
Abstract
Study Design
Retrospective case–control study.
Objectives
To confirm the fact that spinal cord dimensions are smaller in adults with Klippel-Feil syndrome (KFS) than in pediatric patients with KFS and to compare the clinical characteristics and outcomes of neurologic complications in patients with KFS with matched controls.
Methods
We performed an independent 1:2 case–control retrospective radiographic and chart review of a consecutive series of adults with KFS who underwent surgical intervention. The control group consisted of consecutive non-KFS surgical patients. Patients were matched in 1:2 case–control manner. Their charts were reviewed and the clinical characteristics were compared. Axial T2-weighted magnetic resonance imaging (MRI) was used to measure the anteroposterior and mediolateral axial spinal cord and spinal canal at the operative levels and measurements were compared.
Results
A total of 22 patients with KFS and 44 controls were identified. The KFS group had a tendency of more myeloradiculopathy, and the control group had a tendency toward more radiculopathy. Both tendencies, however, were not significantly different. MRIs of 10 patients from the KFS group and 22 controls were available. There was no difference in the area of both spinal cord and canal at the operative levels.
Conclusion
Contrary to the finding in previous reports on pediatric patients, there were no differences between KFS and well-matched control groups in terms of age of onset, presentation, revision rate, complication rate, surgical outcome, and cross-sectional spinal cord and canal dimensions at the operative level.
Introduction
Klippel-Feil syndrome (KFS) is a congenital anomaly characterized by fusion of one or more levels of the cervical spine.1 It is caused by improper segmentation of cervical vertebrae. 2 , 3 It is often associated with other anomalies including Sprengel deformity, 4 renal agenesis, 5 aortic or cardiac anomaly, 6 or impairment of hearing. 7
Various neurologic anomalies were also reported such as cervical cord dysraphism, diastematomyelia, and Chiari malformations. 8 These congenital neurologic anomalies are considered as the predisposing risk factors for higher neurologic complication in patients with KFS. 9 More importantly, hypermobility of the adjacent unfused segment and subsequent degenerative change were indicated as the cause of the higher rate of neurologic complication in patients with KFS. 10 , 11 Most recently, Auerbach et al reported that children with KFS, compared with age-matched controls, have a significantly smaller cross-sectional spinal cord area, which can be an additional risk factor for the higher neurologic complication rate in KFS. 12
Even though many studies support the higher prevalence of neurologic complication in KFS, it is still controversial. Nagib et al reported 43% of their cases required surgical decompression, 13 whereas Theiss et al reported that 22% of their cases had neurologic symptoms and only 6% of their patients required surgical decompression. 14 To the authors’ knowledge, there has been no study that compares KFS with matched controls in terms of clinical characteristics and outcomes after surgery.
This study addresses the following questions. First, is the spinal cord dimension smaller in adults with KFS compared with adults without KFS, as was found in pediatric patients with KFS? If a similar finding occurs in adults, it may predispose the KFS patient to a lower threshold for neurologic deficit. Second, do patients with KFS do as well with surgical treatment as matched controls without KFS in terms of complications and neck disability index (NDI) scores?
Materials and Methods
A consecutive series of adults (>18 years old) with KFS who underwent surgical intervention by a single surgeon between 1996 and 2007 were matched in 1:2 case–control manner according to gender and body mass index (BMI; malnourished, BMI < 18.5; normal weight, BMI 18.5 to 25; overweight, BMI 25 to 30; obese, BMI > 30). The control group was selected from a group of remaining surgical patients without KFS in the same period. We performed an independent 1:2 case–control retrospective radiographic and chart review.
Axial T2-weighted magnetic resonance imaging (MRI) was used to measure the anteroposterior and mediolateral axial spinal cord and spinal canal dimensions at the operative levels. The spinal cord and canal area were then calculated using the equation of an ellipse: area (ellipse) = π × (anteroposterior dimension) × (mediolateral dimension), a previously validated technique (Figs. 1, 2). 12 , 15 If there were multiple levels in a patient, the average area of the levels was used for comparison.
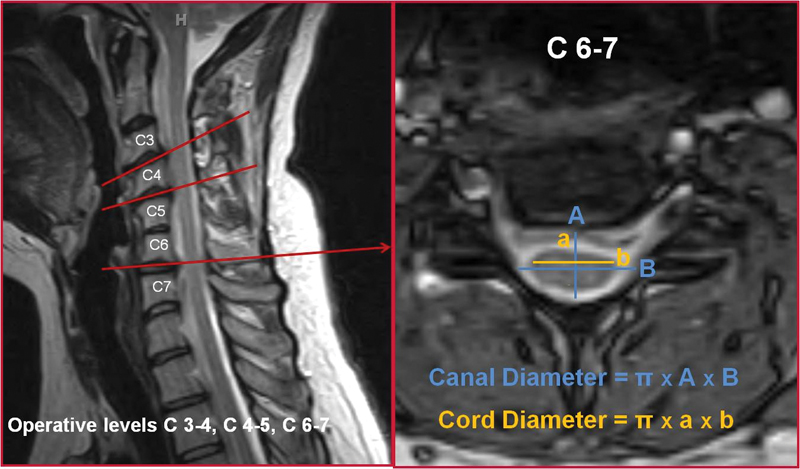
Measurement in patient with Klippel-Feil syndrome. Magnetic resonance imaging was used to measure the anteroposterior and mediolateral axial spinal cord and spinal canal dimensions at the operative levels.
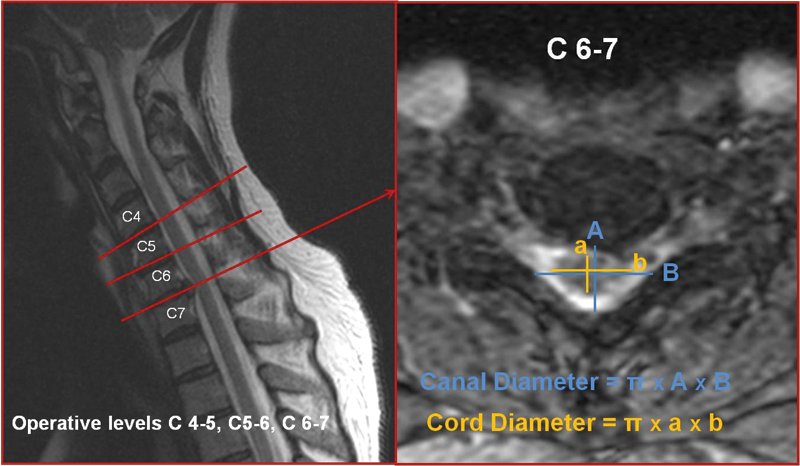
Measurement in control patient. With magnetic resonance imaging, the spinal cord and canal area were calculated.
Their charts were reviewed and the clinical characteristics were compared in terms of gender, preoperative symptoms, total number of fusions, incidence of revision surgery, complications, and pre- and postoperative NDI scores. Preoperative symptoms were compared in terms of myelopathy, radiculopathy, and myeloradiculopathy. The symptom categories were noted from the clinical charts dictated by the surgeon based on physical exam and patients’ symptoms.
Measured values of KFS and control groups were compared using the independent t test. However, for the nominal values (e.g., sex, age, symptoms), Pearson chi-square or Fisher exact test was used, depending on the expected count.
Results
A total of 22 KFS and 44 control patients were identified. The mean ages were 50.5 ± 12.5 and 50.5 ± 12.0 in the KFS and the control groups, respectively. The most common congenital fusion level was C2–3 followed by C3–4. Overall, 27% of patients had >1 congenital fusion level. In the KFS population, the surgical level was as follows: one level cephalad to the congenital fusion (17%), one level caudal to the congenital fusion (66%), and in between two congenitally fused areas (17%; Fig. 3). There was no difference in gender and age between the two groups. The KFS group had a tendency of more myeloradiculopathy, and the control group had a tendency toward more radiculopathy. Both tendencies, however, were not significantly different. No other clinical values were significantly different between the two groups. There was no statically significant difference in total number of levels fused, in number of revision surgery, in complication rates, and in pre- and postoperative NDI scores. MRIs of 10 KFS and 22 control group patients were available. There was no statically significant difference in the area of both the spinal cord and canal at the operative levels (Table 1).
KFS versus controls
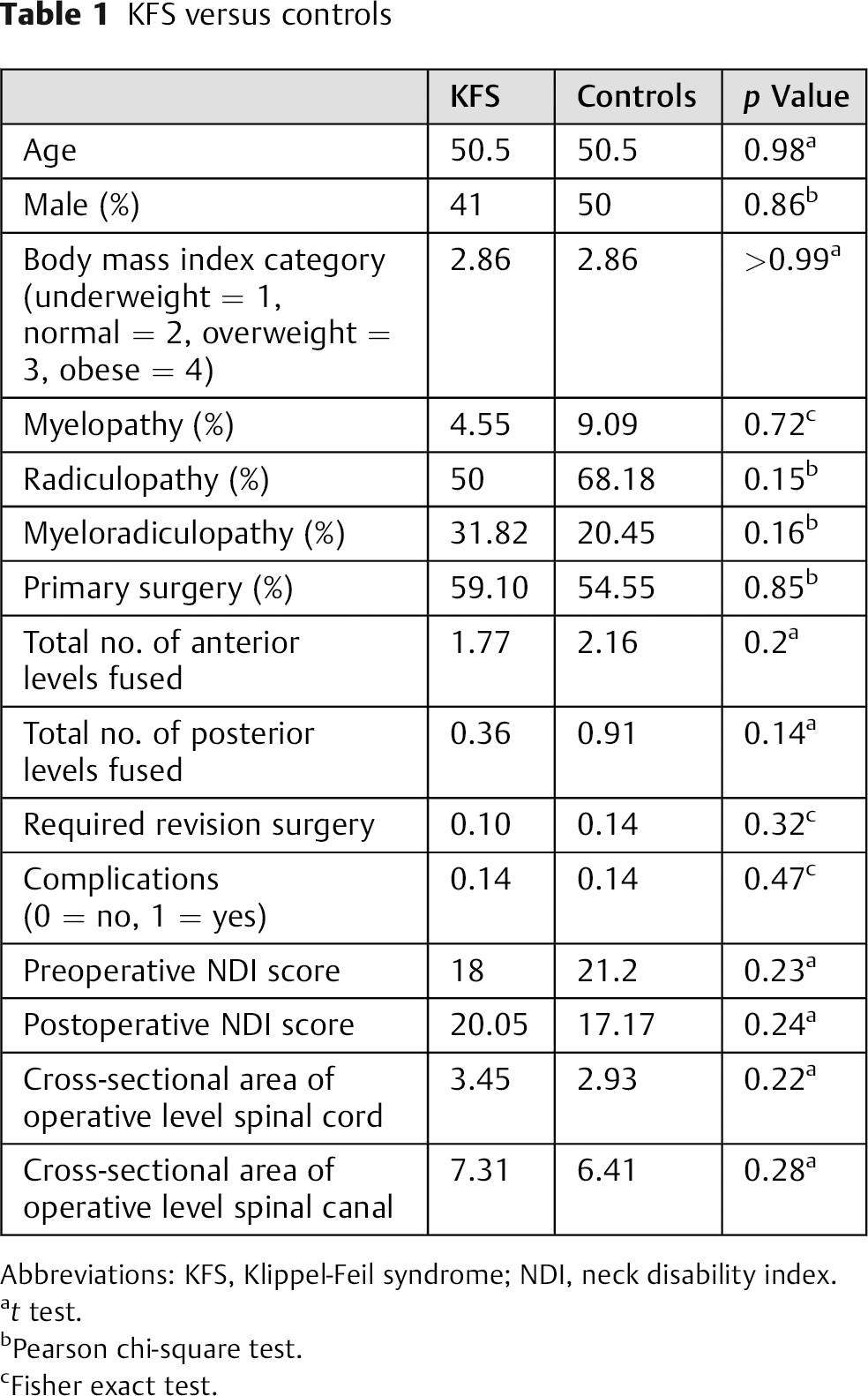
Abbreviations: KFS, Klippel-Feil syndrome; NDI, neck disability index.
t test.
Pearson chi-square test.
Fisher exact test.
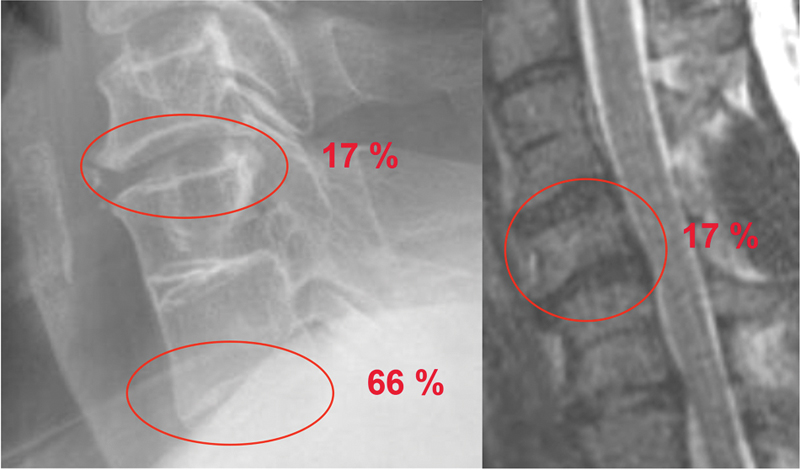
In the population with Klippel-Feil syndrome, the surgical level was: one level cephalad to the congenital fusion in 17%, one level caudal in 66%, and between two in 17%.
Discussion
KFS is a relatively rare disorder, with a prevalence rate of 0.71%. 16 In children, it has been reported that the cross-sectional area of the spinal cord is significantly reduced in patients with KFS versus patients without KFS. It has been suggested that such reductions may lead to higher rates of neurologic deficits. We undertook this study to determine whether the findings of reduced cross-sectional area of the spinal cord also occurs in adults, because that would suggest that adults with KFS are also predisposed to higher rates of neurologic deficits. Second, we sought to determine if patients with KFS who underwent surgery were more disposed to complications or poorer outcomes, as compared with non-KFS matched controls.
We compared 22 patients with KFS with 44 matched control group patients according to gender and BMI. Interestingly, the KFS group had a tendency toward more myeloradiculopathy, and the control group had a tendency of more radiculopathy. Because the KFS group was compared with a matched control group and both underwent decompressive surgeries, results do not reflect the prevalence of the neurologic complications in KFS or normal populations. However, considering the fact that there are many reports of sudden myelopathy or central cord syndrome after minor injuries in patients with KFS, 17 , 18 , 19 , 20 , 21 the fact that the KFS group had a tendency of more myeloradiculopathy rather than radiculopathy alone may be important. Spine surgeons who incidentally find patients with KFS should pay careful attention to the adjacent level of the fusion by possibly utilizing more advanced imaging or patient education.
We found C2–3 to be the most common congenital fusion level followed by C3–4. In the KFS group, the surgical level was most common at one level caudal to the congenital fusion (66%). Considering 17% of the surgical level was between two congenitally fused areas, 87% of overall surgical levels were located caudal to the fused vertebra.
Contrary to the findings in previous reports on pediatric patients, 12 there was no statically significant difference between the KFS group and the well-matched control group in terms of age of onset, presentation, revision rate, complication rate, surgical outcome, and cross-sectional spinal cord and canal dimensions at the operative level. This suggests that previous reports may have erred or that patients with KFS undergo a relative enlargement of the spinal cord as they grow. A strong correlation between decreased spinal cord diameter and the prevalence of neurologic symptoms was found in patients multiple sclerosis. 22 , 23 , 24 Also in severe compressive myelopathy, spinal cord dimension was correlated with the outcome. 25 , 26 , 27 In KFS, however, Samartzis et al advocated that increased space available for the cord would protect from neurologic complication instead of aggravating it. 28 Therefore, it is reasonable to deduce that the spinal cord enlarges as patients with KFS grow. Further studies, however, are required to elucidate this information.
There are several shortcomings with our study. First, the number of patients we evaluated was small. There were only 22 patients with KFS and only 10 had MRIs that were available, and post hoc power analysis showed the study was underpowered (Table 2). However, a case series study is subject to be underpowered by nature, and KFS is a relatively rare condition. Although our numbers are small, they nevertheless represent one of the larger series in the literature.
Post hoc power analysis
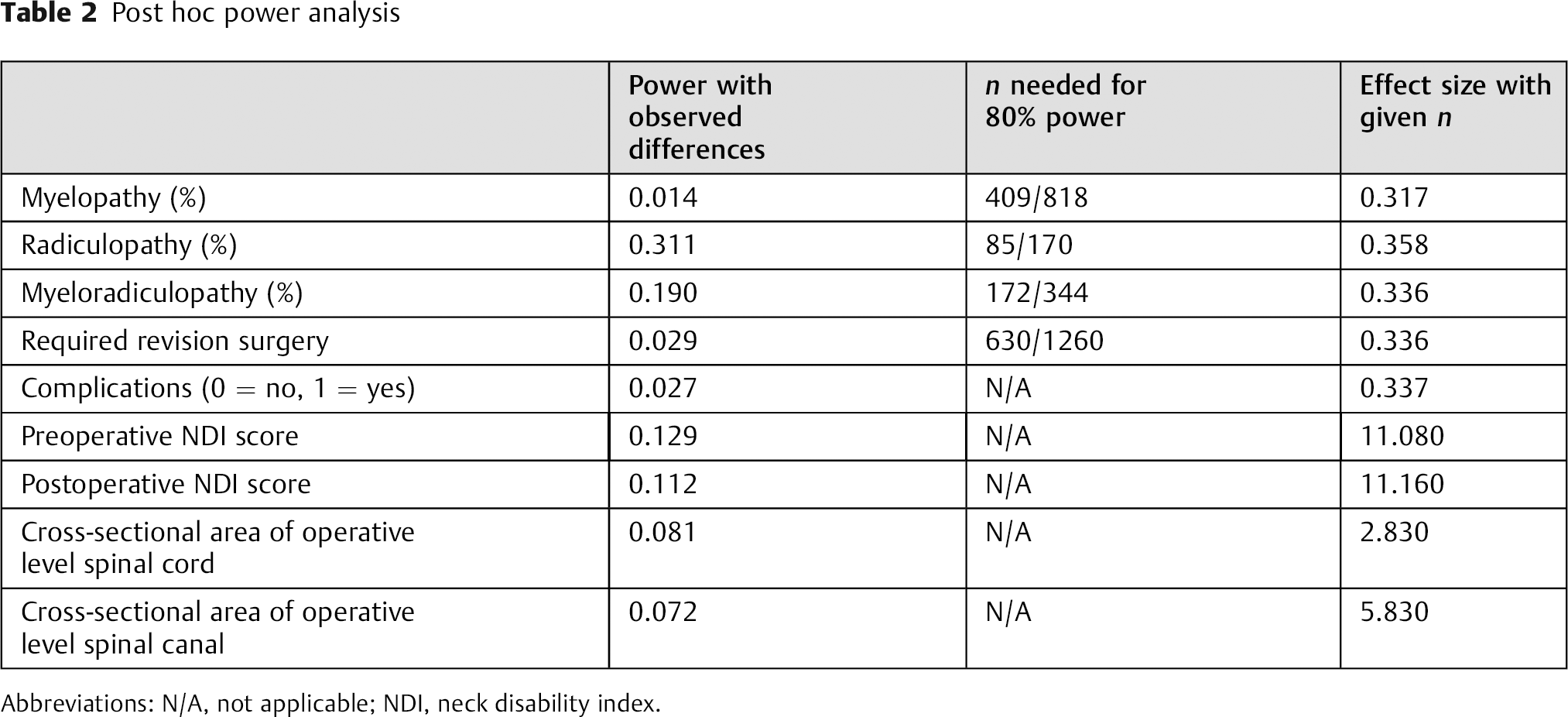
Abbreviations: N/A, not applicable; NDI, neck disability index.
In conclusion, it appears that patients with KFS who undergo surgery have similar outcomes as those without KFS, in terms of complication rates and NDI outcome measures. In addition, it appears that spinal cords of adults with KFS do not have smaller cross-sectional areas than spinal cords of non-KFS controls. If one believes the premise that smaller cross-sectional areas predispose to greater chance of neurologic deficits, at least it does not appear that patients with KFS are so predisposed based on this study with relative small number of cases. Therefore, further study with larger number of cases will be needed to confirm our conclusion.
Disclosures
Woojin Cho, none
Dong-Ho Lee, none
Joshua D. Auerbach, none
Jennifer K. Sehn, none
Colin E. Nabb, none
K. Daniel Riew, none