
Abstract
Study Design
In vitro biomechanical study.
Objective
To investigate the biomechanics of thoracolumbar burst and Chance-type fractures during fall from height.
Methods
Our model consisted of a three-vertebra human thoracolumbar specimen (n = 4) stabilized with muscle force replication and mounted within an impact dummy. Each specimen was subjected to a single fall from an average height of 2.1 m with average velocity at impact of 6.4 m/s. Biomechanical responses were determined using impact load data combined with high-speed movie analyses. Injuries to the middle vertebra of each spinal segment were evaluated using imaging and dissection.
Results
Average peak compressive forces occurred within 10 milliseconds of impact and reached 40.3 kN at the ground, 7.1 kN at the lower vertebra, and 3.6 kN at the upper vertebra. Subsequently, average peak flexion (55.0 degrees) and tensile forces (0.7 kN upper vertebra, 0.3 kN lower vertebra) occurred between 43.0 and 60.0 milliseconds. The middle vertebra of all specimens sustained pedicle and endplate fractures with comminution, bursting, and reduced height of its vertebral body. Chance-type fractures were observed consisting of a horizontal split fracture through the laminae and pedicles extending anteriorly through the vertebral body.
Conclusions
We hypothesize that the compression fractures of the pedicles and vertebral body together with burst fracture occurred at the time of peak spinal compression, 10 milliseconds. Subsequently, the onset of Chance-type fracture occurred at 20 milliseconds through the already fractured and weakened pedicles and vertebral body due to flexion-distraction and a forward shifting spinal axis of rotation.
Introduction
Compression and flexion-distraction injuries of the thoracolumbar spine, often associated with clinical instability, represent a subset 1 of spinal injuries that occur most often during motor vehicle crashes 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 and fall from height. 11 , 12 , 13 , 14 , 15 Over 65 years ago, Chance theorized that a horizontal split fracture through the spinous process, pedicles, and vertebral body was attributed to flexion load. 16 Prior to implementation of three-point lap-shoulder belts in automobiles, Chance-type fractures were most often reported in conjunction with intra-abdominal injuries in those restrained by a lap-only belt during severe frontal crashes. In 1973, Rennie and Mitchell hypothesized that flexion-distraction injuries were caused by excessive tensile force of the posterior spinal elements combined with vertebral body compression. 3 In a 2006 report of 53 patients with Chance-type fracture due to motor vehicle crashes, falls, or blunt or sports impact, Bernstein et al observed that over half had Chance burst fracture with retropulsion of the vertebral body cortex. 11 Ragel et al found a 38% incidence of flexion-distraction fractures of the thoracolumbar spine in soldiers within vehicles attacked by improvised explosive devices. 17
Previous biomechanical research has investigated mechanisms of thoracolumbar spine injuries in cadavers during simulated motor vehicle crashes. 18 Large compressive strain on the anterior vertebral body was observed immediately following impact with subsequent tensile strain during rebound. Others have investigated mechanisms of thoracolumbar injuries in human or bovine spinal segments during a simulated high-energy trauma using weight drop, 19 , 20 , 21 material testing apparatuses, 22 , 23 , 24 , 25 , 26 or vertical impaction of specimens affixed below a simulated torso mass. 27 Little work has been done to investigate spinal injury mechanisms during simulated fall from height. These fundamental data are needed as a baseline for evaluation of injury prevention systems and are valuable clinically for diagnosis and management of those sustaining thoracolumbar spine injuries during real-life falls.
The goal of this study was to investigate the biomechanics of thoracolumbar burst and Chance-type fractures during fall from height of a newly developed biomechanical model.
Methods
Overview
This study represents a continuation of our previous research. In our earlier work, 28 we described the development of the hybrid cadaveric/surrogate model for simulating a fall from height and evaluated its performance using a single specimen. The present study expands upon this earlier work to investigate mechanisms of thoracolumbar spine injuries during a simulated fall from height of additional specimens.
Specimen Preparation
Four three-vertebra human spinal segments from two female donors were prepared by dissecting all nonosteoligamentous soft tissues. Specimens 1 (T9–T10–T11) and 2 (T12–L1–L2) were prepared from a 74-year-old donor, and specimens 3 (L3–L4–L5) and 4 (T12–L1–L2) were prepared from a 72-year-old donor. The donors had no history of spinal disease or trauma. The upper and lower vertebra of each specimen was fixed within a resin mount. A combination of screws and wires were used to fix the vertebra rigidly within its mount. 29 Each mount had protruding bolts for subsequent attachment to a load cell in the surrogate dummy. No screws or wires were placed in the middle vertebra.
Hybrid Cadaveric/Surrogate Model
The hybrid model (Fig. 1a) was composed of the three-vertebra specimen mounted inside a crash test dummy (BioRID II, Humanetics Innovative Solutions, Plymouth, Michigan, United States). 28 The dummy components included the upper torso, upper thoracic spine, arms, and pelvis. We did not include the surrogate legs as our pilot studies demonstrated that leg inertial loads caused significant variability in lumbar and pelvic posture at impact and in the location of impact to the buttocks. The bolts within the upper and lower mounts were fixed to separate uniaxial load cells (upper: 10 kN ultimate load, model LCCA-750; lower: 40 kN ultimate load, model LCCA-3K; Omega Engineering, Inc., Stamford, Connecticut, United States). Compressive muscle forces were simulated using preloaded cables to stabilize the specimen in neutral posture and provide resistance to spinal motions during trauma. The total model mass was 46.9 kg. This included the upper torso above the upper mount, upper thoracic spine, and arms with cumulative mass of 31.7 kg plus the pelvis below the lower mount with mass of 15.2 kg. The torso was connected to the surrogate upper thoracic spine using laterally aligned studs. A steel plate with 5.0 kg mass, representative of head mass, was attached to the upper torso. Movie flags were rigidly fixed above and below the specimen.
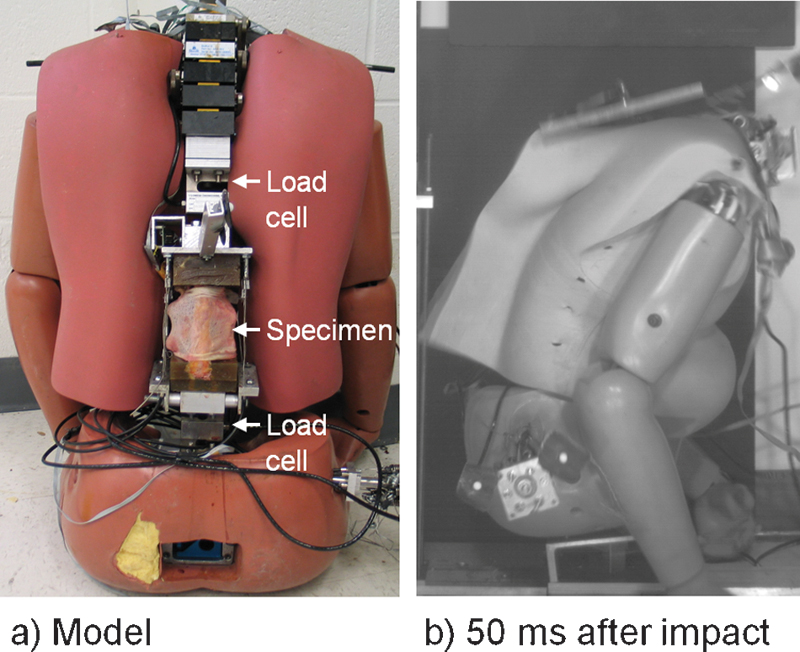
The newly developed model used to study the biomechanics of thoracolumbar burst and Chance-type fractures during fall from height. 28 (a) The model includes a spine specimen inside a crash dummy. Load transducers were fixed superior to and inferior to the specimen. (b) High-speed camera image at 50 milliseconds following impact demonstrating compression followed by flexion-distraction of the specimen within the impact dummy.
Fall from Height and Monitoring
Each specimen was subjected to a single fall onto the buttocks (Fig. 1b) from an average height of 2.1 m (standard deviation [SD] 0.1 m) with average velocity at impact of 6.4 m/s (SD 0.2 m/s). A custom experimental apparatus, built in our laboratory for vertical drop testing, included vertical linear bearings, a load cell fixed to the ground, a lift mechanism consisting of a ratchet hoist and pulley, and electromagnets at the top of the apparatus. The electromagnets were used to engage the steel head plate before simulating the fall. Impact loads at the ground were measured with a high-capacity load cell (40 kN ultimate load, model LCCA-3K; Omega Engineering, Inc.). A high-speed camera was used to record the falls at 500 frames/s (MotionPRO, Redlake MSAD, San Diego, California, United States). A LabVIEW program was written to control the electromagnet, initiate high-speed camera recording, and record the load data during the fall at 1 kHz (LabVIEW 8.5, National Instruments, Austin, Texas, United States).
Data Analyses
The load data and high-speed movies were used to determine the time-varying biomechanical responses during each fall from height. We analyzed the high speed movies using Matlab to track the movie flag markers and compute the motions of the spine specimen. The mean (SD) errors were −0.06 degrees (0.17 degrees) for rotation 30 and 0.3 mm (0.2 mm) for translation. 31 We double differentiated the marker translation data to obtain linear accelerations of the lower vertebra and filtered these data at 100 Hz using a third-order, dual-pass, Butterworth low-pass filter. We expressed the translations and accelerations in the ground coordinate system, which was fixed to the ground and had its positive z-axis oriented anteriorly, positive y-axis oriented superiorly, and positive x-axis oriented to the left, relative to the model pre-impact. Fluoroscopy, radiography, and detailed anatomical dissection were used to identify the injuries to the middle vertebra of each spine specimen. Ligamentous structures were evaluated to determine macroscopically identifiable partial or complete injuries.
Results
The time-varying biomechanical responses during the falls and post-trauma radiographs demonstrate specimen-specific responses and injuries (Figs. 2, 3, 4, and 5). The middle vertebra of all specimens sustained pedicle and endplate fractures with comminution, bursting, and reduced height of its vertebral body. Average peak compressive forces and accelerations occurred within 14 milliseconds of impact with forces reaching 40.3 kN at the ground, 7.1 kN at the lower vertebra, and 3.6 kN at the upper vertebra (Table 1). We observed lag time between the onset of compressive forces at the lower vertebra (lag time = 2.5 milliseconds, SD 0.4 milliseconds) and upper vertebra (lag time = 2.7 milliseconds, SD 0.2 milliseconds), relative to the onset of ground force. Subsequently, average peak flexion (55.0 degrees) and tensile forces (0.7 kN upper vertebra, 0.3 kN lower vertebra) occurred between 43.0 and 60.0 milliseconds (Table 1). Peak tension force occurred first at the upper vertebra at 49.3 milliseconds followed by the lower vertebra at 60.0 milliseconds. Hyperflexion was demonstrated by vertebral motions consisting of posterior translation at the lower vertebra (Figs. 2d and 3d) and posterior followed by anterior translations at the upper vertebra (Fig. 3d).
Average force, acceleration, and rotation peaks and occurrence times during fall from height, ordered chronologically
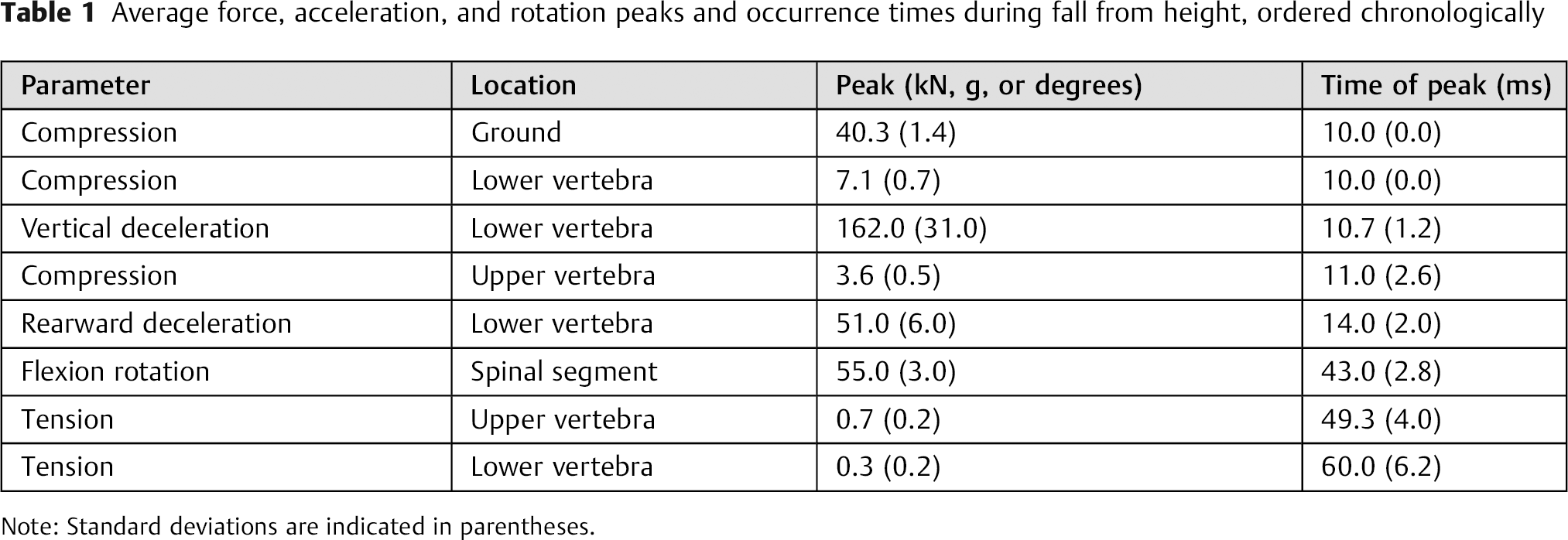
Note: Standard deviations are indicated in parentheses.
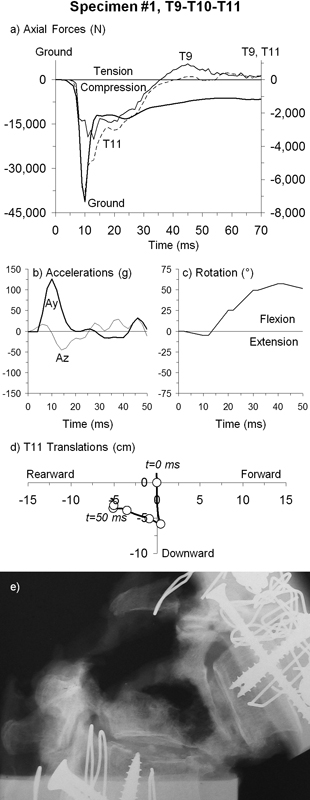
Specimen 1, T9–T10–T11. Time history responses during fall from height for: (a) axial forces at the ground and T11 and T9 vertebrae; (b) vertical (Ay) and horizontal (Az) accelerations of T11; (c) rotation of T9 relative to T11; and (d) T11 translations at 10-millisecond intervals in the ground coordinate system. (e) Post-trauma sagittal radiograph of the flexed spine.
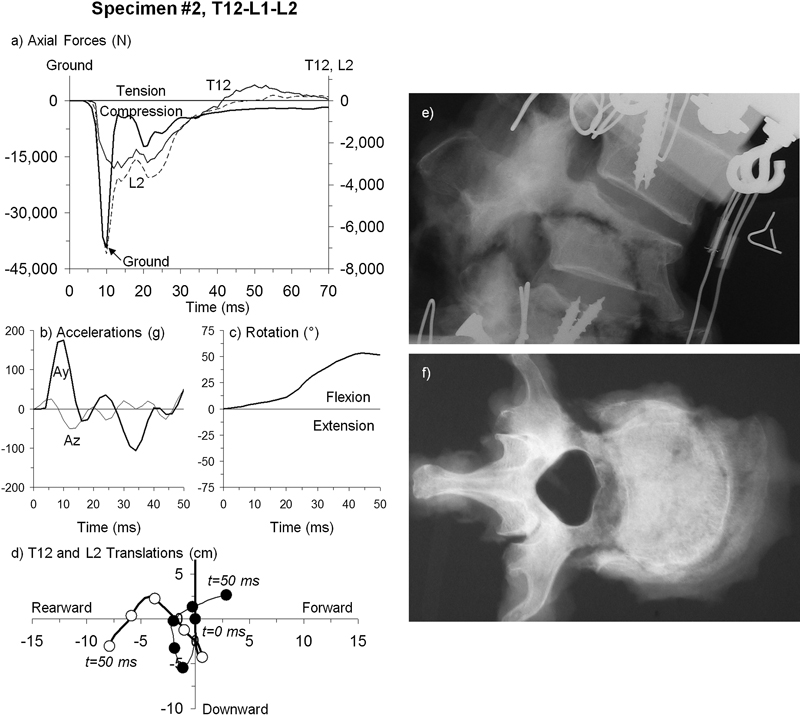
Specimen 2, T12–L1–L2. Time history responses during fall from height for: (a) axial forces at the ground and L2 and T12 vertebrae; (b) vertical (Ay) and horizontal (Az) accelerations of L2; (c) rotation of T12 relative to L2; and (d) translations of T12 (closed black circles) and L2 (open white circles) at 10 milliseconds intervals in the ground coordinate system. Post-trauma radiographs: (e) sagittal and (f) superior.
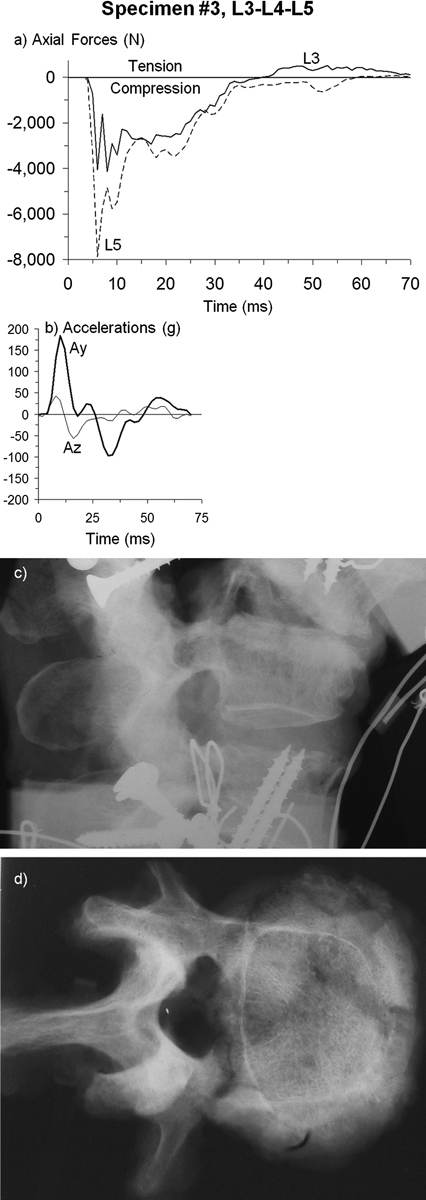
Specimen 3, L3–L4–L5. Time history responses during fall from height for: (a) axial forces at the L5 and L3 vertebrae and (b) vertical (Ay) and horizontal (Az) accelerations of L5. Post-trauma radiographs: (c) sagittal and (d) superior.
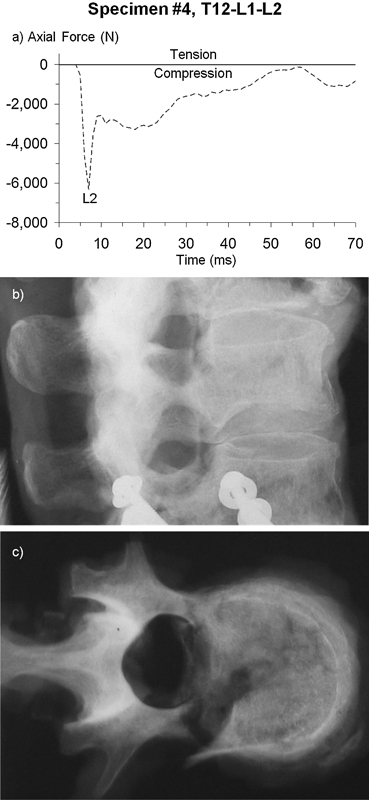
Specimen 4, T12–L1–L2. Time history responses during fall from height for: (a) axial force at the L2 vertebra. Post-trauma radiographs: (b) sagittal and (c) superior.
Compression and flexion-distraction injuries were observed in all specimens. In specimen 1 (T9–T10–T11), complete ruptures of the T9/10 ligaments were observed for the ligamentum flavum and posterior capsular, interspinous, and supraspinous ligaments. A horizontal split fracture was observed at T10 entering through the laminae at the posterior region of its upper facets, through the pedicles, and extended anteriorly through its vertebral body (Fig. 2e). The T10 spinous process was not fractured. In specimen 2 (T12–L1–L2), ligamentous injuries were observed at L1/2 (complete) and T12/L1 (partial) in the ligamentum flavum and posterior capsular, interspinous, and supraspinous ligaments. A horizontal split fracture was observed at L1 through its pedicles and extended anteriorly through its vertebral body (Fig. 3e). No macroscopic ligamentous injuries were observed in specimens 3 or 4. In specimen 3 (L3–L4–L5), reduced vertebral body height and compression of L4 was apparent from the sagittal radiograph, particularly anteriorly (Fig. 4c) with upper endplate fracture and right partial pedicle fracture (Fig. 4d). In specimen 4 (T12–L1–L2), the L1 vertebra sustained bilateral pedicle fractures and more severe fracture of the upper endplate as compared with the lower endplate (Figs. 5b and 5c).
Discussion
We investigated mechanisms of thoracolumbar burst and Chance-type fractures during a simulated fall from height in a newly developed model (Fig. 1). The model was composed of a human spine specimen inside a crash dummy. We observed clinically relevant compression and flexion-distraction injuries including Chance-type fractures. The T10 fracture pattern of specimen 1 (Fig. 2e) was similar to a Type II Chance fracture described by Gumley et al, 4 in which the fracture line entered the laminae at the base of the spinous process. We observed complete injuries to the posterior ligaments at T9/10 in this specimen and retropulsion of the posterior vertebral body cortex consistent with an associated burst component combined with Chance-type fracture described by Bernstein et al. 11 The fracture pattern in this specimen was similar to that described by Magerl et al, 1 consisting of flexion subluxation with bilateral facet fracture associated with complete burst fracture (classification B1.2.3 + A3.3). In specimen 2, the L1 fracture line entered at the pedicles and extended anteriorly through its vertebral body (Fig. 3e). In this specimen, macroscopically identifiable injuries were observed in the posterior ligaments at T12/L1 and L1/2. Specimens 3 and 4 (Figs. 4c, 4d, 5b, and 5c) exemplified injuries that were observed in all specimens: pedicle and endplate fractures with comminution, bursting, and reduced vertebral body height. The range of thoracolumbar spine injuries observed in the present specimens, including osseous fractures with and without complete injuries of the posterior ligamentous complex, suggests varying clinical instability and neurologic injuries in fall from height patients.
Based upon clinical case series 3 , 5 , 9 , 11 and biomechanical experiments, 18 hypotheses exist regarding the mechanism of Chance burst fracture of the thoracolumbar spine in individuals restrained by a lap-only belt during a motor vehicle crash. Smith and Kaufer theorized that the lap-belt acted as a fulcrum at the anterior abdominal wall, subjecting the thoracolumbar spine to flexion-distraction injuries. 9 To explain combined Chance and vertebral body compression fractures, Rennie and Mitchell theorized that the spinal axis of rotation was near the posterior longitudinal ligament. 3 Gertzbein and Court-Brown suggested that the burst fracture occurred during the rebound phase after the spine was weakened by the Chance fracture. 5 Bernstein et al postulated that the spinal axis of rotation shifted posteriorly from the anterior abdominal wall to the vicinity of the posterior longitudinal ligament during the crash. 11 The incidence of Chance fracture during frontal crashes has been reduced, but not eliminated, due to the implementation of three-point lap-shoulder belts. Submarining, or displacement of the pelvis under the lap belt causing spinal hyperflexion, has been theorized as the mechanism causing Chance fracture in those restrained by a three-point belt. 32 , 33 Ragel et al postulated various mechanisms of thoracolumbar spine fractures in soldiers within vehicles attacked by improvised explosive devices, all of which involved hyperflexion with or without restraint systems. 17
The mechanism of a Chance-type fracture with an associated burst component of the thoracolumbar spine during a traumatic fall may be deduced using our present data. Following the buttocks’ impact with the ground, the spine specimen was subjected to an injurious compressive load, largest at the lower vertebra as compared with the upper vertebra (peak 7.1 kN versus 3.6 kN, Table 1), with an average pulse duration of 39 milliseconds. Lag time between the onset of axial load at the ground to the lower vertebra to the upper vertebra indicated transfer of load superiorly. Our maximum peak spinal load exceeded previously reported tolerance data of cadaveric spine specimens subjected to compression load at various loading rates: between 2.4 and 3.2 kN at 0.0065 m/s, 34 3.3 kN at 0.01 m/s, 35 between 2.8 and 5.8 kN at 0.1 m/s, 22 and 4.2 kN at 2.5 m/s. 35 These comparative data indicate high likelihood that the pedicle, vertebral body, and burst fractures of our specimens occurred very early, at approximately the time of peak spinal compression, 10 milliseconds. Flexion rotation was minimal at this time (Figs. 2c and 3c).
A sharp increase in flexion rotation was subsequently observed beginning at 20 milliseconds (Fig. 3c), suggesting the onset of the Chance-type fracture through the already fractured and weakened pedicles and vertebral body. Spinal load transitioned from compression to tension at 39 milliseconds, the approximate time of peak flexion rotation, with the greatest peak tension occurring at the upper vertebra compared with lower (0.7 kN versus 0.3 kN, Table 1). These loads were between 4 and 19% of the peak compressive loads during the fall and between 11 and 25% of that previously reported to cause flexion-distraction failure in lumbar functional spinal units (2.8 kN). 36 These comparative data indicate that the early injurious compression loads and fractures predisposed our specimens to subsequent flexion-distraction injuries. The continued momentum of the torso center of mass, with its position anterior to the spine, caused spinal tension, distraction, and flexion. The tensile spinal forces yielded fracture lines approximately perpendicular to their lines of application (Figs. 2e and 3e), consistent with that theorized by Rennie and Mitchell. 3
In flexion, the axis of rotation for intact lumbar functional spinal units lies in the vicinity of the posterior longitudinal ligament, 37 and for the thoracic spine, it is inferior to the nucleus pulposus. 38 The initial compression fractures sustained by our specimens immediately following impact may have altered the normal rotation center during the subsequent flexion-distraction phase. Nonetheless, we hypothesize that the spine axis of rotation in our specimens was initially near the posterior longitudinal ligament and subsequently shifted anteriorly, causing the Chance-type fracture to enter the anterior vertebral body. Although future research is needed to evaluate this hypothesis, evidence is provided by the post-trauma sagittal radiographs (Figs. 2e and 3e), which indicate a rotation center at the anterior vertebral body.
Our study has limitations inherent to cadaveric research models. Complete biomechanical response data were not available for all specimens due to isolated instances of transducer malfunction. Our high-energy experiment was complex and required significant preparation and pilot work. We presented all data that were deemed accurate representations of the biomechanical responses. Due to a lack of young cadaveric material, our sample size was limited to four spine segments with an average age of 73 years, which precluded investigation of the large variety of fractures observed clinically. 4 The three-vertebra specimens were from distinctly different regions of the spine from T9 through L5. The severity of thoracolumbar spine injuries in younger individuals, who are more prone to sustain falls from high heights, would most likely be less than that reported in the present study. We did not measure bone mineral density of the spinal segments, which was likely correlated with failure force. The small sample size precluded statistical analyses of the response data. Our model included a cadaveric spine segment mounted within a surrogate spine. The surrogate components represented 50th percentile male results and produced biomechanical responses that were stiffer than those of specimen-specific anatomical components. Our model enabled measurement of spinal loads, data that are not easily obtained from a whole cadaver model. Our model produced clinically relevant thoracolumbar spine fractures in a realistic fall from height scenario including burst fractures with (specimens 1 and 2; Figs. 2 and 3) and without (specimens 3 and 4; Figs. 4 and 5) Chance-type fracture. Traumatic compression was transferred to the cadaveric spine due to rapid deceleration of the buttocks and downward momentum of the upper body weight. Other biomechanical models of high-energy trauma, such as those using weight drop or material testing apparatuses, cannot fully replicate the injury mechanism during fall from height.
We determined mechanisms of thoracolumbar burst and Chance-type fractures due to simulated fall from height. Loads consisting of injurious compression followed by flexion-distraction were observed. Peak compression force and bony failure occurred within 10 milliseconds of impact. Chance-type fractures due to flexion-distraction were observed. Continued clinical and biomechanical studies will ultimately lead to improved prevention measures and reduced frequency and severity of traumatic thoracolumbar spine injuries.
Disclosures
None
Footnotes
Acknowledgments
We thank Dr. Xiao Han, MD, for thoughtful discussion.