
Abstract
Objective
To gain a greater understanding of anomalous insertions of the anterior horn of the medial meniscus through evaluation of a rare case and a review of the existing literature on medial meniscus malformations.
Methods
This report describes a 26-year-old man with an anomalous insertion of the anterior horn of the medial meniscus combined with symptomatic hypertrophy of the anterior horn and a synovial cyst. We also conducted a review of the existing literature on medial meniscus malformations using five major scholarly literature databases and search engines.
Results
The literature review revealed that the incidence of anomalous insertions of the anterior horn of the medial meniscus is 0.5% to 2.8%. Not all patients undergo surgical excision; some are only symptomatically treated. In our patient, the arthroscopic view was consistent with the imaging characteristics. No special operation was performed to treat the anomalous insertion. At the 18-month follow-up, the patient had no symptom recurrence and had returned to practicing sports.
Conclusion
The pain during hyperextension in our patient was caused by a cyst and anterior horn hypertrophy. If the symptoms in such cases are not caused by the anomalous insertion, no special treatment is needed.
Keywords
Introduction
Congenital meniscal abnormalities are rare. The most common meniscal anomaly is the discoid meniscus, which is more often seen in the lateral than medial meniscus and is more prevalent in Asians than in patients of other ethnicities. 1 Anomalies of the medial meniscus are rarer than those of the lateral meniscus, 2 but the most common types of such anomalies include medial discoid menisci, anomalous insertions of the anterior horn, meniscus hypoplasia, a ring-shaped meniscus, and meniscal ossicles.3–5 Many types of meniscal malformations have been reported because of the central role they play in causing pain and limiting a patient’s daily activities. Anomalous insertions of the anterior horn of the medial meniscus into the anterior cruciate ligament (ACL) have been infrequently reported. Three cases were reported by our department in 2010 6 ; however, to the best of our knowledge, this is the first case report of an anomalous insertion of the anterior horn of the medial meniscus into the ACL combined with hypertrophy of the anterior horn and a symptomatic synovial cyst (Figure 1).
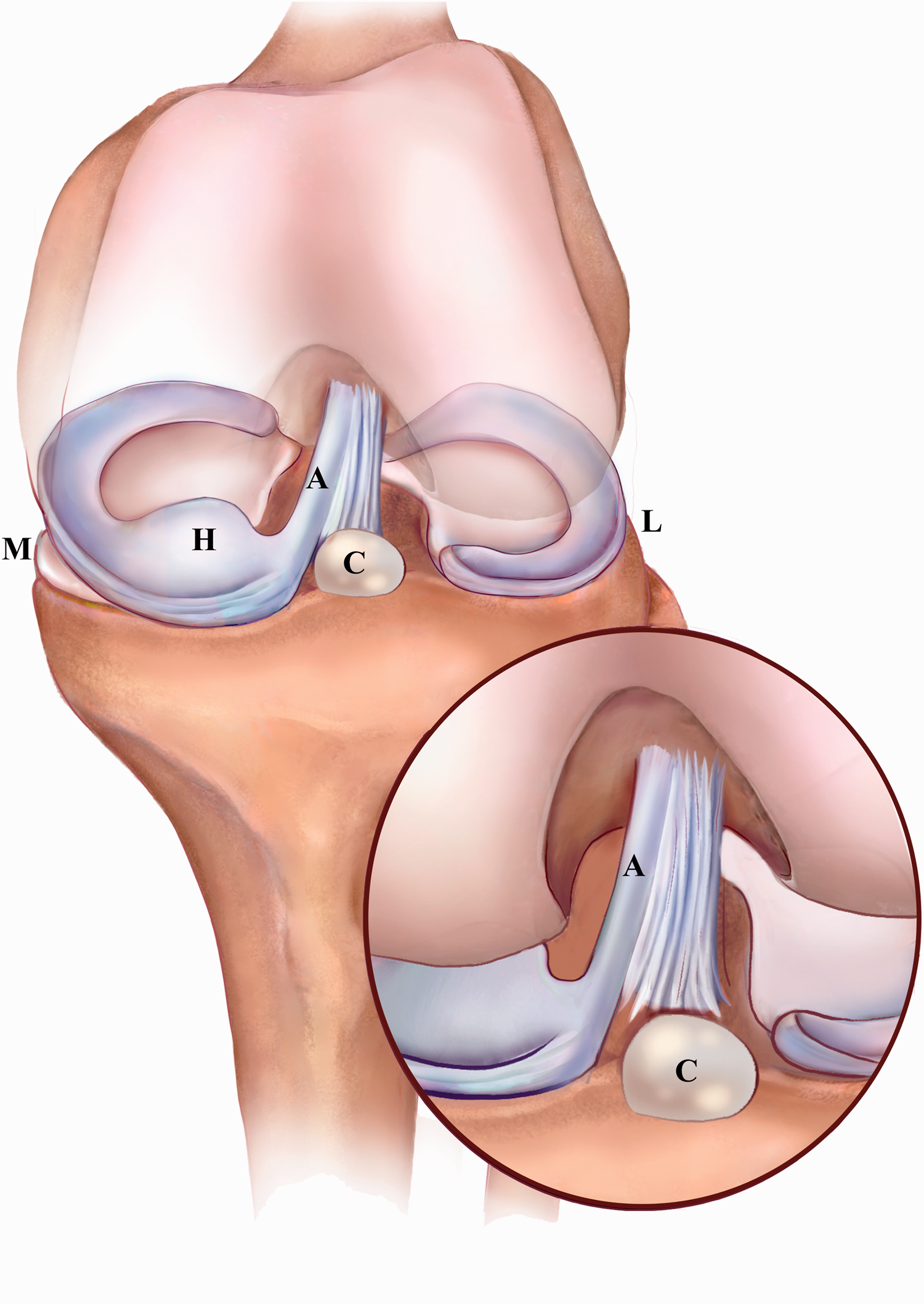
Three-dimensional modeling images of the malformation by the software Photoshop CC (Adobe Inc., San Jose, CA, USA).
To help guide clinical practice, we collected and summarized relevant articles on anomalous insertions of the anterior horn of the medial meniscus. These articles were obtained from PubMed, SciELO, ScienceDirect, MEDLINE, and Google Scholar. The following keywords were used in the search: “medial meniscal anatomic variants” and/or “medial meniscus anomaly” and/or “anomalous insertions of medial meniscus” and/or “medial meniscus abnormality.” The medial meniscus malformations identified during the literature search were then briefly summarized with a particular focus on the diagnosis and treatment of anomalous insertions of the anterior horn of the medial meniscus.
Case report
History
A 26-year-old man was admitted to our hospital with an aching pain in the left knee due to a crash injury. The pain had persisted for 1 month, and the patient had experienced no symptoms before the injury. Physical examination revealed a positive hyperextension test result, and the range of motion was 0° to 140°. He felt pain during terminal extension and could not endure overextension. There was no swelling or tenderness of the knee. The results of a McMurray test, an anterior drawer test, and a lateral stress test were negative. In the right knee, the results of these tests were also negative and the range of motion was normal.
Imaging characteristics
A radiograph of the knee was normal. T2-weighted magnetic resonance imaging (MRI) showed hypointense cord-like tissue in the anterolateral side of the ACL (Figure 2(a), (b)), a cyst in front of the tibial insertion site of the ACL (Figure 2(c)), and hypertrophy of the anterior horn of the medial meniscus (Figure 2(d)). We suspected that this deformity was symmetrical and therefore performed an MRI examination of the contralateral knee. The right knee was similar to the left, with hypointense cord-like tissue in front of the ACL, hypertrophy of the anterior horn of the medial meniscus, and a cyst in front of the tibial insertion site of the ACL (Figure 3(a), (b)); however, the cyst was smaller than that in the left knee (Figure 3(c) and Figure 4).

Preoperative magnetic resonance imaging. (a) The anomalous insertion of the medial meniscus in the coronal plane (yellow arrowhead). (b) The anomalous insertion in the sagittal plane (yellow arrowhead). (c) The clearly visible cyst in the sagittal plane (white arrowhead). (d) Hypertrophy of the anterior horn of the medial meniscus (white arrowhead).

Magnetic resonance imaging of the contralateral knee. (a), (c) Hypointense cord-like tissue was present in front of the anterior cruciate ligament (yellow arrowhead), and (b) a cyst was present in front of the tibial insertion site of the anterior cruciate ligament (white arrowhead). Hypertrophy of the anterior horn of the medial meniscus was also present in the contralateral knee.

Size of the cysts in both knees. The long and short axes of the cyst in the left knee were 10.31 and 8.06 mm, respectively. The long and short axes of the cyst in the right knee were 9.60 and 6.40 mm, respectively.
Arthroscopic examination
Arthroscopic examination of the left knee revealed a cyst anterior to the ACL tibial insertion site, an anomalous insertion of the medial meniscus that ran from the anterior horn to the lateral femoral condyle (Figure 5(a)), and abnormal hypertrophy of the anterior horn of the medial meniscus (Figure 5(b)). No traumatic changes, such as bleeding, were present around the synovial cyst or the anterior horn of the medial meniscus. When the knee was extended, the cyst and the anterior horn were compressed by the femur and tibia (Video 1). We therefore completely excised the cyst with a shaver and trimmed the anterior horn of the medial meniscus (Figure 5(c)). However, we did not treat the anomalous insertion; instead, we only obtained a tissue sample for pathological examination. Hematoxylin–eosin staining revealed that the anomalous insertion comprised fibrocartilage and collagen fibers (Figure 6(a)), the region of hypertrophy comprised fibrocartilage (Figure 6(b)), and the cyst was a synovial cyst (Figure 6(c).

Intraoperative images. (a) During the operation, the cyst and anomalous insertion were confirmed. (b), (c) During the operation, the hypertrophy of the anterior horn of the medial meniscus was confirmed, and we used basket forceps and a shaver to trim the anterior horn of the medial meniscus.

Postoperative pathologic examination (hematoxylin–eosin staining) revealed that (a) the anomalous insertion comprised fibrocartilage and collagen fibers (25×), (b) the hypertrophy comprised fibrocartilage (400×), and (c) the cyst was a synovial cyst (25×).
Postoperative rehabilitation
After surgery, the patient used a disposable knee supporter for 3 days and was encouraged to perform range-of-motion exercises and quadriceps exercises. Full range of motion was achieved within 2 weeks of the arthroscopic surgery.
Follow-up
MRI re-examination 6 months after surgery revealed that the anterior horn of the medial meniscus was smaller than before surgery (Figure 7(a)) and matched the femoral condyle. Additionally, most of the anomalous insertion was preserved and the cyst had been completely excised (Figure 7(b)). Eighteen months after the operation, the patient had no pain and the hyperextension test was negative. No significant muscle atrophy was present, and the patient experienced no lifestyle restrictions, including when practicing sports.

Postoperative magnetic resonance imaging. (a) Six months after the operation, magnetic resonance imaging re-examination revealed that the anterior horn of the medial meniscus was smaller than that preoperatively. (b) The synovial cyst had been completely removed, and no evidence of recurrence was present.
Discussion
In our department, anomalous insertions of the anterior horn of the medial meniscus into the ACL have been seen in four cases during the past 10 years. Three of these four cases were associated with a medial meniscus tear, 6 and only one was associated with hypertrophy of the anterior horn of the medial meniscus and a synovial cyst anterior to the ACL tibial insertion site (the case reported herein).
We considered the anterior cyst to be the primary cause of the patient’s symptoms in the present case for three main reasons. First, when operating on this patient, we observed an impact on the cyst during knee straightening, which was consistent with the patient’s symptoms. We only removed the cyst and trimmed the anterior horn of the meniscus without addressing the anomalous insertion, and the patient’s pain disappeared postoperatively. Second, MRI examination of the contralateral (right) knee also revealed an anomalous insertion, hypertrophy of the anterior horn of the medial meniscus, and an anterior cyst. However, the cyst was smaller than that on the operational side, potentially explaining why the right knee was asymptomatic. Third, the patient received conservative treatment for approximately 1 month before the operation, mainly consisting of nonsteroidal anti-inflammatory drugs and shock wave and other physical therapies. If the patient’s symptoms had been caused by the subpatellar fat pad or synovitis, he should have experienced significant relief with this conservative treatment. However, his symptoms were not significantly alleviated.
There are many types of medial meniscus anomalies. Smillie 7 reported that the incidence of a medial discoid meniscus was 0.3%, and Kim and Choi 8 reported a case of an extremely rare bilateral complete discoid medial meniscus. Benedick et al. 5 reported a case involving an 18-year-old man with a diminutive-appearing medial meniscus that was identified by MRI and confirmed by diagnostic arthroscopy. Ohkoshi et al. 9 conducted arthroscopic studies of variants of the anterior horn of the medial meniscus, and the most common variant was a meniscus attached to the ACL or transverse ligament. 10 Our literature search produced 16 articles involving 56 cases of anomalous insertions of the medial meniscus into the ACL (Table 1). Johnson 11 first reported an anomalous insertion of the anterior horn of the medial meniscus into the ACL, although he did not provide details. Rainio et al. 12 reported that the incidence of an anomalous insertion of the anterior horn of the medial meniscus was 1.2%. However, no previous reports have described an anomalous insertion of the anterior horn of the medial meniscus combined with hypertrophy of the anterior horn and a synovial cyst.
Literature review of anomalous insertions of the anterior horn of the medial meniscus.

The mechanism by which an anomalous insertion of the anterior horn of the medial meniscus is formed remains unclear, although it is generally believed to be closely related to an abnormal variation during embryonic development. During embryological development, the meniscus and cruciate ligaments appear at approximately 7 weeks. Both structures are formed directly from the blastema and not from secondary invasion of the synovial tissue into the joint. 13 The anterior horn of the medial meniscus attaches to the anterior aspect of the upper tibia near the joint line during the 10th and 11th weeks of embryological development. This may be a critical time for the development of the anomaly. 12 If the synovial fold that separates the articular cavity of the fetus is not fully recessed, it will develop in to the subpatellar fat pad. Therefore, an anomalous insertion of the anterior horn of the medial meniscus into the ACL and hypertrophy of the anterior horn may be two variants of the subpatellar fat pad.
Nakajima et al. 14 reported that the pathology of the anomalous insertion is fibrocartilaginous tissue, as in other parts of the meniscus. Arjun et al. 15 reported that the anomalous insertion consisted of fibrous cartilage tissue, and Nagashima et al. 16 found that the anomalous insertion consisted of loose fibrous connective tissues. However, one pathological finding among our four patients was that the anomalous insertion consisted of collagen fibers, and the anomalous insertion in the present case comprised both fibrocartilage and collagen fibers. Therefore, we cannot rule out the possibility that the anomalous insertion is a positional variation of the ACL. In addition, these pathological differences in the anomalous insertions may be related to the sampling location, with proximity to the anterior horn of the medial meniscus versus proximity to the ACL leading to different pathological results as follows: a sampling location closer to the meniscus is closer to the fibrocartilage, and a sampling location closer to the ACL is closer to the ligament.
Whether meniscus injuries are related to anomalous meniscus insertions is unclear. The meniscus moves back and forth as the knee flexes and extends. Because of the larger distance between the anterior and posterior horns of the medial meniscus, and because the body of the medial meniscus is closely connected with the tibial collateral ligament, the movement range of the medial meniscus is significantly smaller than that of the lateral meniscus. 17 An anomalous insertion of the anterior horn of the medial meniscus may further limit the movement of the anterior horn of the medial meniscus such that when an external force suddenly acts on the knee, the medial meniscus cannot cooperate with the movement of the femoral condyle in a timely manner, resulting in meniscus injury. 18 Therefore, we believe that an anomalous insertion of the anterior horn of the medial meniscus into the ACL may make the medial meniscus more vulnerable to injury. In addition, the genu varus deformity observed in one of our four patients (not in the patient described herein) may have also aggravated the stress on the medial meniscus, leading to meniscus injury.
In most of the cases identified in our literature search, the patients had no related clinical symptoms and the anomalous insertions were unexpectedly found during arthroscopy. 15 When we subsequently reviewed the cases from our department using MRI, we consistently found a hypointense linear structure arising at the anterior horn of the medial meniscus and coursing superiorly along the ACL,3,15,19 and the MRI signal was the same as that of the meniscus and the ACL. Additionally, in most of these patients, the medial meniscus was significantly larger than normal. Despite this larger size and that the anomalous insertion had no bony attachment, no significant meniscal extrusion was present. This might be explained by the the anomalous insertion acting as an anchor for the anterior horn of the medial meniscus. MRI always reveals a high-signal gap between the ACL and the anomalous insertion, which is often misdiagnosed as a tear of the anterior horn of the medial meniscus. 20 Attention should therefore be paid to differential diagnosis.
No consensus has been reached on the treatment of an anomalous insertion of the anterior horn of the medial meniscus into the ACL, and it is important to establish whether the patient’s symptoms are being caused by the anomalous insertion. 21 Santi and Richardson 22 described a patient whose symptoms were fully relieved by resection of the anomalous insertion. Shea et al. 13 reported a case of anomalous insertion of the medial meniscus with subluxation of the patella. The pain at the medial joint line disappeared after excision of the anomalous insertion, indicating that removal of anomalous insertions may not have a detrimental effect. The same operation and outcome were also reported by Nakajima et al. 14 However, Rainio et al. 12 described 11 patients with anomalous insertions, among whom only 1 considered that resection of the anomalous insertion relieved the pain. Kim et al. 23 reported four cases of a lateral discoid meniscus with anomalous insertion of the anterior horn of the medial meniscus, and they concluded that simply trimming the lateral discoid meniscus could relieve the patients’ symptoms. Arjun et al. 15 successfully treated a patient with a medial meniscal tear associated with an anomalous insertion by only partial medial meniscectomy, with no treatment for the anomalous insertion. The symptoms in all four of our patients disappeared completely despite our only repairing the torn meniscus or trimming the hypertrophy of the anterior horn of the medial meniscus and completely excising the cyst without performing any treatment for the anomalous insertion.
We conclude that a patient’s symptoms may not necessarily be related to an anomalous insertion and that if there are other injuries potentially causing the symptoms, the anomalous insertion requires no special treatment.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
The patient and his family were informed that data from his case would be submitted for publication, and they provided their consent. This study was approved by the Ethics Committee of Peking University Shenzhen Hospital.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sanming Project of Medicine in Shenzhen [grant number SZSM201612078].
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.