
Abstract
Study Design
Retrospective comparative study.
Objective
A narrow spinal canal is an important risk factor for predicting a spinal cord injury (SCI); however, the radiologic parameters have not been fully established. The authors conducted a comparative study to forecast SCI risk by determining a predictive spinal canal diameter (SCD) cutoff value from magnetic resonance image (MRI) in the Korean population.
Methods
On T2-weighted MRI of the cervical spine, the SCD at the pedicle (SCDpedicle) and the intervertebral disk level (SCDdisk) were measured in patients with SCI without spinal instability and in healthy subjects. Additionally, the vertebral body diameter (Dvertebral body) and intervertebral disk diameter (Dintervertebral disk) were measured, and the two ratios (SCDpedicle to Dvertebral body and SCDdisk to Dintervertebral disk) were calculated. In the SCI group, the extent of high signal intensity on the T2-weighted midsagittal MRI was determined.
Results
The data obtained from 20 patients in the SCI group (18 men, mean age 61.35 years) and 65 individuals in the control group (47 men, mean age 57.05 years) was compared. All the parameters including the SCD and the calculated ratios were significantly smaller in the SCI group than in the control group. Among them, the area under the receiver operating curve (AUC) value for the SCDdisk-to-Dintervertebral disk ratio at C2–C3, with a cutoff ratio value of 0.59, provided the greatest positive predictive value. A low SCDdisk-to-Dintervertebral disk ratio at C4–C5 and the presence of >40 mm of high signal intensity on the MRI were related with the presence of complete SCI.
Conclusion
Because the C2–C3 level is relatively wide compared with the subaxial cervical spine, a small ratio at C2–C3 provided the greatest positive predictive value in SCI. Complete SCI is associated with a small SCDdisk-to-Dintervertebral disk ratio at C4–C5 and with extensive high signal intensity on MRI.
Introduction
Traumatic cervical spinal cord injury (SCI) is frequently a result of spinal fracture and dislocation or an outcome of discoligamentous injury. 1 , 2 , 3 Neurologic deficits after trauma to the cervical spine may develop in the absence of bony damage, and such instances often are described as SCI without radiographic abnormality or as SCI without radiologic evidence of trauma. 3 , 4 , 5 , 6 Most patients with SCI are elderly, including those without radiographic abnormality and those without radiologic evidence of trauma. Moreover, such patients have a congenitally narrow spinal canal or exhibit degenerative changes such as spinal stenosis, osteophytes, hypertrophy of the ligamentum flavum, hypertrophy of the posterior longitudinal ligament (PLL), or ossification of the PLL (OPLL). 4 , 5 , 7 Hyperextension injury to a narrow spinal canal may lead to intramedullary injury in the absence of a spinal fracture or dislocation and can frequently result in an incomplete SCI. 3 , 6 , 8 , 9 , 10 , 11 , 12
Although the studies into cervical spine stenosis and its association with cervical trauma have been reported, the benefits of prophylactic surgery for cervical spinal stenosis have not been established. 1 , 2 , 3 , 13
In this study, we investigated the cervical spinal canal diameters in subjects exhibiting traumatic cervical SCI without spinal fracture by examining T2-weighted midsagittal magnetic resonance images (MRIs). Based on our analysis, a cutoff value associated with neurologic deficits from acute trauma to the cervical spine was determined. In addition, the relationship between the SCI severity and the radiologic parameters was examined.
Materials and Methods
Patient Populations
Between 2004 and 2011, 134 patients underwent operations for traumatic cervical SCI in our department. Patients with a facet fracture or dislocation; those with vertebral body, spinous process, or lamina fractures; and those with intervertebral disk rupture as demonstrated on computed tomography (CT) and/or MRI were excluded from our study. Among those, 20 patients without spinal instability were included in our SCI group. Patient neurologic status was assessed by the American Spinal Injury Association (ASIA) impairment scale, and the injury mechanism was classified as either low or high energy.14,15 Low-energy injury included a fall onto the ground level or a fall from a low height (<1 m) and high-energy injury was a fall from more than 1 m or a motor vehicle accident. Age- and sex-matched subjects between 40 and 80 years old without prior surgery to the cervical spine and who underwent cervical MRI in our health screening center between 2010 and 2011 were included in our control group.
All included patients provided written and informed consent, and the study was conducted with institutional review board permission.
Radiologic Evaluation of T2-Weighted Magnetic Resonance Images
For each member of the SCI group, an initial preoperative MRI was obtained within 48 hours following trauma. On T2-weighted midsagittal MRI, the spinal canal diameters (SCDs) at the C3–C7 pedicle levels (SCDpedicle) and the C2–C3 to C6–C7 intervertebral disk levels (SCDdisk) were measured in both groups (Fig. 1). Additionally, for both groups, the anteroposterior vertebral body diameter (Dvertebral body) and the intervertebral disk diameter (Dintervertebral disk) were measured on MRI at each pedicle and intervertebral disk level. The SCDpedicle-to-Dvertebral body and SCDdisk-to-Dintervertebral disk ratios were calculated at each pedicle and intervertebral disk level. In addition, the extent of the high signal intensity on T2-weighted midsagittal MRI was measured in the SCI group. Measurements were taken by an independent observer using picture archiving and communication system software (M-view, version 5483; Infinite Healthcare, Seoul, Korea) and were recorded to the nearest 0.01 mm.
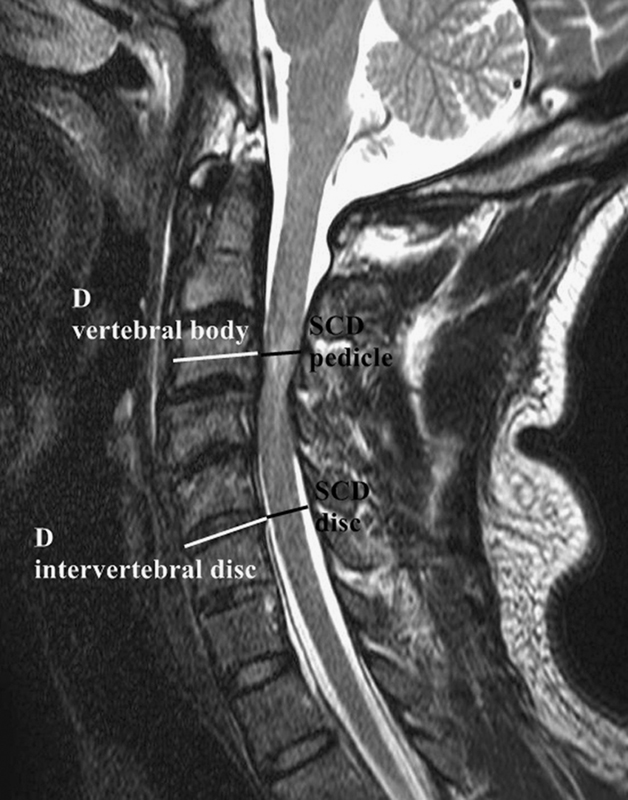
Radiologic evaluation on T2-weighted midsagittal magnetic resonance imaging. Spinal canal diameter (SCD) was measured at each pedicle (SCDpedicle) and intervertebral disk level (SCDdisk). After measuring the anteroposterior diameter of the vertebral body (Dvertebral body) and the diameter of the intervertebral disk (Dintervertebral disk), the SCDpedicle-to-Dvertebral body and SCDdisk-to-Dintervertebral disk ratios were calculated.
Statistical Analysis
Descriptive statistics are presented as means and standard deviations. The chi-square test was used to compare the gender distribution between the two groups. The t test and Wilcoxon rank sum test were used to compare age composition and the measured continuous parameters between the groups. Receiver operating curves were calculated to evaluate the accuracy of parameters used to predict SCI. The highest area under the receiver operating curves (AUC) value was used to enable derivation of a cutoff value. The AUC value with the lowest [(1 − sensitivity)2 + (1 − specificity)2] value was selected as the cutoff value. The positive predictive value (PPV), represented by the proportion of patients with positive test results that were correctly diagnosed (i.e., true-positives divided by all positives), was determined. The negative predictive value, represented by the proportion of patients with negative test results that were correctly diagnosed (i.e., true-negatives divided by all negatives), was also determined. The positive likelihood ratio was calculated by dividing the sensitivity by the false-positive rate. The negative likelihood ratio was calculated by dividing the false-negative rate by the specificity. A leave-one-out cross-validation method was used during re-evaluation of the obtained cutoff value as an indicator of diagnostic ability. A p value < 0.05 was considered significant for all statistical analysis results.
Results
Patient Demographics
Of the 134 patients with cervical SCI considered for inclusion in this study, 20 patients (14.9%) had SCI without spinal instability and were included in our SCI study group. The study group included 18 male and 2 female patients, and the group's mean age was 61.35 ± 12.20 years (Table 1). The injury mechanism was high energy in 9 patients (45%) and low energy in 11 patients (55%). Injury sources were motor vehicle accident (4 patients), fall of >1 m (5 patients), fall of <1 m (5 patients), and fall onto the ground level (6 patients). The initial neurologic status was complete injury in 3 patients and incomplete injury in 17 patients. The initial ASIA scores were A in 3, B in 7, C in 6, and D in 4 patients. The initial neurologic level was C3 in 4, C4 in 9, C5 in 4, and C6 in 3 patients. The underlying cervical spinal disease was spinal stenosis in 13, OPLL in 4, and PLL hypertrophy in 3 patients. Analysis of the age, gender, injury mechanism, neurologic level, and preoperative underlying disease data stratified according to initial neurologic status did not reveal a significant difference between the complete injury and incomplete injury members of the SCI group (all p > 0.05).
Patient demographics in SCI group
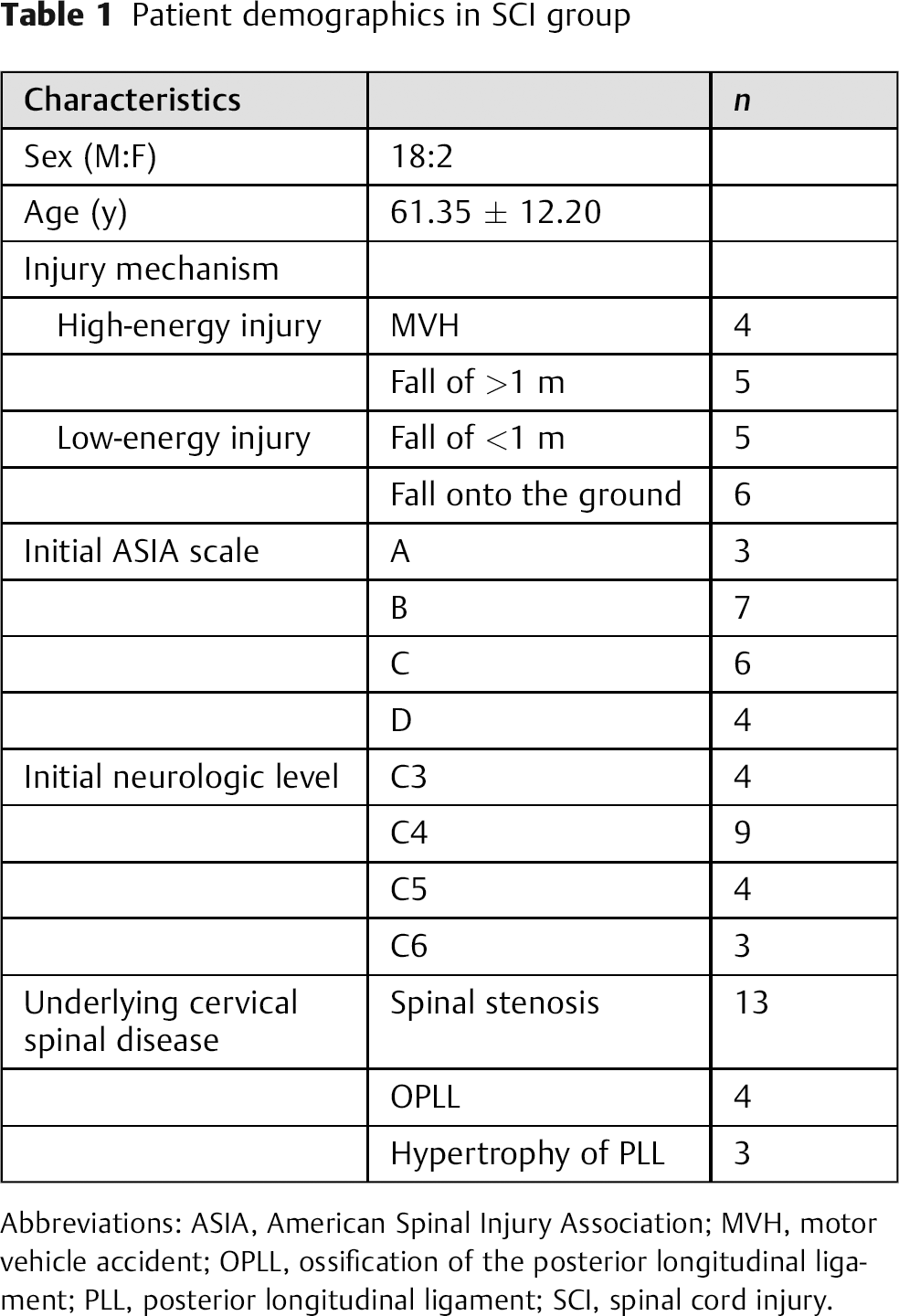
Abbreviations: ASIA, American Spinal Injury Association; MVH, motor vehicle accident; OPLL, ossification of the posterior longitudinal ligament; PLL, posterior longitudinal ligament; SCI, spinal cord injury.
There were 65 individuals included in the control group: 47 male and 18 female subjects with a mean age of 57.05 ± 7.41 years. There were no statistically significant differences in the patient demographic characteristics between the SCI and control groups (gender, p = 0.137; age, p = 0.156).
Radiologic Parameters on Magnetic Resonance Images for Predicting Spinal Cord Injury Risk
The measured and calculated radiologic parameters used to assess spinal canal narrowing are demonstrated in Fig. 2. All parameters, including spinal canal diameters at each pedicle and intervertebral disk level, and the calculated ratios at each level, were significantly lower in the SCI group than in the control group.
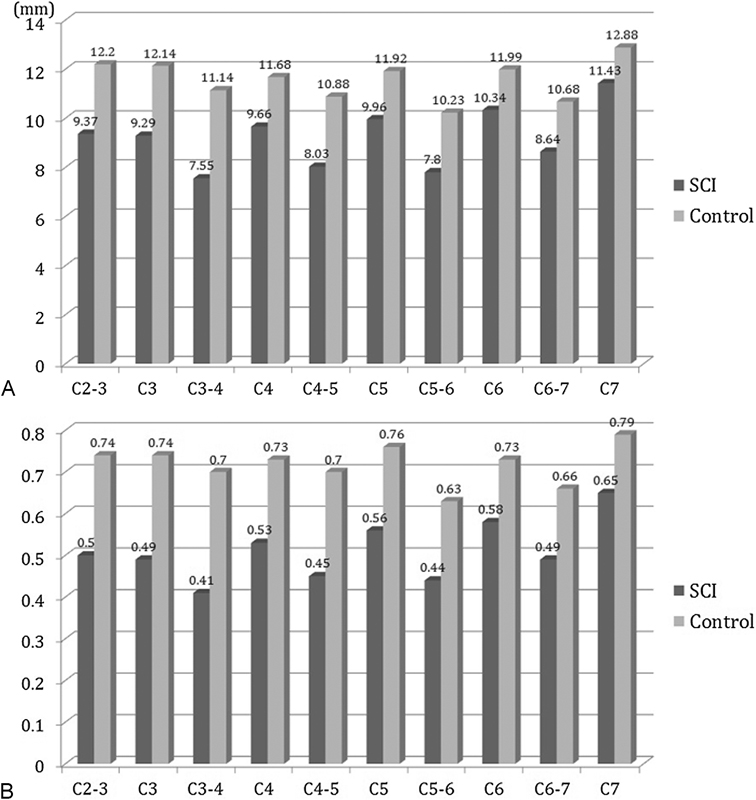
Radiologic parameters in the spinal cord injury (SCI) and control groups. (A) Spinal canal diameters at pedicle levels C3, C4, C5, and C6 and diameters at intervertebral disk levels C2–C3, C3–C4, C4–C5, C5–C6, and C6–C7 were significantly smaller in the SCI group than in the control group (p < 0.05). (B) Calculated ratio of spinal canal diameter at each pedicle to anteroposterior diameter of the vertebral body and ratio of spinal canal diameter at the intervertebral disk level to diameter of the intervertebral disk were significantly lower in the SCI group than in the control group (p < 0.05).
The AUC value for predicting SCI was highest for the SCDdisk-to-Dintervertebral disk ratio at the C2–C3 intervertebral disk level. The associated cutoff value was 0.59 (Table 2). When the SCI group members were stratified into subgroups above and below that 0.59 cutoff value, the PPV was 81.82% with an associated accuracy of 97.23% (Table 3). Although the 0.59 cutoff value based on the SCDdisk-to-Dintervertebral disk ratio at C2–C3 maximized both sensitivity and specificity, we applied the leave-one-out cross-validation method to evaluate the cutoff value's diagnostic ability. As a result, the AUC was 0.968 (95% confidence interval 0.934 to 1.000) with PPV and accuracy values of 80.95 and 96.77%, respectively.
Area under the receiver operating curve
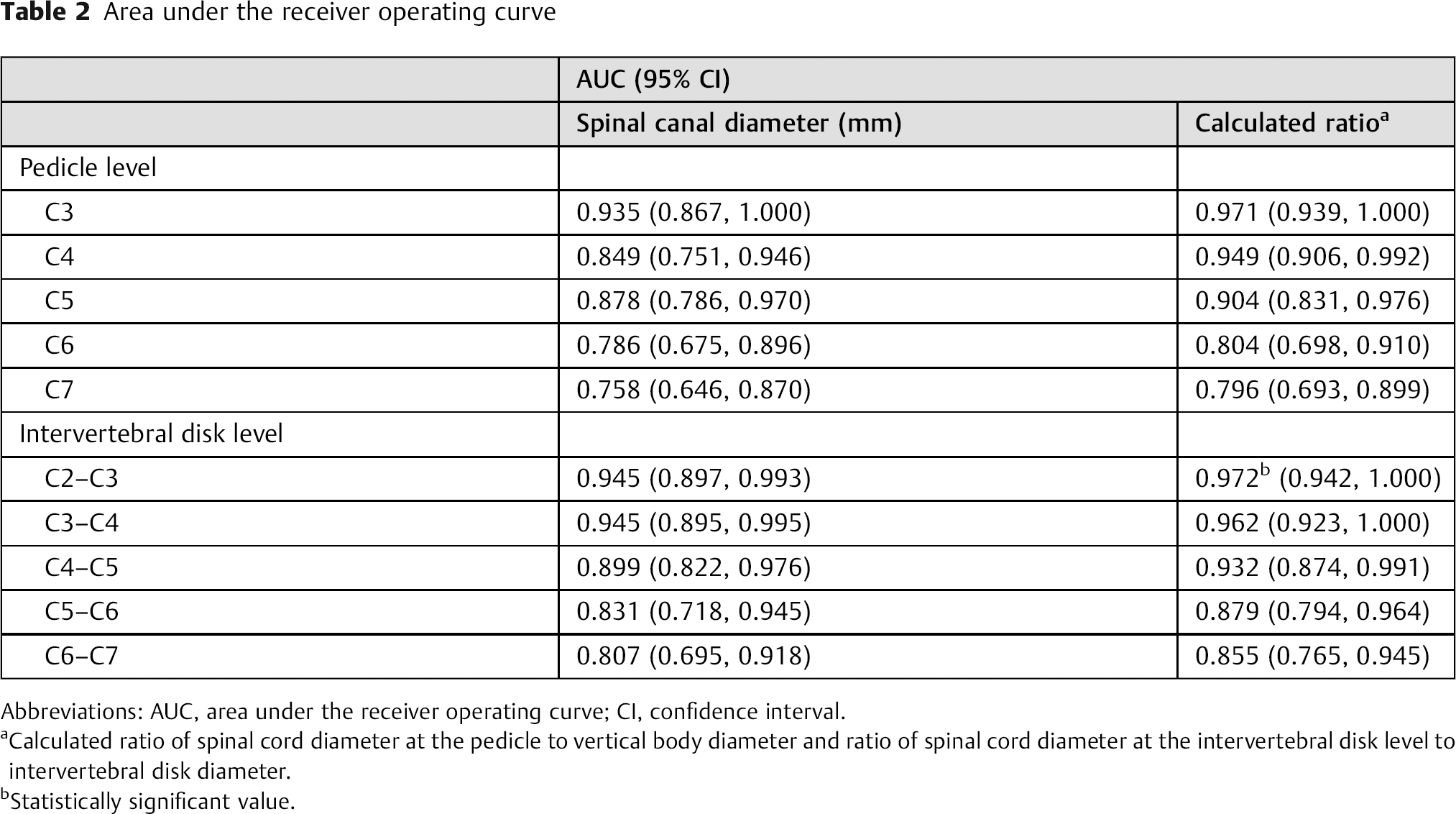
Abbreviations: AUC, area under the receiver operating curve; CI, confidence interval.
Calculated ratio of spinal cord diameter at the pedicle to vertical body diameter and ratio of spinal cord diameter at the intervertebral disk level to intervertebral disk diameter.
Statistically significant value.
Predicting SCI risk from spinal canal diameter ratio (SCDdisk to Dintervertebral disk) at the C2–C3 intervertebral disk
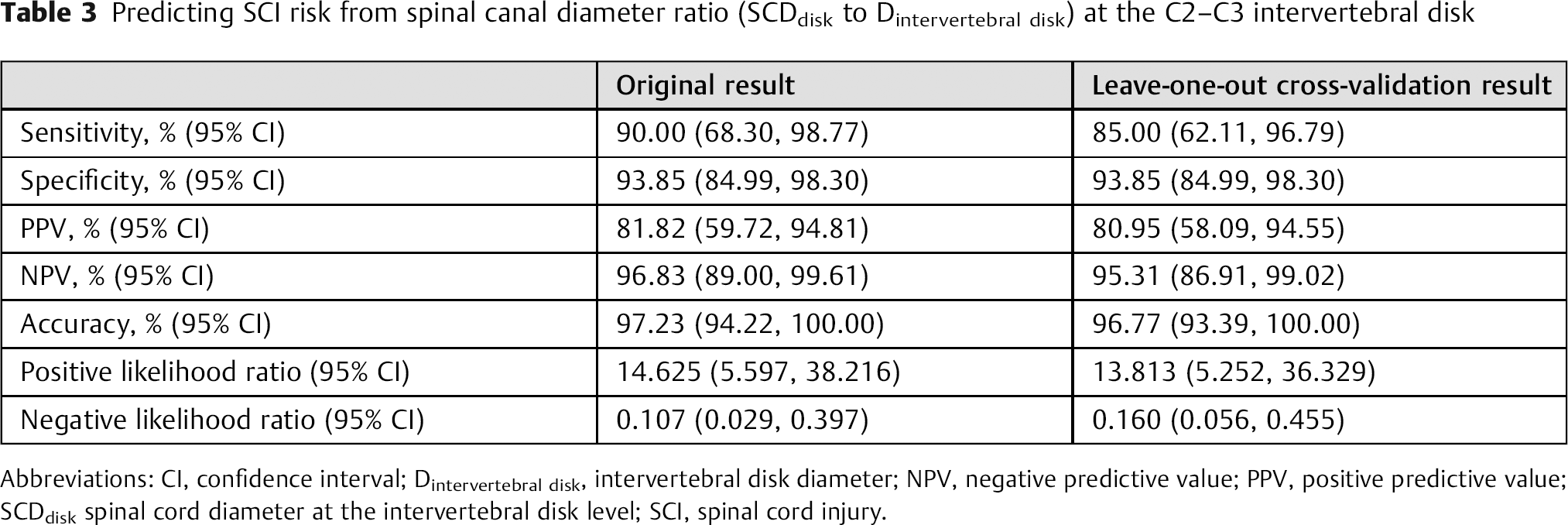
Abbreviations: CI, confidence interval; Dintervertebral disk, intervertebral disk diameter; NPV, negative predictive value; PPV, positive predictive value; SCDdisk spinal cord diameter at the intervertebral disk level; SCI, spinal cord injury.
Radiologic Parameters in Spinal Cord Injury Group
When the SCI group was divided into complete and incomplete injury subgroups, the SCDdisk-to-Dintervertebral disk ratio at the C4–C5 intervertebral disk level produced a statistically significant difference between the subgroups (p = 0.04, Table 4). In addition, high signal intensity on T2-weighted MRI was significantly more extensive in patients with complete injury (44.91 ± 11.39 mm) than in patients with incomplete injury (24.14 ± 14.41 mm, p = 0.04, Fig. 3).
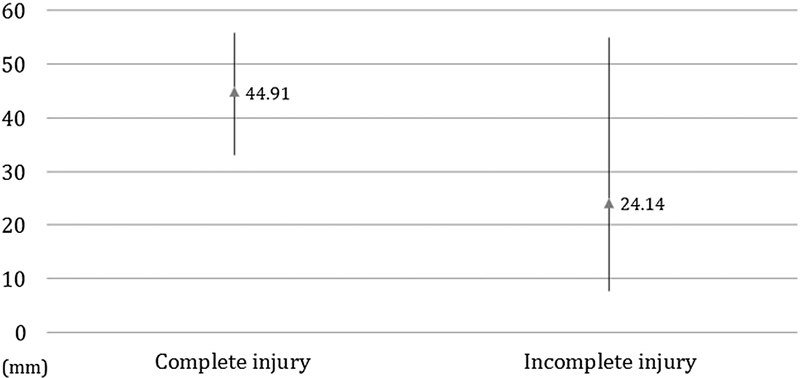
Extent of high signal intensity on T2-weighted magnetic resonance imaging (MRI) in subjects with complete and incomplete spinal cord injury. The amount of high signal intensity on T2-weighted MRI was significantly greater in patients with complete injury than in patients with incomplete injury (p = 0.04).
Radiologic parameters in patients with SCI with complete or incomplete injuries
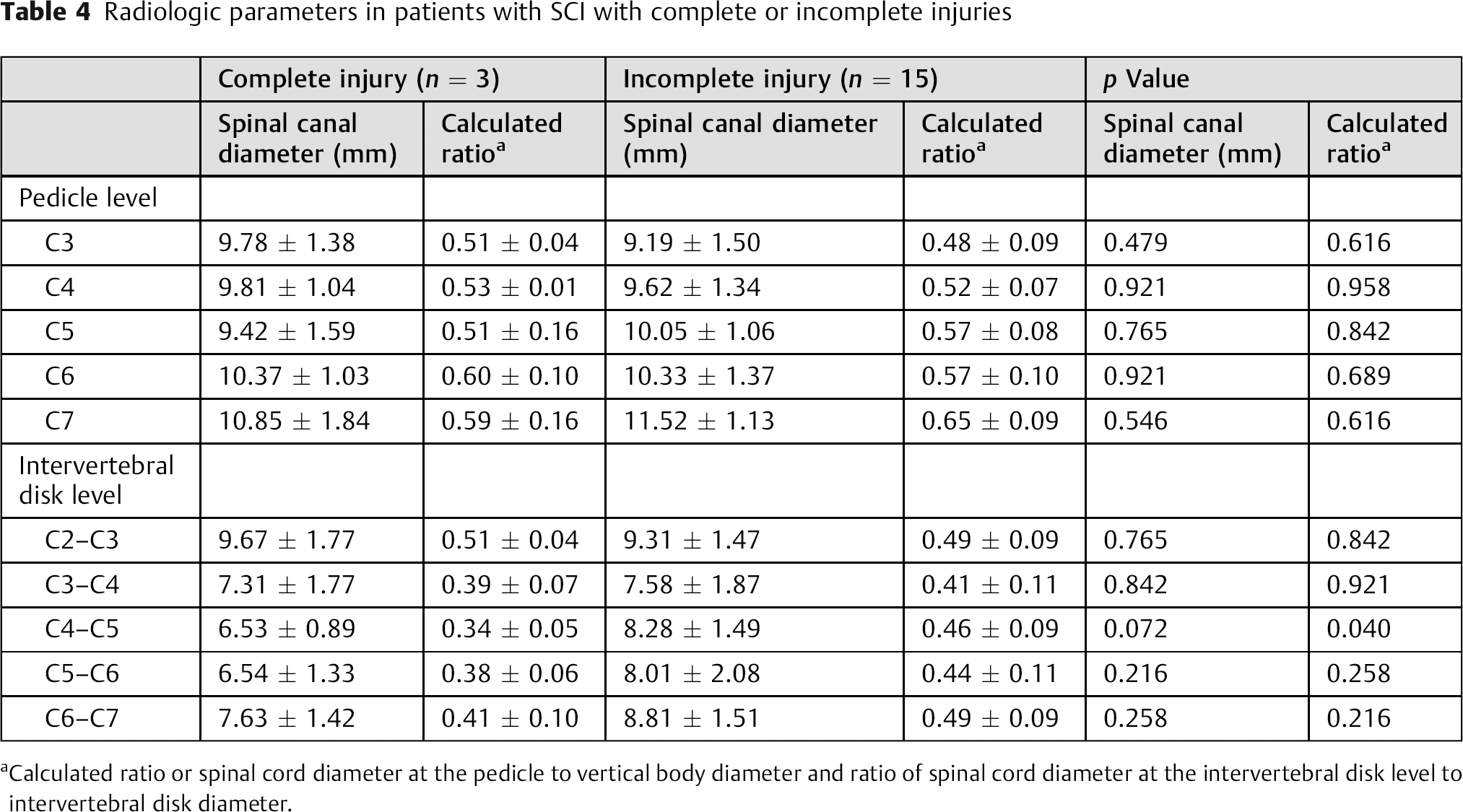
Calculated ratio or spinal cord diameter at the pedicle to vertical body diameter and ratio of spinal cord diameter at the intervertebral disk level to intervertebral disk diameter.
Discussion
Several studies have reported that a narrow ratio of spinal canal to the vertebral body (Torg-Pavlov ratio) might be an important risk factor for the development of cervical spondylotic changes and the occurrence of traumatic SCI. 5 , 16 , 17 , 18 , 19 The present study was focused on the risk prediction of traumatic SCI without subaxial fractures and dislocations compared with other studies. 18 , 19 Hyperextension of the cervical spine results in significant stenosis compared with that from flexion. In addition, the cerebrospinal fluid space is constricted in a narrow spinal canal. SCI could be the result of cord compression from an underlying osteophyte, PLL hypertrophy, OPLL, or hypertrophy of the ligamentum flavum accompanied by a narrow spinal canal. 5 , 16 , 17 Some authors have investigated correlations between spinal canal diameter or space available for the cord and the severity of neurologic deficits and have assessed the need for prophylactic surgery in patients with a narrow spinal canal. 18 , 19 , 20 , 21 In recent studies of European subjects, it was suggested that a Torg-Pavlov ratio cutoff value of 0.7 on plain radiography or a minimal disk-level canal diameter cutoff value of 8.0 mm on MRI provided a PPV useful in predicting the occurrence of SCI. 3 , 13 In the Korean population in this study, a cutoff value of 0.59 for the SCDdisk-to-Dintervertebral disk ratio at the C2–C3 intervertebral disk level yielded the greatest PPV for predicting the presence of SCI.
The mean sagittal spinal canal diameter at C1 to C7 is reported to range from 15.33 to 20.46 mm with maximal diameter at C1 and minimal diameter at C4. 22 , 23 , 24 In general, sagittal diameters in females are ∼1 mm smaller than in males at all vertebral levels. 22 The mean transverse diameters at the same levels range from 24.45 to 27.00 mm. 24 Torg et al reported that a ratio of 0.80 or less in spinal canal diameter to the vertebral body diameter indicated a high sensitivity for transient cervical neuropraxia. 25 In those studies, the diameters and ratios were derived from lateral radiographs, and the obtained measurements were significantly smaller than those obtained from CT images. 26 The measured spinal canal diameters and the calculated ratios in the present study were smaller than those previously reported, but these differences may be related to differences in spinal characteristics of Asian and European populations.
The spinal canal diameter at the C2–C3 level is typically wider than that of the subaxial cervical spine. Therefore, a narrow spinal canal at C2–C3 suggests the presence of marked spinal stenosis. Determination of a cutoff value at the C2–C3 intervertebral disk level may enable identification of patients with a narrow spinal canal. In addition, in our subjects with complete SCI after cervical trauma, a small SCDdisk-to-Dintervertebral disk ratio at the C4–C5 intervertebral disk level and the presence of extensive high signal intensity on T2-weighted MRI were associated with a poor clinical outcome. Therefore, regardless of the neurologic level, clinicians should determine such ratios when attempting to predict clinical outcome.
There is controversy about the use of prophylactic surgery for cervical spondylotic myelopathy. 27 , 28 Takao et al recently reported that the risk associated with the incidence of traumatic SCI in subjects with a cervical spinal stenosis was 124.5 times higher than that for subjects without a cervical spinal stenosis. 5 However, data from the Spinal Injury Network of Fukuoka, Japan suggested that only 0.017% of subjects with a cervical spinal stenosis might avoid traumatic SCI if they undergo decompression surgery before trauma. 5 Including the present study, several authors have reported that a narrow spinal canal is the most important risk factor associated with predicting SCI; however, sufficient evidence to recommend prophylactic surgical management of SCI is not yet available. 29 , 30 , 31 , 32 , 33 , 34 Because this was a retrospective study with a small number of patients, analyses of subjects stratified by ASIA group, injury mechanism, neurologic level, preoperative underlying cervical spinal disease, and postoperative neurologic status were not conducted. However, a significant difference between patients with complete and incomplete injuries was detected. Because these injuries may reflect different disease categories and may affect clinical outcome, analysis of underlying diseases including cervical spinal stenosis, OPLL, and PLL hypertrophy should be conducted. Therefore, a post-trauma study with a large number of patients with SCI should be undertaken. The optimal control group for such a study would be comprised of patients with cervical trauma but without neurologic symptoms. However, MRI evaluation has not been recommended after cervical clearance in patients with normal voluntary movement of neck after trauma. 35 Due to that limitation, an age- and sex-matched population between 40 and 80 years old that had cervical MRI evaluated for health screening was used as the control group in this study. Nevertheless, our results indicate that, in an elderly Korean population, a cutoff value of 0.59 for a SCDdisk-to-Dintervertebral disk ratio at the C2–C3 intervertebral disk level would yield the greatest PPV for the prediction of SCI. Furthermore, in our subjects with SCI with complete injury, there was a significantly low SCDdisk-to-Dintervertebral disk ratio at the C4–C5 intervertebral disk level and significantly more extensive high signal intensity on MRI.
Conclusion
All investigated MRI parameters in the SCI group were significantly smaller than in the control group. Small SCDdisk-to-Dintervertebral disk ratio at C2–C3 provided the greatest positive predictive value in SCI. In addition, when a cervical SCI has occurred, a small SCDdisk-to-Dintervertebral disk ratio at the C4–C5 level and the detection of >40 mm of high signal intensity on MRI are associated with a poor clinical outcome.
Disclosures
Soo Eon Lee, none
Chun Kee Chung, none
Footnotes
Acknowledgments
The authors thank the Medical Research Collaborating Center at the Seoul National University Hospital and the Seoul National University College of Medicine for its help with statistical analyses. This study was supported by a National Research Foundation of Korea grant funded by the Korean government (MSIP, 2010–0028631).