
Abstract
Study Design
Retrospective chart review and review of literature.
Objective
Few case reports of traumatic L5–S1 displacement have been presented in the literature. Here we present two cases of traumatic spondylolisthesis showing both anterior and posterior displacement, the treatment algorithm, and a review of the literature.
Methods
The authors conducted a retrospective review of representative patients and a literature review of traumatic spondylolisthesis at the L5–S1 junction. Two representative patients were identified with traumatic spondylolisthesis: one with an anterior dissociation, and the other with a posterior dissociation.
Results
Radiographic, computed tomography, and magnetic resonance imaging illustrated the bony and soft tissue injury found in each patient, as well as the final stabilization and outcomes. Operative stabilization was necessary, and both patients were treated with open reduction internal fixation. The patient with posterior dissociation had complete recovery without neurologic sequelae. The patient with anterior dissociation had persistent bilateral L5–S1 radiculopathy with intact rectal tone, due to neurologic compression.
Conclusions
Few cases of traumatic spondylopelvic dissociation that are isolated to the L5–S1 disk space are described in the literature. We examined both an anterior and a posterior dissociation and treated both with L5–S1 posterior spinal fusion. The patient with anterior dissociation had persistent L5–S1 root injury; however, the patient with posterior dissociation had no neurologic deficits. This is the opposite of what is expected based on anatomy. These cases offer insight into the management of anterior and posterior L5–S1 spondylopelvic dissociation.
Introduction
Traumatic spondylolisthesis of the lumbosacral junction is a rare injury with just over 100 cases found in the literature since it was first described over 70 years ago and fewer than 20 cases presented over the last 10 years. 1
Lumbosacral dissociation refers to the translocation of the L5 over the S1 vertebrae. A classification system for the different causes of spondylolisthesis has been developed and includes dysplastic, isthmic, degenerative, traumatic, and pathologic causes. 2 , 3 , 4 Most of these refer to changes in the vertebrae that occur over time due to genetic, mechanical, or pathologic processes that lead to an olisthesis of a superior vertebra over an inferior vertebra. Traumatic spondylolisthesis specifically refers to anterior or posterior displacement of the vertebrae following acute high-energy trauma to the pelvis or spine.
Of the L5–S1 diskal spondylolisthesis injuries reported in the literature, most involve dislocation in the anterior direction, with fewer than 10 cases reported in the posterior direction. 1 , 5 , 6 , 7
Two cases are presented with a dislocation at the L5–S1 junction. The first case is an anterior dislocation following a crush injury, and the second is posterior dislocation resulting from an automobile accident.
Case Reports
Case One
A 49-year-old man was sleeping on a loading dock while intoxicated and was crushed by a semitruck. He was taken to a local emergency department where he was evaluated and released to jail without an injury diagnosis. Although incarcerated, he began to experience worsening leg and back pain. He was then brought to our institution by ambulance from jail complaining of low back pain, left hip pain, and left thigh pain, with decreased perianal and penile sensation but no urinary incontinence. Rectal tone was absent, with a normal bulbocavernosus reflex, but he was otherwise neurologically intact. The initial radiographs showed bilateral L5–S1 facet joint fractures with grade 2 L5–S1 anterolisthesis, as well as L4 and L5 spinous and transverse process fractures (Fig. 1). Computed tomography (CT) confirmed the anterior dissociation of the lumbar spine from the sacrum (Fig. 2).
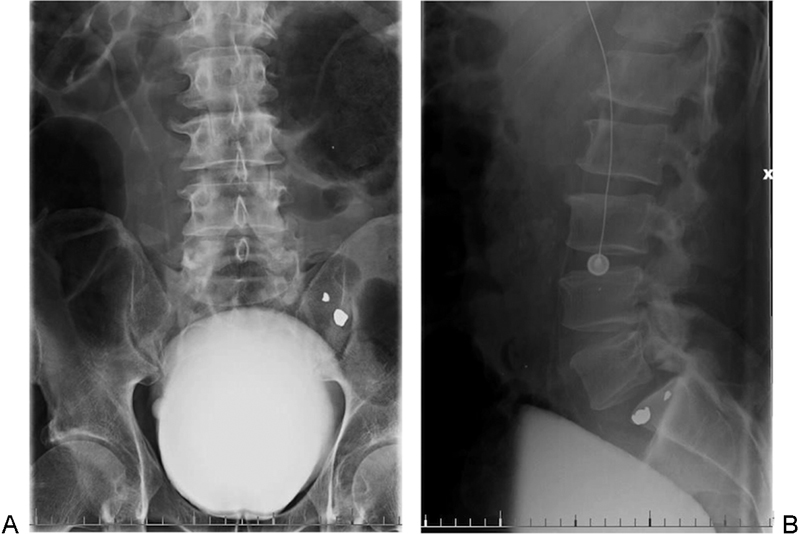
(A, B) Anteroposterior and lateral lumbar radiographs revealing bilateral L5–S1 facet joint fractures with a grade 2 L5–S1 anterolisthesis and L4–L5 spinous process and transverse process fractures. Bullet fragments from remote gunshot wound visible.
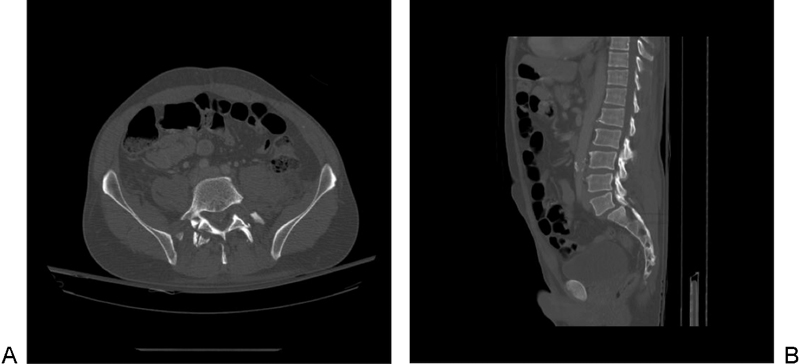
(A) Axial computed tomography image showing L5–S1 bilateral facet fractures and L5 spinous process fracture. (B) Sagittal computed tomography showing L5–S1 anterolisthesis.
The patient was urgently taken to the operating room where he was found to have a complete disruption of the right L5 superior facet through the pars interarticularis as well as a left-sided fracture dislocation at the L5–S1 level. He also had significant disruption of the interspinous ligament between L5 and S1 with fractures noted at the L5 lamina. A wide decompression with diskectomy was performed, ensuring that both the L5 and S1 nerve roots were free of compression. The anterior end plate and disk were sheared and displaced posteriorly and they impinged upon the roots and exiting cauda equina. L5 and S1 were instrumented with pedicle screws. The L5–S1 interspace was gently distracted, and a transforaminal lumbar interbody fusion was performed. Local autograft was packed within the disk space and tamped into place. Verification of its placement was made using fluoroscopy. Instrumentation was compressed posteriorly to restore natural lordosis (Fig. 3). A satisfactory reduction of the L5 vertebral body was obtained, and fusion was completed with decortication, local autograft, allograft, and demineralized bone matrix. Neuromonitoring was used throughout the procedure.

(A) Anteroposterior fluoroscopic intraoperative image showing bilateral screws and rods. (B) Lateral fluoroscopic intraoperative image showing rods, screws, and interbody fusion material.
Postoperatively, the patient's physical exam was unchanged. He had decreased penile, scrotal, and medial thigh sensation. Perianal sensation was intact, but rectal tone remained absent.
Case Two
A 23-year-old woman presented after a high-speed motor vehicle accident. She was a restrained rear seat passenger wearing both lap and shoulder belts, without loss of consciousness, and she was able to self-extricate from the vehicle. On arrival, she complained of back pain with tingling in the buttocks and posterior thighs, but she was initially discharged home. She was called back to the emergency room within 2 hours, when the final read of her CT scan demonstrated retrolisthesis of L5 on S1 with a small anterior fracture along the end plate of L5 and S1 and narrowing of the disk space (Fig. 4). She complained of worsening radicular symptoms and pain with ambulation. Subsequent magnetic resonance imaging demonstrated disruption of the posterior ligamentous complex and disk disruption with a collection of fluid in her facet joints (Fig. 5). A traumatic posterior L5–S1 spondylolisthesis was confirmed, and its instability likely responsible for the neurologic symptoms.
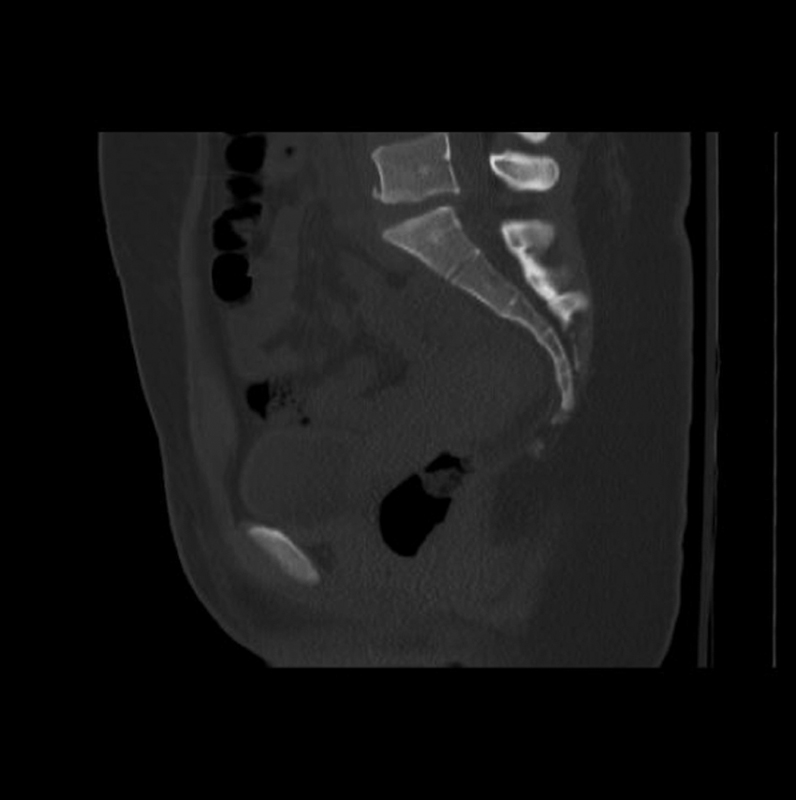
Sagittal computed tomography image showing L5–S1 retrolisthesis.
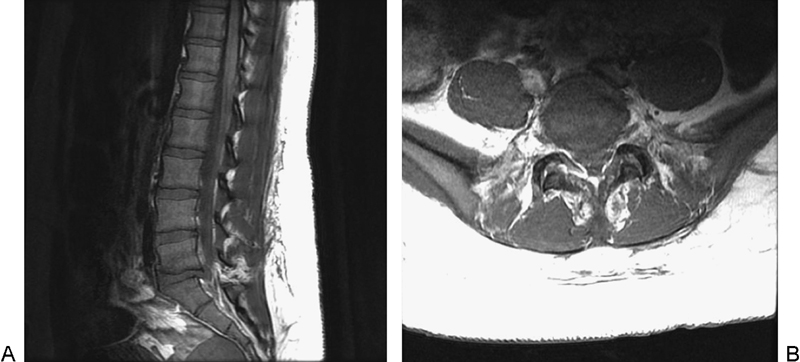
(A, B) Sagittal and axial magnetic axial imaging showing L5–S1 retrolisthesis, bilateral facet subluxation, interspinous ligament injury, and L5–S1 traumatic disk herniation with significant narrowing of the spinal canal.
The patient was brought to the operating room. Traumatic hemorrhage with edema in the soft tissues was noted. There was a complete transverse disruption of the posterior midline fascia in a typical tension failure injury of the posterior structures. The traumatic dissection was completed from the spinous processes to the level of the ligamentum flavum and dura. Instrumentation of the L5 and S1 pedicles occurred, and a diskectomy and a posterior lumbar interbody fusion were performed. The patient tolerated the procedure without complications (Fig. 6).

(A, B) Anteroposterior and lateral radiographs showing intact rods and screws fusing the L5–S1 levels.
Postoperatively the patient had a favorable outcome. Her radicular symptoms resolved and she was ambulating fully upon discharge without neurologic deficits.
Discussion
Traumatic spondylopelvic dissociation through the L5–S1 disk space is a rare entity, with roughly 100 cases reported since it was first described by Watson-Jones in 1940. 1 , 8 , 9 , 10 Translation may be anterior or posterior; however, posterior traumatic dislocations are rarer, with only 10 cases reported in the literature. 11 , 12 The lumbosacral articulation is itself a solid complex of bony and ligamentous restraints, which include the L5–S1 disk complex, the posterior facets, the iliolumbar ligamentum, and robust posterior musculature rendering it resistant to injury. 11
Watson-Jones suggested that the mechanism for anterior dislocation involves hyperextension. 10 , 13 However, most authors consider the mechanism of anterior spondylopelvic dissociation to be a combination of hyperflexion with compression, although the exact pathophysiology is still controversial. 8 , 9 , 14 , 15 , 16 Some authors argue that anterior dislocation results from lateral hyperflexion and rotation, and others report that this type of dissociation is purely a result of the direct trauma vectors. 17 , 18 , 19
Posterior dislocations are thought to result from posterior translation of the vertebrae on a fixed pelvis. 18 This mechanism would result in disruption of the posterior column and posterior ligamentous structures. Often the fractures are minimal, as the bony elements are moving away from one another. The final resting place of the spine and pelvis do not always represent the force vectors encountered during the actual accident. A posterior spondylolisthesis has been attributed to a combination of shear forces in the anterior direction and hyperextension due to high-energy trauma impact trauma to the posterior pelvis. 5 Case 2 involves a patient in a motor vehicle accident, therefore a combined injury is likely.
Early recognition of a spondylopelvic dissociation is often difficult, and initial diagnosis can be wrong. 14 , 15 , 16 As a result of the high-energy mechanism, 50 to 88% of cases have associated transverse process fractures. 9 The presence of transverse process fractures should increase the suspicion for spondylopelvic dissociation. 8 , 9 , 15 , 16 On an anteroposterior radiograph, helpful signs include obliquity of L5 on the sacrum and transverse process fractures. 11 On lateral radiographs, increased interspinous distance, spondylolisthesis, L5 on S1 kyphosis, and a narrow anterior disk space height are suggestive of dissociation. CT may reveal the empty facet sign and empty or perched facets on axial cuts. 11 , 15 Certainly a high index of suspicion should be made for any patient involved in a significant injury with back pain with or without neurologic symptoms. In these cases, a screening CT scan is mandatory.
Lumbosacral dissociation is a three-column injury and is considered unstable. 11 , 20 Neurologic deficits are present in approximately one third of cases with bilateral L5–S1 injury, and these patients should be treated with surgical urgency. 13 Pure cauda equina syndrome is rarely found. 9 For patients without neurologic deficits, magnetic resonance imaging should be completed to assess the severity of the lesion and to decide whether or not the canal needs to be explored. 6 , 13 Although CT scans independently give no direct information on the integrity of the disks and ligaments, widened facet joints or avulsion fractures may suggest ligamentous disruption. 9
Open reduction and internal fixation using pedicle screws is considered the standard of treatment for this injury. 9 , 16 It is safest to perform the reduction intraoperatively where the canal can be explored to ensure there are no bone or disk fragments. 13 Because this is a three-column injury, anterior support may be necessary to ensure stability. For more complex or extensive L5–S1 injuries, additional fixation, including pelvic or iliosacral fixation, may be necessary. 16 , 21 , 22 Some authors had advocated a trial of nonoperative management, but most patients in the literature who have been treated conservatively eventually required surgery. 3 , 11 , 23 , 24 Final prognosis is typically determined by the preoperative neurologic status. 18
Only three cases of posterior traumatic lumbosacral dissociations have been reported to date. 12 Posterior dislocations are theoretically more commonly associated with neurologic injury as the bony ring is often left intact, more readily causing impingement. 4 , 6 They are also more likely to occur in the setting of more severe traumatic disruption and therefore lead to more neurologic compression. Anterior dislocations, which often have bony fractures, can self-decompress the spine and allow the room necessary for the neural elements. In our case examples, the anterior translation resulted in a disk/end plate herniation, which is likely responsible for the continued neurologic injury in the patient with the L5–S1 anterior spondylolisthesis. The posterior spondylolisthesis in case two initially presented with worsening neurologic symptoms but did not sustain any long-term neurologic injury, likely due to rapid reduction and fixation.
Traumatic dissociation through the L5–S1 disk level is a rare injury that has two major injury patterns: anterior spondylolisthesis or posterior spondylolisthesis. Both represent a three-column injury that dissociates the pelvis from the spine and requires surgical stabilization. Because it is a rare injury, it can easily be missed without appropriate radiographic examination and a high index of suspicion.
Disclosures
Michael Robbins, none
Zachary Mallon, none
Rolando Roberto, none
Ravi Patel, none
Munish Gupta, Board membership: FOSA; Consultant: Depuy Synthes, Medtronic; Royalties: Depuy Synthes; Stock options: Proctor Gamble, Johnson and Johnson
Eric Klineberg, none
EBSJ wishes to thank the authors and Dr. France for their contributions by bringing to our readers’ attention this important albeit rare severe injury entity. In this day and age it seems near impossible that such major injuries are still missed, yet we have two such cases here. The insightful discussion of Dr. France points out two of the major potential problems faced by many emergency departments around the world:
Disruption of the usual trauma algorithm by rushing patients to urgent care outside of the customary sequence
Time pressures to “process” patients toward a final disposition
Although most trauma centers around the globe have reasonably ready access to CT scanners—which allows for easy diagnosis of lumbopelvic trauma—the real challenge lies in getting this relatively simple diagnostic test completed. Thoughts on how to counter these two problems have been formulated but have not been formally implemented as protocol formats or been studied in a peer-reviewed setting.
The intuitive answer to handling patients who were not beneficiaries of a completed trauma workup due to life- and/or limb-saving procedures are best managed by tagging them as “trauma incomplete” and maintaining them in such a status until a formal secondary trauma survey has been completed. Electronic medical records can be helpful to keep reminding the providers of the need to finalize such a secondary trauma survey.
The time pressure issue is probably best addressed by implementing CT scans instead of plain radiography in trauma assessments. Of course, the area of interest has to be part of the screening protocol, and a quality interpretation should involve not just a radiologist but a knowledgeable clinician involved in the care of the patient.
Finally, a quality improvement system that constructively reviews missed cases and looks to implement changes would be a desirable institutional enhancement.