
Abstract
Study Design
Case report.
Objective
To report the case of one patient who developed a giant, completely calcified, juxtafacet cyst.
Methods
A 57-year-old woman presented with a 2-year history of progressively worsening lower back pain, left leg pain, weakness, and paresthesias. Imaging showed a giant, completely calcified mass arising from the left L5–S1 facet joint, with coexisting grade I L5 on S1 anterolisthesis. The patient was treated with laminectomy, excision of the mass, and L5–S1 fixation and fusion.
Results
The patient had an uncomplicated postoperative course and had complete resolution of her symptoms as of 1-year follow-up.
Conclusions
When presented with a solid-appearing, calcified mass arising from the facet joint, a completely calcified juxtafacet cyst should be considered as part of the differential diagnosis.
Introduction
Juxtafacet cysts (JFCs) are uncommon intraspinal, extradural lesions that arise from the facet joints. JFCs can be further distinguished as either synovial cysts, if histology confirms the presence of a synovial lining membrane, or alternatively as a ganglion cyst, if no such membrane is present. However, few differences exist between the two in terms of diagnosis and management. 1 , 2 , 3 , 4 , 5 , 6 , 7 Their pathogenesis remains unclear, with most authors citing excessive joint mobility leading to synovial fluid herniation through joint capsule defects. 2 , 4 , 7
Calcification in the cyst walls is a common finding on imaging for JFCs, appearing as peripheral areas of high attenuation on computed tomography (CT) and peripheral hypointensity on T1- and T2-weighted magnetic resonance imaging (MRI). 8 , 9 , 10 But although calcification of the cyst walls are commonly reported findings, 9 , 10 , 11 complete calcification of the cyst is exceedingly rare. 11 , 12 , 13 We present here an unusual case of a JFC presenting as a giant, multilobular, completely calcified mass with significant extraforaminal extension.
Case Report
The patient was a 57-year-old woman who presented with a 2-year history of gradually worsening lower back and left leg pain. She also reported numbness in her left heel and foot and subjective weakness in the left foot. Her past medical history was significant for hypothyroidism, hypertension, mild levoscoliosis, rheumatoid arthritis, and scleroderma managed on weekly methotrexate injection. Her past surgical history was negative for any previous lumbar surgeries, but the patient had received multiple cervical surgeries resulting in C3–C7 fusion. On neurologic exam, the patient was found to have decreased strength in plantarflexion and dorsiflexion of the left lower extremity but was otherwise nonfocal.
The patient's imaging was most notable for a large, multilobular mass, measuring 54 × 31 × 30 mm, arising from the left L5–S1 facet joint that had caused destruction of the joint itself and that showed severe encroachment of the adjoining foramen, with coexisting grade I anterolisthesis of L5 on S1. The lesion was hyperdense on plain radiograph (Fig. 1) and on CT imaging (Fig. 2a, 2b, and 2c) and appeared hypointense on T1- and T2-weighted MRI sequences (Fig. 3a and 3b, respectively).

Preoperative plain film of the lumbar spine showing a large, completely calcified lesion extending out from the L5–S1 intervertebral space.
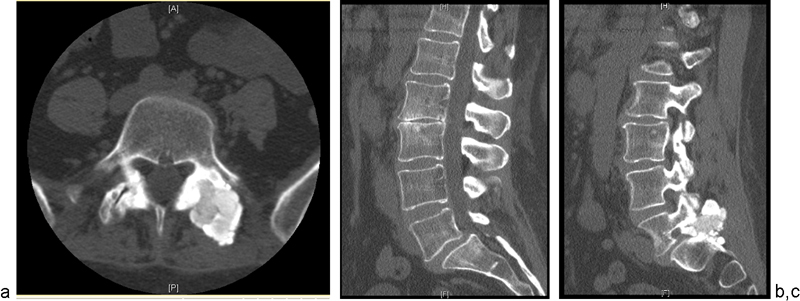
(a) Axial computed tomography (CT) image taken preoperatively, showing the origin of the lesion from the left L5–S1 facet joint. (b) A preoperative midsagittal CT image demonstrating grade 1 anterolisthesis of L5 on S1. (c) A preoperative sagittal CT image demonstrating foraminal stenosis at L5–S1 caused by the lesion.
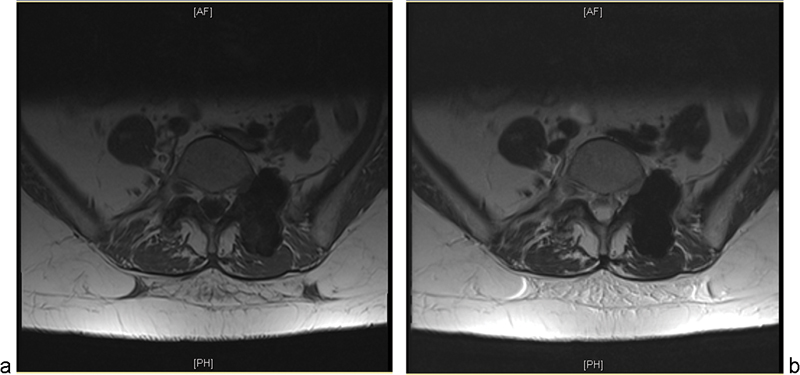
(a) T1-weighted magnetic resonance image (MRI) of the same lesion, which appears uniformly hypointense. (b) T2-weighted MRI, also demonstrating uniform hypointensity.
The patient underwent an L5 laminectomy for excision of the mass along with an L5 to S1 fixation and fusion. Intraoperatively, the lesion was noted to consist of a pastelike material that was compressing the thecal sac and that extended ventrally out of the foramen. Histologic analysis identified the lesion as a mineralized simple pseudocyst, containing mineralized proteinaceous material that did not refract plane polarized light after ethanol fixation (Fig. 4a and 4b). No lining epithelium was visualized.
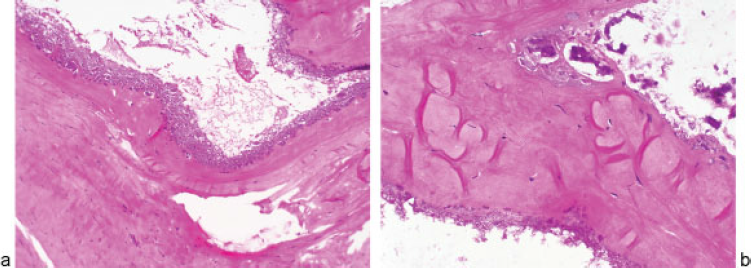
(a) Hematoxylin and eosin–stained sections of the resection reveal dense membranous fibrous connective tissue separating spaces associated with dense calcifications as well as smaller loculated spaces filled with calcium (×20 magnification). (b) Higher magnification (×40) reveals the wall of the spaces to be associated with granular calcifications and no obvious cellular lining.
The patient experienced no intraoperative or postoperative complications, and her postoperative hospital course was unremarkable. By postoperative day 2, the patient had recovered full strength in her extremities but still had some residual numbness, and she was discharged to home in stable condition on postoperative day 3. At 2-year follow-up, the patient continued to be free of her lower extremity pain and weakness and had not experienced any subsequent postsurgical complications (Fig. 5a and 5b).

(a) Postoperative plain film (anterior-posterior) showing removal of the mass and placement of fixation hardware. (b) Lateral view of the same.
Discussion
Mineralized, extradural lesions of the lumbar spine arising from the facet joint are uncommon causes of spinal pathology. The differential diagnosis consists of several uncommon disorders, including synovial osteochondromatosis, 14 tumoral calcinosis, 15 tumoral calcium pyrophosphate dehydrate crystal deposition disease (pseudogout), 16 and lumbar presentation of ossification of the ligamentum flavum. 17 The case we present here represents another potential consideration in that differential diagnosis.
Completely calcified JFCs are rare, with only a handful of instances existing in the literature. Almefty et al presented four patients with multiple-level, bilateral, consistently calcified thoracic spinal cysts. 12 These lesions were atypical due to their number, location, and mineralization. Kasliwal and Deutsch presented on the case of a unilateral lumbar JFC at the L4–L5 level. 13 Similar to our case, the patient presented with radicular symptoms in the setting of a lumbar lesion that appeared hypointense on T1- and T2-weighted MRI. It should be noted that calcification of JFCs can result from treatment as well, as Métellus et al noted a case of a cyst undergoing complete calcification after intracystic steroid injection therapy. 11
The case presented here was remarkable not just for its mineralization but also for its size. JFCs have typically been recorded to be between 10 and 20 mm in diameter at their widest dimension on imaging. 10 , 18 The case we report here, however, measured 54 mm at its widest dimension, showing significant extension into nearby structures. Moreover, although JFCs frequently extend into the spinal canal and cause compression of the thecal sac, 2 the majority of the lesion in our case existed outside the spinal canal. This may explain how the cyst grew to be so large before the patient presented for evaluation.
It should also be noted that our patient's medical history included rheumatoid arthritis and scleroderma, and systemic inflammatory diseases have been associated with JFCs in the past. 1 , 19 Moreover, inflammatory arthritides are known to contribute to the pathogenesis of synovial cysts outside of the spine. 20 However, no studies to date have established systemic inflammation as a risk factor for JFC development, and the role of inflammatory joint disease in the pathogenesis JFCs remains unclear.
Many methods of treating JFCs have been described, including simple laminotomy with cystectomy and the potential addition of a laminectomy, hemilaminectomy, mesial facetectomy, or foraminotomy. 3 , 4 Minimally invasive approaches with tubular retractors have also been described. 19 , 21 In terms of treatment of this patient, it was presumed that the symptoms of back pain were secondary to facet dysfunction and that the left-sided plantar flexion weakness was due to foraminal stenosis. Due to the size and mineralization of the lesion, it was felt that a complete facetectomy was needed to adequately address the underlying pathology, necessitating a concurrent fusion.
Our case highlights the significant variation that exists in the size, location, and content of JFCs. Although uncommon, JFCs should be considered in the differential diagnosis of lesions arising from the facet joint, even if they appear calcified and noncystic in nature.
Disclosures
None
Footnotes
Acknowledgments
We would like to acknowledge Dr. Roger McLendon for his assistance with preparation of the pathology slides.