
Abstract
Study Design
Case report.
Objectives
Decompression of metastatic spinal cord compression has been shown to improve quality of life and prolong ambulation in patients undergoing palliative treatment. We report a case of metastatic cervical myelopathy treated with a combined approach using corpectomy and stabilization together with balloon kyphoplasty to allow adequate decompression and immediate stability in a patient with significant destruction of adjacent vertebral bodies.
Methods
The cervical spine was approached anteriorly and decompressed with a C7 corpectomy. Subsequent stability was achieved with insertion of a trabecular metal cage. Balloon kyphoplasty was used to treat lytic lesions within the posterior body of the adjacent vertebrae for pain relief and increased stability. Additional stability was achieved through the application of an anterior plate.
Results
Full limited decompression and stabilization were successfully achieved. The patient had no further neurologic deterioration and made modest improvements that allowed a return to independent ambulation.
Conclusion
This limited approach may be an option for patients with metastatic spinal cord compression, lytic destruction of adjacent vertebral bodies, and limited life expectancy.
Introduction
Metastatic cervical spine disease can be challenging to treat and has limited life expectancy and often multifocal disease. Balloon and radiofrequency kyphoplasty have both been used to reduce pain and the risk of collapse in the palliative treatment of painful metastatic cervical lesions. 1 Balloon kyphoplasty through a mini–open anterior approach has been successfully used to treat pain and restriction of movement in a patient with two-level cervical metastases from primary lung cancer. 2 There are no prior reports of its combined use with corpectomy in the cervical spine. Although cement leak is a reported complication of this technique, it is most often not clinically significant. 3
Cement augmentation has been widely used in the thoracolumbar spine to treat osteoporotic compression fractures adjacent to instrumented fusion procedures. 4 More recently, it has also been reported in the cervical spine. 5 The authors report on how balloon kyphoplasty in particular can be used to simultaneously treat lytic lesions in the posterior vertebral body and also augment the stability of an anterior cage and plate construct following C7 corpectomy. Where there is extensive lytic destruction of adjacent vertebra in a patient undergoing palliative treatment for carcinoma of the lung, balloon kyphoplasty allowed safe implantation of cement.
Case Report
A 77-year-old man presented to our service with primary lung carcinoma and an estimated life expectancy of 6 to 9 months. He complained of recent-onset axial neck pain and described symptoms of progressive myelopathic deterioration over several weeks. He failed to respond to 48 hours of high-dose dexamethasone and was unable to ambulate independently.
Magnetic resonance imaging showed cord compression behind a large lesion in the vertebral body of C7 with additional lytic lesions extending posteriorly within the C6 and T1 vertebral bodies (Fig. 1). Balloon kyphoplasty was used rather than simple vertebroplasty because of the anticipated risk of posterior cement leak and the less than optimal filling that may result during vertebroplasty.
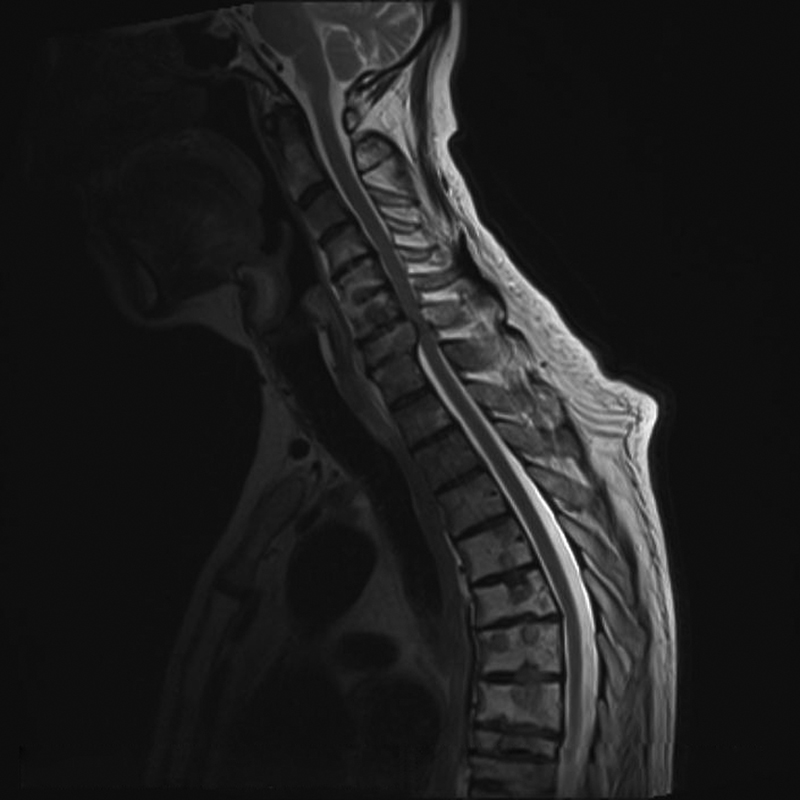
Sagittal T2-weighted magnetic resonance imaging demonstrating metastases within the vertebral bodies and cord compression at C7 with increased signal in the cord.
The lytic destruction of adjacent vertebral bodies was further visualized with computed tomography (Figs. 2 and 3).
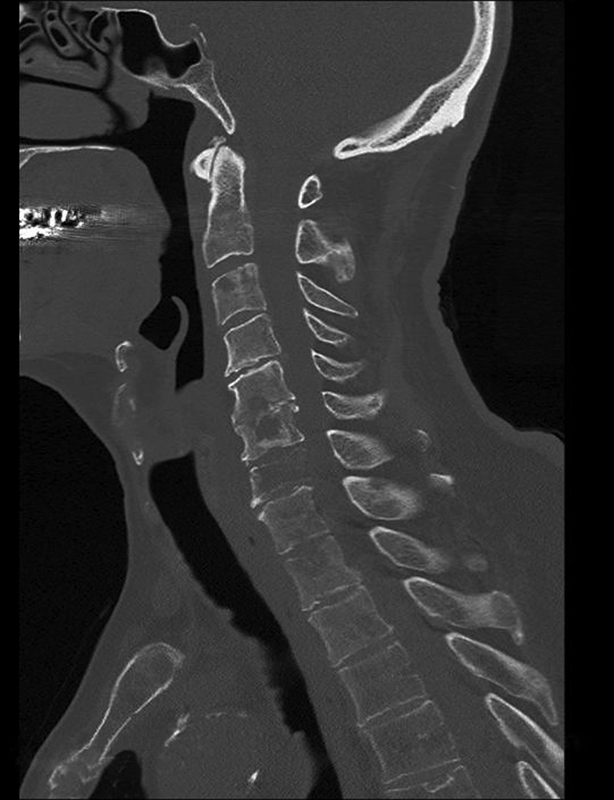
Sagittal computed tomography of the cervical spine showing large lytic lesions in C6 and C7 vertebral bodies.

Additional sagittal computed tomography of the cervical spine demonstrating further lytic destruction of the T1 vertebral body.
Metastatic deposits without neural compression can be treated with cervical balloon kyphoplasty. 6 Standard treatment of anterior cord compression might involve corpectomy and stabilization. Due to the adjacent vertebral involvement without neural compression and in view of the limited life expectancy, we decided that this patient might benefit from a limited combined procedure using balloon kyphoplasty to treat the painful adjacent lesions and standard surgical decompression of the cord at the compressed level.
A C7 corpectomy was first performed through an anterior approach to the cervical spine. This allowed full decompression of the cord. An anterior trabecular metal cage was inserted to regain stability. Using the same approach, anterior cervical kyphoplasty trocars were inserted into C6 and T1. Bone tamps were inflated to 400 psi. Cement augmentation was then performed under fluoroscopic guidance. At T1, an oblique beam allowed for best visualization as the cement was inserted. An anterior plate was applied during the 18 minutes of working time available with the cement used. This provided additional support to the adjacent vertebral bodies and allowed early postoperative mobilization of the patient without a cervical orthosis.
The patient recovered well in the postoperative period and noticed improvement in his myelopathic symptoms, neck pain, and mobility. Neck pain improved from 8/10 on a visual analog scale preoperatively to 3/10 at 2 weeks postoperation and 1/10 at 6 weeks. Unfortunately, some weeks later the patient was admitted to the hospital with a chest infection. He recovered from that episode and associated deterioration and went on to receive palliative radiotherapy. At 12-week follow-up, postoperative radiographs showed good implant position with no evidence of cage subsidence (Figs. 4 and 5). He remained ambulatory with minimal neck pain until his death from cancer-related complications 5.5 months following his procedure.

Postoperative lateral radiograph showing position of the implants and cement augmentation.

Postoperative anteroposterior radiograph showing position of the implants and cement augmentation.
Discussion
In this case, the combined presentation of axial neck pain and neurologic compression from metastatic spinal disease presented an opportunity to utilize a combined approach designed to maximize benefit and minimize risks in a patient with limited life expectancy.
Case series and reports suggest that vertebroplasty and kyphoplasty in the cervical spine can be used to treat painful metastatic deposits. 3 , 7 This is usually advocated through a minimal anterior approach to minimize the risks of percutaneous trocar insertion.
Treating this patient with posterior decompression through laminectomy or laminoplasty alone may have relieved neurologic compression but likely would not have addressed his axial neck pain. The addition of an instrumented fusion procedure would have increased stability and may have led to improved neck pain. When considering additional posterior stabilization, the risk remained of postsurgical kyphosis if the patient were to survive longer than expected, and the authors were also concerned about the morbidity and infection risk associated with posterior approaches.
Anterior corpectomy and stabilization of the symptomatic lesions would have involved multiple-level corpectomy and the subsequent morbidity associated with that approach.
A combined approach was chosen in an attempt to both maximize the decompression and achieve good postoperative stability. Balloon kyphoplasty was chosen to specifically treat the lytic vertebral lesions involving not only anterior but also posterior vertebral bodies. It was hoped that the increased stability achieved would lead to a reduction in axial pain.
The patient reported an improvement in neck pain and regained independent ambulation, which was our primary aim. He was able to perform many activities of daily living with minimal assistance. The patient was extremely satisfied with the procedure, and postoperative radiographs showed no evidence of cage subsidence at 12 weeks.
Conclusion
This case report shows that combined anterior cervical corpectomy and adjacent cement augmentation is technically feasible. The authors consider this a treatment option for patients with metastatic spinal cord compression, limited life expectancy, and widespread lytic lesions including the posterior aspect of the vertebral body.
Disclosures
Antony Bateman, none
Adam Way, none