
Abstract
Study Design
Case report.
Objective
We report a case of spontaneous atlantoaxial rotatory fixation (AARF) presenting 9 months after onset in an 11-year-old boy.
Methods
This is a retrospective case report of spontaneous ankylosis of occiput to C2 following traction, manipulative reduction, and halo immobilization for refractory atlantoaxial rotatory fixation.
Results
The patient underwent traction followed by close manual reduction and placement of halo immobilization after 6 months of severe spontaneous-onset AARF that had been refractory to chiropractic manipulation and physical therapy. Imaging demonstrated dislocation of the left C1–C2 facet joint and remodeling changes of the C2 superior facet prior to reduction, followed by near complete reduction of the dislocation after manipulation and halo placement. Symptoms and clinical appearance were satisfactorily improved and the halo vest was removed after 3 months. At late follow-up, computed tomography demonstrated complete bony ankylosis of the occiput to C2. The patient was found to be HLA B27-positive, but he had no family history of ankylosing spondyloarthropathy or other joint symptoms. The underlying reasons for spontaneous fusion of the occiput to C2 could include the traction, HLA-B27-related spondyloarthropathy, or arthropathic changes caused by traction, reduction, the inciting insult, or immobilization.
Conclusion
When discussing treatment of childhood refractory AARF by traction, closed manipulation, and halo immobilization, the possibility of developing “spontaneous” ankylosis needs to be considered.
Introduction
Atlantoaxial rotatory fixation (AARF) is an uncommon condition that usually occurs in children after an inflammatory upper respiratory tract infection or pharyngitis, but it can also be spontaneous or follow minor trauma or surgery on the oropharynx. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 Fielding and Hawkins have classified AARF into four types on the basis of the rotational displacement and competency of the transverse ligament. 1 Most cases are thought to be the result of nonresolving acute atlantoaxial rotational subluxation or “acute torticollis.” Treatment usually consists of traction until reduction occurs, followed by immobilization in Minerva brace or halo vest. 1 , 9 , 10 , 11 , 12 , 13 If reduction does not occur, most authors recommend surgical fusion with attempt at reduction to the most normal position possible, followed by traction, immobilization, or internal fixation. 9 , 10 , 14 , 15 , 16 Some authors even report more aggressive surgical methods to achieve reduction and fusion. 17 , 18 More recently, Scapinelli, Tauchi et al, and others have reported closed reduction under anesthesia and halo immobilization with good results in most cases, with surgical fusion performed if a C2 articular process deformity remains following treatment or if repeat rotational displacement occurs. 11 , 19 , 20 , 21
We report a case of spontaneous AARF in an 11-year-old boy, presenting 9 months after onset. The patient underwent traction, closed reduction, and halo immobilization. At follow-up, this child had spontaneous and impressive bony ankylosis of the occiput to C2. He was found to be HLA B27-positive but had no other clinical manifestations of ankylosing spondylitis.
Case Report
An 11-year-old boy presented to our clinic with torticollis that started 9 months prior. The onset was spontaneous with the patient awaking one morning with a severe headache and a head tilt. He was initially evaluated by his primary care physician who recommended careful observation for 2 weeks, but due to its persistence and pain, the child was evaluated at a local emergency department where a computed tomography (CT) scan of his cervical spine was obtained; he was discharged with pain medications and a prescription for physical therapy. His neck pain and headaches did not abate with the medication or therapy. The parents sought the help of a chiropractor who performed a manual adjustment alleviating his pain and headache instantly, but the head tilt still persisted. Subsequent manipulations by the chiropractor totaled 28. He revisited his primary care physician for his head tilt, without neck pain or neurologic symptoms. The patient was referred to a neurologist and an orthopedic surgeon. The neurologist prescribed Sinemet (Merck & Co., Inc., Whitehouse Station, New Jersey, United States) and valium, but neither provided any form of relief of his head tilt. After evaluation by the orthopedic surgeon, further imaging including magnetic resonance imaging (MRI), CT scan, and magnetic resonance angiography revealed Fielding and Hawkins type II rotatory fixation of C1 on C2 with adequate space for the cord, no myelopathic changes, and a normal vertebral artery flow. He was referred to us for further treatment of his condition.
At the time of presentation to us, he had no neck pain or neurologic symptoms. His past medical history was pertinent for Asperger syndrome, but otherwise negative, with no history of oropharyngeal surgery. Family history was negative for inflammatory arthritis or ankylosing spondylitis.
On exam, he had obvious torticollis with his chin pointed toward his right. A photograph of the patient at time of presentation can be seen in Fig. 1. His rotation was markedly limited in turning to the left. His neurologic exam was normal except C5 sensory disturbance and 3/5 left deltoid weakness noted. He had no spasticity or ataxia. His reflexes were brisk bilaterally in both upper and lower extremities, but Hoffmann, clonus, and Babinski reflexes were absent. Cranial nerves were intact.

Patient at presentation after affected by atlantoaxial rotatory fixation.
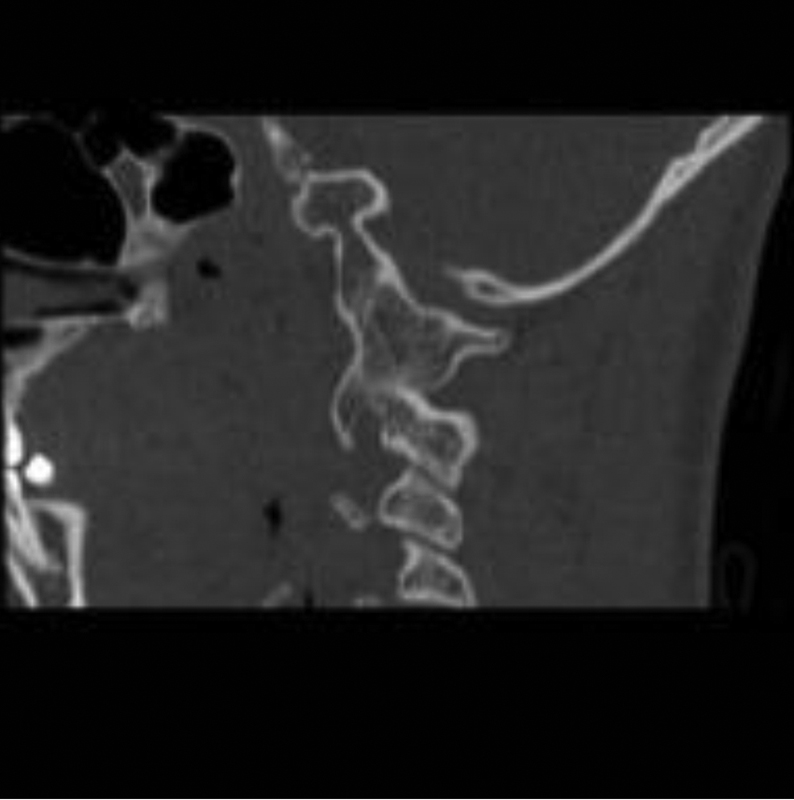
His MRI showed no spinal cord compression, signal change, or C5 nerve root compression on the left. Magnetic resonance angiography showed intact vertebral artery flow bilaterally. CT scans revealed anterior dislocation of left lateral mass of C1 on C2 (Fig. 2). The transverse ligament appeared intact. Remodeling of his left C2 articular facet with early signs of possibly bridging osteophytes was noted. The inferior facet of C1 on the left was at the level of the C2–C3 disk space (Figs. 2,3,4).
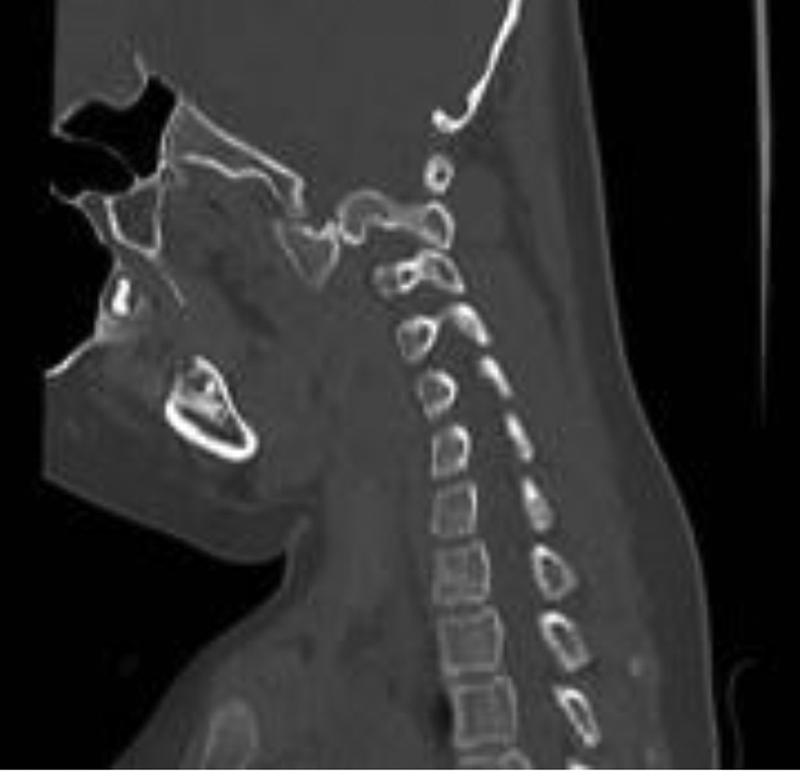
Sagittal reconstruction computed tomography at presentation, left C1–C2 facet dislocation.
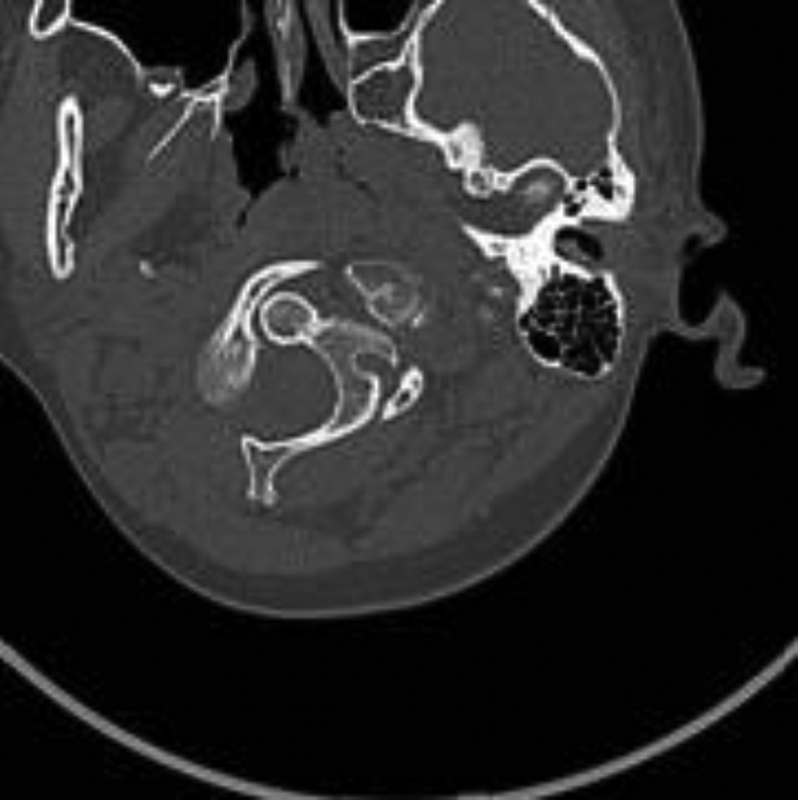
Axial computed tomography at presentation, left C1–C2 facet dislocation.

Coronal reconstruction computed tomography at presentation, left C1–C2 facet dislocation.
Treatment options were discussed with family and halo traction was initiated. Traction was increased over 1 week from 5 to 25 pounds, during which the inferior displacement of the left C1 lateral mass improved but the rotational deformity did not reduce.
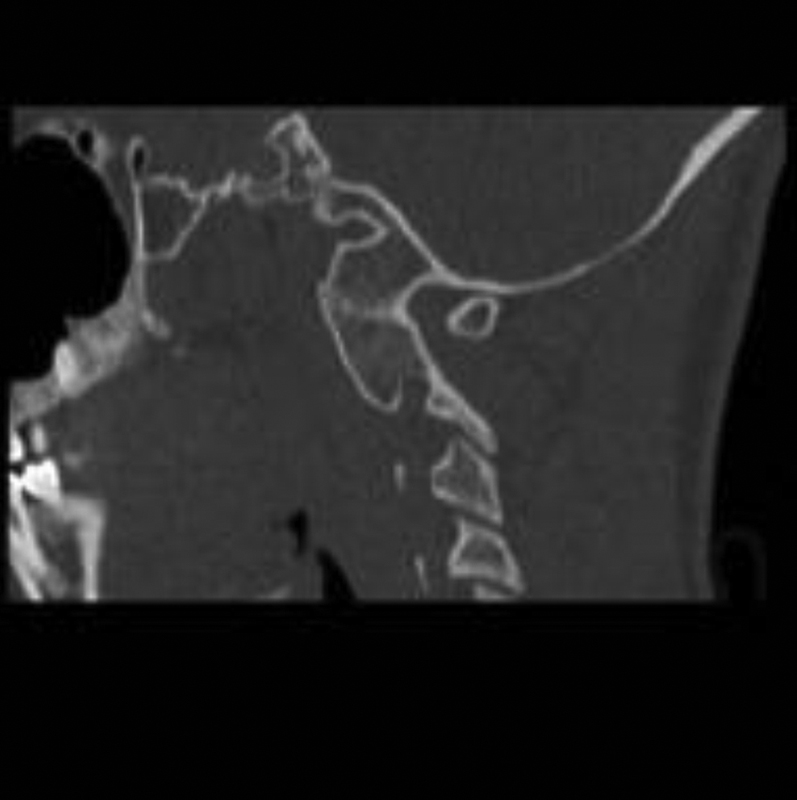
Options of surgical reduction and fusion or manipulative reduction and halo vest for 3 months were discussed and the family chose the latter. Manipulative reduction was performed in the CT suite under mild sedation while in traction. The initial result of the reduction can be seen in Figs. 5 and 6. He was then placed in a halo vest in a reduced position with plans for 3 months of halo immobilization.

Postreduction sagittal reconstruction computed tomography in halo vest.

Postreduction coronal reconstruction computed tomography in halo vest.
Three months following reduction, his halo vest was removed. His neurologic exam at that time showed that his deltoid weakness had improved to functional insignificance but had not completely resolved. Some rotational malalignment was still present, but the left C1–C2 facet was not dislocated. Increasing signs of spontaneous ankylosis of the left C1–C2 facet were present. The family declined surgical treatment as they felt his clinical improvement was acceptable. Mild residual torticollis was present. Six months after reduction, a CT scan was obtained and can be seen in Figs. 7, 8, and 9. The patient's final picture is depicted in Fig. 10.
Six months’ follow-up postreduction sagittal reconstruction computed tomography through right C1–C2 facet. Note solid bony ankylosis of occiput to C2. Lower cervical facets appear normal.
Six months’ follow-up postreduction sagittal reconstruction computed tomography through left C1–C2 facet. Note solid bony ankylosis of occiput to C2.

Six months’ follow-up computed tomography three-dimensional reconstruction showing occiput-to-C2 fusion.

Patient at 6 months’ follow-up.
Discussion
Traditionally, AARF that does not reduce in traction has been treated by posterior C1–C2 fusion with reduction of the deformity at the time of surgery, if possible. 1 Closed reduction of AARF and use of halo traction has been advocated as a method of treatment that avoids surgical fusion in most cases and thus should preserve C1–C2 rotational movement, which accounts for nearly 50% of cervical spine rotation. 11 , 19
Spontaneous fusion of the cervical spine as a result of halo-pelvic immobilization was reported by Dove et al in 5 of 83 patients. 22 However, all spontaneous fusions occurred from C2 and below, and none occurred in patients immobilized for 3 months or less. The majority of patients in that series were immobilized for 6 months or longer. Spontaneous fusion at C1–C2 following traumatic fracture dislocation is also reported. 23 We were unable to find other reports in the English language literature of spontaneous occiput-C2 fusion following AARF.
“Spontaneous” fusion of the cervical spine often occurs in ankylosing spondyloarthropathies. 24 Hamilton and MacRae reported on a 27-year-old patient with spontaneous AARF with no evidence of infectious or inflammatory process who developed clinical and laboratory evidence of ankylosing spondylitis 3 years after the onset of her symptoms. 25 This patient underwent a surgical C1–C2 fusion, so whether spontaneous ankylosis may have occurred is unknown. Hamilton and MacRae hypothesized that the inflammatory process can cause laxity and incompetence of the transverse ligament resulting in AARF. 25 Lui and Inman also described atlantoaxial subluxation as the initial manifestation of spondyloarthritis, 26 and Mitra et al, as a manifestation in juvenile rheumatoid arthritis. 27
HLA-B27 functions as an antigen-presenting molecule and has been associated with spondyloarthropathies but is present in patients without ankylosing spondylitis. 24 Our patient was later found to be HLA-B27-positive but has not manifested any other evidence of ankylosing spondyloarthropathy.
The natural history of untreated AARF is unknown, but in a study by Fielding and Hawkins, two patients who refused treatment were followed for 8 years; one underwent spontaneous correction and the other's deformity remained unchanged. 1 Conservative treatment, such as halter traction, has been shown to be effective when the diagnosis is made early. 6 It has been speculated the duration of symptoms prior to diagnosis and treatment can affect the outcome. 10
Closed reduction and halo immobilization treatment of refractory AARF was reported by Scapinelli and Tauchi et al, with the advantage of avoiding open surgical treatment and fusion in most cases. 19 Tauchi et al noted that the deformity of the C2 lateral mass that occurs in some patients will remodel in most cases after reduction and immobilization. 11 The length of time elapsed from onset to reduction in our patient(∼270 days) was longer than that reported in their series, which ranged from 31 to 169 days. The spontaneous fusion of C1–C2 would thus not be entirely unexpected, despite lack of case reports of this. In fact, the pretreatment CT suggested that spontaneous ankylosis at C1–C2 may have occurred without treatment, though in a severely displaced position. We have seen other cases in which posttreatment CT suggests that spontaneous C1–C2 fusion may occur following closed reduction and halo treatment of refractory AARF. It remains unusual, however, that fusion occurred from occiput to C2 in our patient.
It is possible that surgical treatment could have resulted in a fusion of C1–C2 only and spared some loss of motion for this child. Furthermore, it is possible, though not certain, that open surgical treatment may have achieved a more anatomical reduction, with less residual rotational deformity. This case shows that closed reduction of refractory AARF may result in spontaneous fusion. Whether this result was determined by some aspect of our treatment or was the result of the underlying conditions is not clear. Factors that may have contributed to the C1–C2 fusion include the length of time from onset, the evidence of evolving ankylosis already present at C1–C2, the trauma occurring to the C1–C2 joint during reduction, and possible preexisting spondyloarthropathy. The underlying reasons for spontaneous fusion of occiput to C2 could include aspects of the underlying condition (inflammatory arthropathy and longstanding, limited neck mobility), physical therapy or chiropractic treatments, traction, manipulative reduction, or immobilization. Knowing that this patient was HLA-B27-positive prior to treatment, however, would not likely have changed our management.
When discussing treatment of childhood refractory AARF by traction, closed manipulation, and halo immobilization, the possibility of developing “spontaneous” ankylosis needs to be considered.
Disclosures
Walter F. Krengel III, none
Paul H. Kim, none
Brett Wiater, none
Within the arena of spine trauma, there is arguably no topic that fulfills clinicians with more unease than pediatric patients. Moreover, cervical deformity is an area that is not well taught and is largely empirical in terms of literature foundation. A combination of both subject areas—pediatric upper cervical spine trauma and acquired deformity—can challenge all but the most experienced clinicians and underscores the value of a larger virtual spine surgeon community where care challenges and experiences can be shared in a real-time fashion.
Of course, attempts at closed management of upper cervical disorders are always laudable in light of the potential of significant loss of motion. The propensity of stripped periosteum to form bone in the very young is well known and led to a probably desirable final ankylosis in this particular patent. Having improved imaging modalities as described by Dr. Avellino may advance our ability to identify such injuries in the future and should help in counseling patients and their families more specifically about the risk of unintended bony ankylosis. MRI of young patients may hold its own challenges, as quality closed-tube imaging usually requires a general anesthesia for most patients in this age category.
Finally, a politically challenging commentary pertains to the use of spinal manipulation in young patients. It is very hard to understand how especially repeated manipulations of a minor's neck can be justified under any circumstances. In principle, allied health care interventions should be subject to the same evidence-based burdens that all other branches of health care are subjected to.