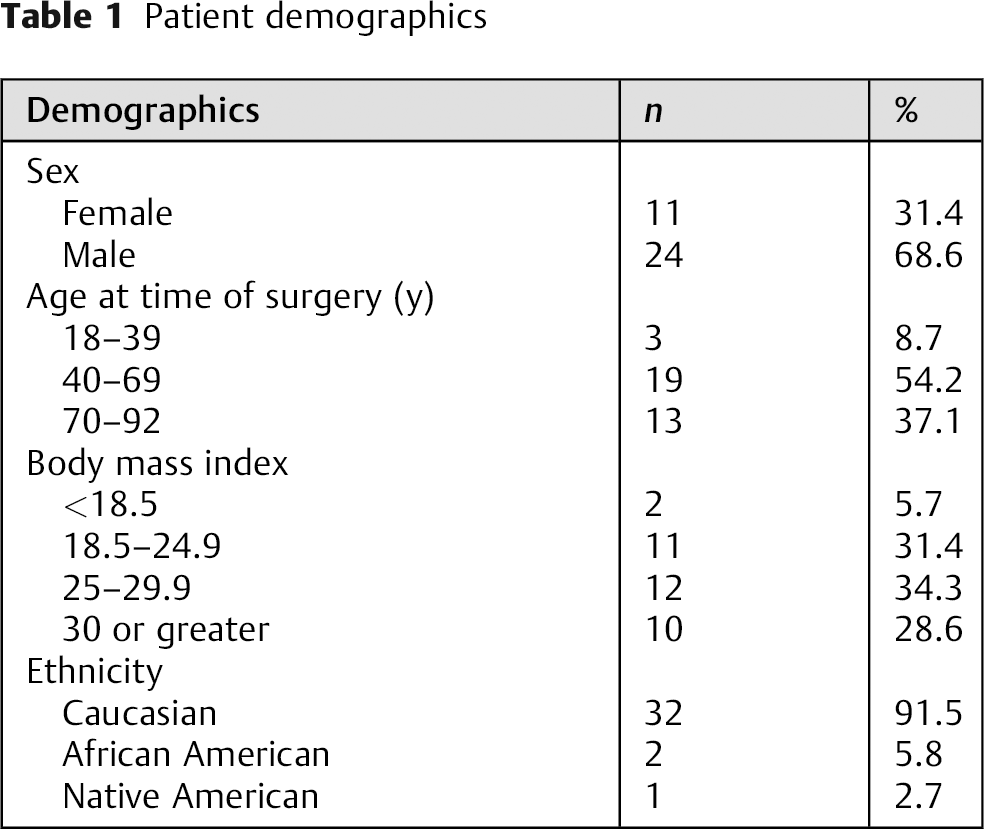
A total of 40 patients undergoing spine tumor surgery (46 procedures) with intrawound vancomycin powder application were identified. Five were excluded because of death less than 30 days postoperatively, and 35 patients (41 procedures) were enrolled (Table 1): 11 women and 24 men with an average age of 61.4 years (range 19 to 92) and average body mass index of 27.3 (range 17.4 to 36.8). At latest follow-up, 15 of the 35 (43%) were deceased as a result of their malignancy.
Patient demographics
Tumor Data
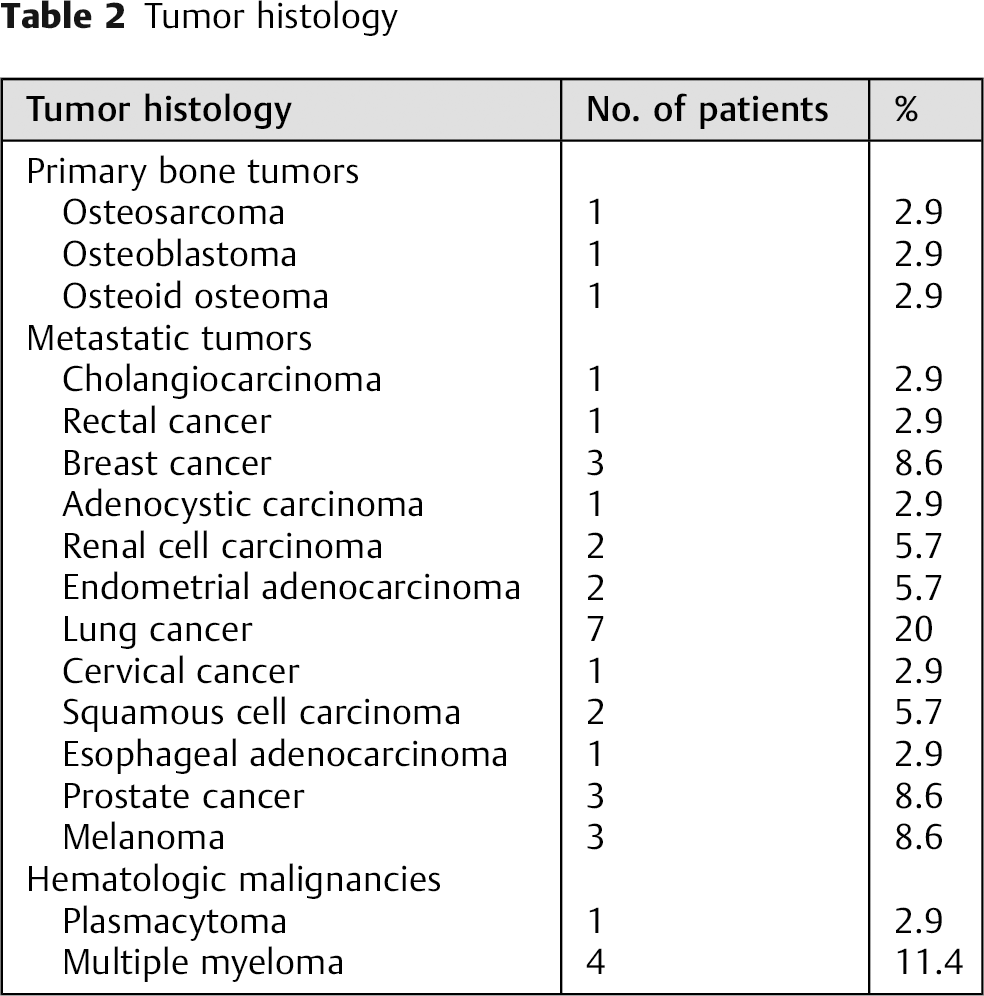
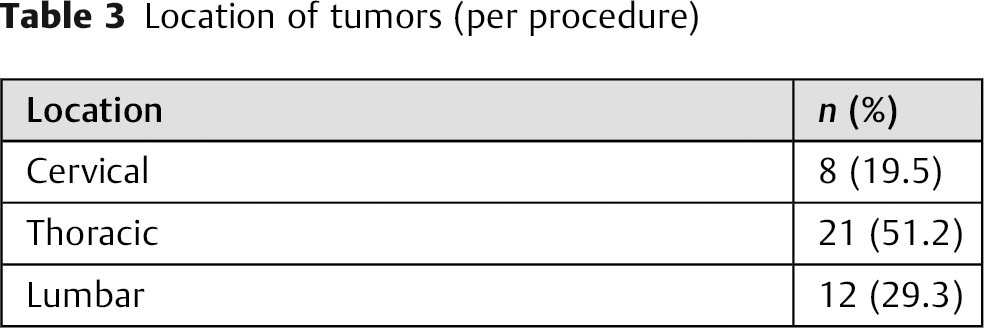
Three cases were primary spine tumors, 5 were hematologic malignancies, and 27 were metastatic cancers (Table 2). All the tumors were extradural. The most common metastatic tumors were lung cancer (n = 7), breast cancer (n = 3), melanoma (n = 3), and prostate cancer (n = 3). The most common hematologic malignancy was multiple myeloma (n = 4). The three primary bone tumors were osteosarcoma, osteoid osteoma, and osteoblastoma. Twenty-one tumors were in the thoracic spine, 12 in the lumbar spine, and 8 in the cervical spine (Table 3).
Tumor histology
Location of tumors (per procedure)
Surgical Data
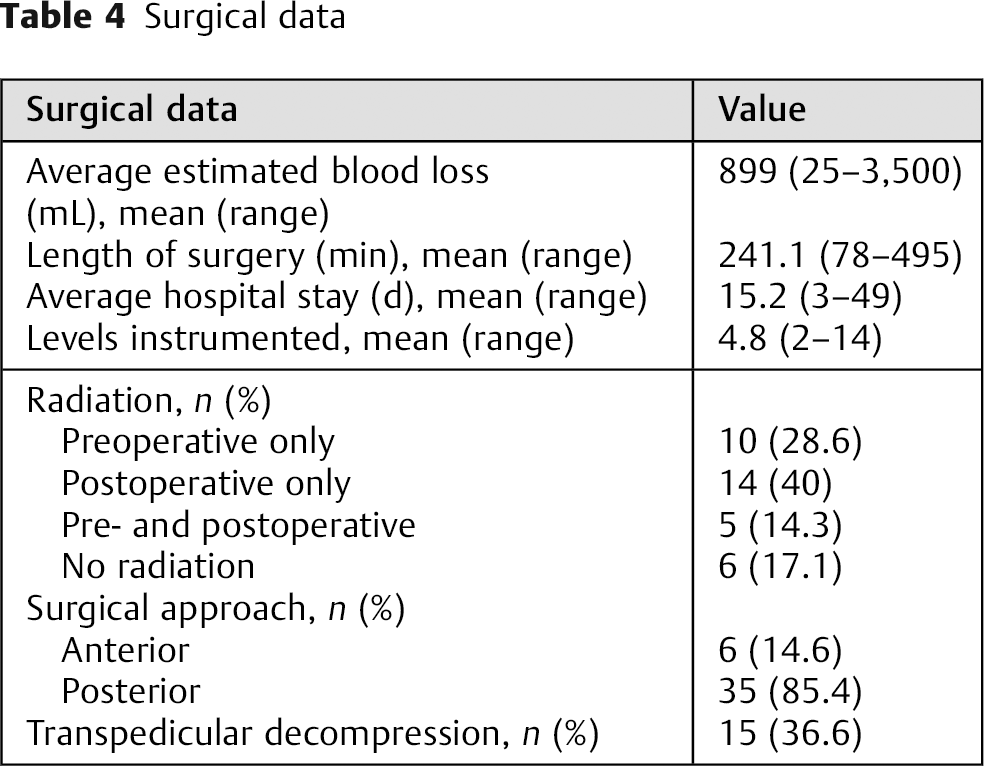
The average estimated blood loss was 899 mL (range 25 to 3,500); 3 patients underwent decompression only and 32 underwent decompression and instrumented fusions (Table 4). Fifteen patients underwent transpedicular decompressions, and an average of 4.8 levels (range 2 to14) were instrumented and fused. The average length of surgery was 241 minutes (range 78 to 495), and the average hospital stay was 15.1 days (range 3 to 49). Ten patients (28.6%) had preoperative radiation only, 14 (40%) had postoperative radiation only, 5 (14.3%) had both pre- and postoperative radiation, and 6 (17.1%) had no radiation. There were no associations between radiation treatment and postsurgical infections (p = 0.19).
Surgical data
Complications per Procedure
Intraoperative
There were 3 incidental durotomies (Table 5); 1 with medial breach at L1 during pedicle screw placement and 1 with arterial bleeding requiring vascular surgery ligation. Four cases had intraoperative neuromonitoring changes; 2 of the 4 patients had postoperative motor weakness.
Surgical and medical complications
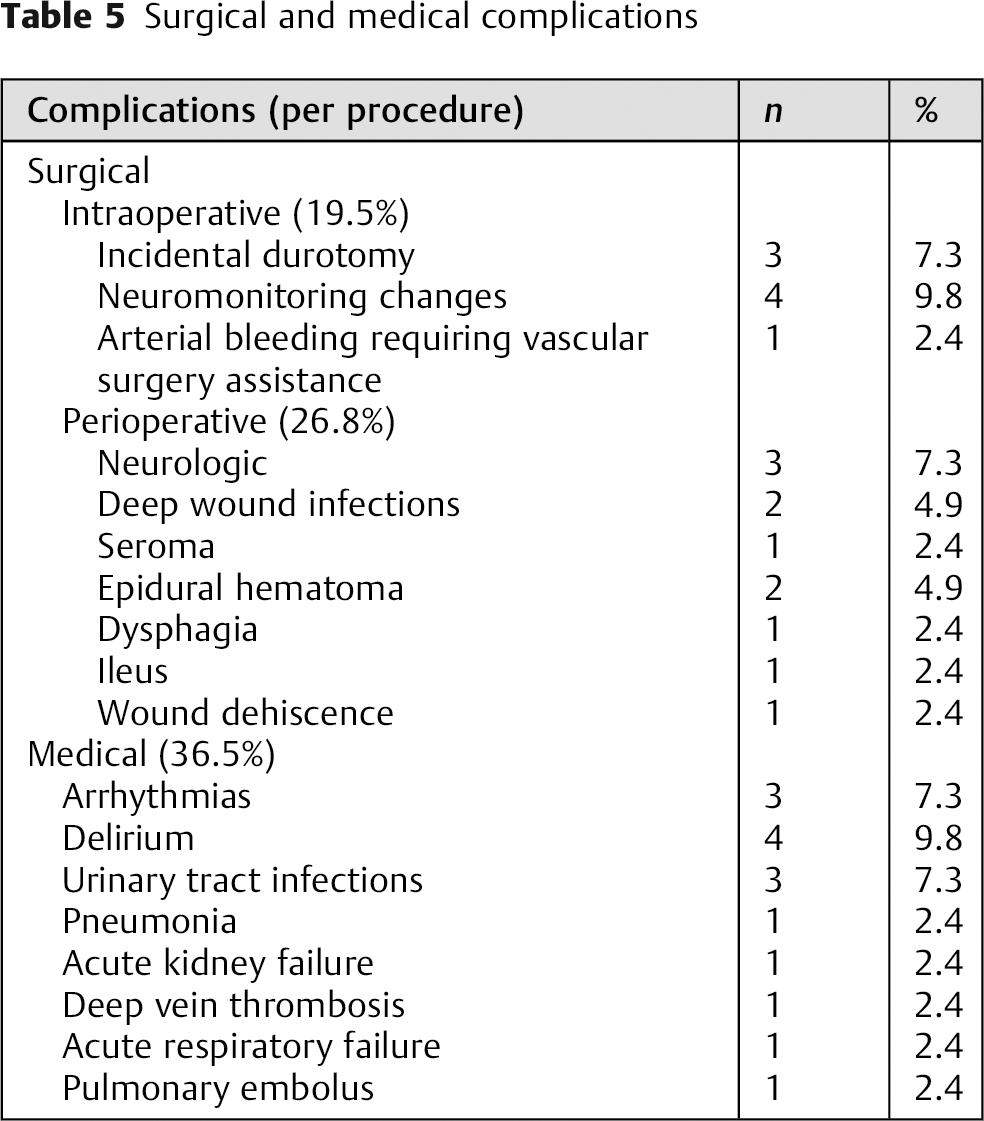
Perioperative
Surgical complications occurred in 26.8% of the patients: 3 neurologic complications (2 cases of motor weakness, 1 thoracic radiculopathy), 2 deep wound infections, 1 sterile seroma, 1 epidural hematoma requiring operative evacuation, 1 hematoma aspirated by interventional radiology, 1 severe dysphagia requiring temporary percutaneous endoscopic gastrotomy tube placement, 1 wound dehiscence, and 1 ileus requiring nasogastric tube placement. Two culture-proven infections (Staphylococcus aureus, Enterobacter cloacae) were noted in 41 procedures (4.9%). The infections were treated with irrigation and debridement and antibiotic administration. The 1 case of seroma was managed with irrigation and debridement with negative intraoperative cultures.
Medical complications occurred in 36.5% of the patients. The following medical complications were identified: 3 arrhythmias, 4 cases of postoperative delirium, 3 urinary tract infections, 1 pneumonia, 1 acute kidney failure, 1 deep vein thrombosis, 1 pulmonary insufficiency requiring reintubation, and 1 pulmonary embolus.
Discussion
SSIs are common complications of spine tumor surgery. 3 , 8 , 9 , 10 Radiation therapy prior to the surgery, corticosteroid use, poor nutritional status, poor wound healing, and immunocompromised hosts are contributing factors for SSIs in patients with cancer. 3 , 9 The skeletal system is the third most common site of metastasis, and the spine is the number one site of skeletal metastases. 11 With the aging population, spine surgeons will be managing more patients with metastases to the spine and subsequent postoperative SSIs. To our knowledge, this study is the first to specifically evaluate the use of intrawound vancomycin powder in spine tumor surgery.
We identified 40 patients (46 procedures) undergoing spine tumor surgeries and receiving intrawound vancomycin powder. Five were excluded because of death less than 30 days postoperatively, and 35 patients (41 procedures) were enrolled. The majority of the tumors were metastatic with heterogenous diagnoses. Most of the tumors (21) were in the thoracic spine, followed by 12 in the lumbar spine and 8 in the cervical spine. Two culture-proven deep wound infections (S. aureus and E. cloacae) were noted in 41 procedures (4.9%). In the infection group, 1 patient had a metastatic prostate cancer and the other had an osteoblastoma. Infections responded to irrigation and debridement and antibiotic administration. There were no associations between radiation treatment and postsurgical infections (p = 0.19).
In one of the largest series (895 procedures) on SSIs following spine tumor surgery, an SSI rate of 10.7% (8.89% for primary nonbony spinal tumors, 9.5% for metastatic spinal tumors, 13.7% for primary bony spinal tumors) was reported. 3 Other series have reported infection rates ranging from 11.5 to 20%. 9 , 10 Preoperative radiation is a reported risk factor for SSIs with rates up to 32%. 8 Some innovations to prevent SSIs in spine tumor surgery include the use of iodine-supported instrumentation. 12 In a series of 125 patients undergoing total en bloc spondylectomy for spine tumors, there was an SSI rate of 12.5% when not using iodine-supported instrumentation versus 1.4% with use of iodine-supported instrumentation. 12 This technology is not yet globally available.
Use of vancomycin powder in spine surgery was first reported by Sweet et al. 13 They found a SSI rate of 0.2% in 911 patients undergoing instrumented thoracolumbar spinal fusion. Molinari et al reported a 1% rate of infections in 1,512 patients undergoing spine surgery with intrawound vancomycin powder. 14 They had 2 SSIs in 37 spine tumor cases (5.4%). In spine deformity surgery with an average of 10 fused levels, an infection rate of 2.7% rate was reported while using intrawound vancomycin powder. 15 Cost analysis study found a savings of $244,402 per 100 thoracolumbar adult deformity procedures. Spine traumas requiring spine surgery have historically high rates of infections. 2 A recent study of 110 patients with operatively managed spine trauma (54 controls; 56 with intrawound vancomycin powder) found 0 infections in the vancomycin group and a 13% rate of infection in the control group (p < 0.02). 1 , 5
One of the criticisms of intrawound vancomycin powder use is the possibility of increased infection with gram-negative organisms. Ghobrial et al evaluated 981 patients undergoing spine surgery with intrawound vancomycin powder application. They diagnosed 66 patients (6.7%) with SSIs, but only 51 patients (5.2%) had a positive wound culture. Although the most common organism was S. aureus, numerous gram-negative organisms were identified. The 15 patients (1.5%) who did not have positive wound cultures were diagnosed with sterile seromas. In the series, 36 patients with spine tumors received intrawound vancomycin powder, for an infection rate of 2.6%. 16
In our series, we found an infection rate of 4.9% in 41 spine tumor procedures with the use of intrawound vancomycin powder. Other series evaluating intrawound vancomycin powder in spine surgery with heterogenous diagnoses have reported infection rates of 2.6 to 5.4% in patients with spine tumor surgery. 14 , 16 However, these studies did not specifically evaluate the patients with spine tumors, and several important factors including tumor histology, location of tumor, and status of radiation therapy administration are missing. In our series, one of the two organisms identified was gram-negative and the second was gram-positive; we also had one case of sterile seroma. Our perioperative surgical complication rate was 26.8% and perioperative medical complication rate was 36.5%, which is similar to prior studies and underscores the complex nature of spine tumor surgery. 17 , 18
An SSI in a patient with a spine tumor is a devastating complication. Patients with spine tumors are often immunocompromised and have poor nutritional status; they have to undergo additional surgery for their SSI, extending their hospital stay and exposing them to increased health care costs. Postsurgical radiation treatment and chemotherapy also have to be delayed following surgical management of an SSI to allow for wound healing. We believe intrawound vancomycin powder is a simple yet effective means of decreasing SSI in patients undergoing spine tumor surgery. The use of iodine-supported instrumentation has the potential to diminish SSI in spine tumor surgery. 12 However, this instrumentation is not widely available, and we postulate that it is more expensive than using intrawound vancomycin powder.
Our study had several limitations. We did not randomize our patients into groups receiving intrawound vancomycin powder and a control group. We also did not use historical controls from our institution on the cases without intrawound vancomycin powder use but relied more on the reported rate of SSI in spine tumor surgery as reported in the literature. We believe the larger series on SSI in spine tumor surgery would be more representative rather than relying on our historical data. Our study was underpowered to detect a statistically significant difference in infection rates when our results are compared against the 10% rate reported by the largest series in the literature. 3 However, our study is the first to specifically evaluate SSI in spine tumor surgery with intrawound vancomycin powder, and we are planning a multi-institutional prospective study that will enroll more patients. We also did not report the preoperative nutritional status of the patients; prealbumin and albumin levels were not available for all patients because some were transferred to our hospital for urgent decompression and management.
In conclusion, in this first study specifically evaluating intrawound vancomycin powder for spine tumor surgery, we report an infection rate of 4.9%. Compared with previous studies of infection rates ranging from 10.7 to 32% (nonsacral spine tumors), our findings are noteworthy. We also found no correlations between radiation treatment and postsurgical infections (p = 0.19). Intrawound vancomycin powder can contribute to decreased infection rates following spine tumor surgery and is a simple means of preventing SSIs.
Disclosures
Richard Okafor, none
William Molinari, none
Robert Molinari, none
Addisu Mesfin, none