
Abstract
Study Design
Questionnaire.
Objective
To evaluate the ability of spine surgeons to distinguish C8–T1 radiculopathies from ulnar neuropathy.
Methods
Twenty-four self-rated “experienced” cervical spine surgeons completed a questionnaire with the following items. (1) If the ulnar nerve is cut at the elbow, which of the following would be numb: ulnar forearm, small and ring fingers; only the ulnar forearm; only the small and ring fingers; or none of the above? (2) Which of the following muscles are weak with C8–T1 radiculopathies but intact with ulnar neuropathy at the elbow: flexor digiti minimi brevis, flexor pollicis brevis, abductor digiti minimi, abductor pollicis brevis, adductor pollicis, opponens digiti minimi, opponens pollicis, medial lumbricals, lateral lumbricals, dorsal interossei, palmar interossei?
Results
Fifteen of 24 surgeons (63%) correctly answered the first question—that severing the ulnar nerve results in numbness of the fifth and fourth fingers. None correctly identified all four nonulnar, C8–T1-innervated options in the second question without naming additional muscles.
Conclusion
The ulnar nerve provides sensation to the fourth and fifth fingers and medial border of the hand. The medial antebrachial cutaneous nerve provides sensation to the medial forearm. The ulnar nerve innervates all intrinsic hand muscles, except the abductor and flexor pollicis brevis, opponens pollicis, and lateral two lumbricals, which are innervated by C8 and T1 via the median nerve. By examining these five muscles, one can clinically differentiate cubital tunnel syndrome from C8–T1 radiculopathies. Although all participants considered themselves to be experienced cervical spine surgeons, this study reveals inadequate knowledge regarding the clinical manifestations of C8–T1 radiculopathies and cubital tunnel syndrome.
Introduction
In a population-based investigation in the United States, Radhakrishnan et al demonstrated an annual incidence of 83 per 100,000 for any cervical radiculopathy; a total of 561 individuals with cervical radiculopathy were studied. 1 C8 was implicated in 35 cases (6.2%), making it the least frequently involved root. 1 As such, isolated C8–T1 radiculopathies are relatively uncommon conditions. 1 , 2 In contrast, among the more common upper extremity entrapment syndromes, ulnar neuropathy originating from the elbow (cubital tunnel syndrome) is second in prevalence to only carpal tunnel syndrome. 3 , 4 Moreover, the incidence of such upper extremity compression syndromes has been rising over recent decades. 3
Electromyography (EMG) and nerve conduction studies (NCS) can assist in confirming either peripheral neuropathy or cervical radiculopathy following physical examination. 2 , 3 , 5 , 6 Their high false-negative rate and suboptimal specificity, however, may limit diagnostic value. 2 , 5 , 6 , 7 , 8 Indeed, Ashkan et al found a sensitivity of 42% and specificity of 40% in diagnosing cervical radiculopathy with EMG and NCS. 7 Considering this and the disparity in incidence between C8–T1 radiculopathies and cubital tunnel syndrome, the physical examination is exceptionally important.
In our experience, gained through years of personal interaction with a large number of spine surgeons at national conferences and cadaver courses, for example, many physicians, including spine surgeons, are satisfied with testing grip strength alone and often fail to demonstrate adequate knowledge regarding the intrinsic hand muscles innervated by C8 and T1. To assess how well practicing spine surgeons are able to differentiate C8–T1 radiculopathies and cubital tunnel syndrome, we designed a brief questionnaire on the most clinically relevant anatomy.
Materials and Methods
Questionnaire Design and Administration
The senior author developed the study questionnaire to be a simple yet comprehensive instrument for the assessment of knowledge regarding the differential manifestations of C8–T1 radiculopathies and cubital tunnel syndrome. The correct answers were confirmed through literature review. The questionnaire was administered as a component of a hands-on Continuing Medical Education course: Expert Techniques for Complex Cervical Surgery: Deformity, Tumors, Transoral Exposures, and Vertebral Artery Dissection (Burr Ridge, Illinois, May 14 to 15, 2010). The course was designed for and marketed to orthopedic and neurologic surgeons who considered themselves experts in routine cervical spine procedures and were interested in learning complex techniques. As the title suggests, covered techniques included various forms of osteotomy for deformity correction, circumferential and mandible-splitting procedures for cervical tumors, transoral exposure of the upper cervical spine, and management of vertebral artery injury.
Thirty-four surgeons completed the course. Each participant was given the opportunity to complete the questionnaire, which was described as an investigational tool to assess their cervical and upper extremity neuroanatomy knowledge base. The participants did not discuss answers with one another before submitting their forms, nor did they access alternative sources of information (i.e., a textbook or the Internet).
Questions
If the ulnar nerve is cut at the elbow, which of the following would be numb? Circle the single best answer.
Ulnar forearm, small and ring fingers
Only the ulnar forearm
Only the small and ring fingers
None of the above
To differentiate between pure ulnar neuropathy and C8–T1 radiculopathies, it is helpful to know which muscles are innervated by C8 and T1. Which of the following muscles are likely to be weak in a patient with C8–T1 radiculopathies but intact in a patient with ulnar neuropathy at the elbow? Circle all that apply.
Flexor digiti minimi brevis
Flexor pollicis brevis
Abductor digiti minimi
Abductor pollicis brevis
Adductor pollicis
Opponens digiti minimi
Opponens pollicis
Medial lumbricals
Lateral lumbricals
Dorsal interossei
Palmar interossei
Results
Thirty-four surgeons participated in the cadaver course. There were 33 men (97%) and 1 woman (3%). Twenty-five were orthopedic surgeons (74%), and 9 were neurosurgeons (26%). Of the 23 participants (68%) who practiced within the United States, represented states included Wisconsin, New York (two), Pennsylvania, South Carolina, Maryland, Connecticut, Mississippi, Minnesota, Georgia, California (two), Rhode Island (two), Utah, Texas (two), Arizona, Illinois (two), Tennessee, North Carolina, and Kentucky. Eleven surgeons (32%) practiced in Brazil (four), Canada, Spain, South Korea (three), Japan, and India.
Twenty-four of 34 surgeons (71%) completed the questionnaire. Fifteen of 24 (63%) correctly answered option C on the first question—that severing the ulnar nerve would result in numbness of the fifth (small) and fourth (ring) fingers alone. None of the 24 surgeons (0%) correctly identified all four nonulnar, C8–T1-innervated options without naming additional, incorrect muscles. The four correct options, encompassing a total of five muscles, included: the flexor pollicis brevis (B) and abductor (D) pollicis brevis, opponens pollicis (G), and lateral lumbricals (I). Although one participant circled all four correct options, six others that are ulnar-innervated were also identified. One surgeon chose two correct options only, and another selected two correct and one incorrect options.
Discussion
Considering the relative rarity of C8–T1 radiculopathies in comparison with cubital tunnel syndrome, 1 , 2 , 3 we suspected that a parallel disparity in experience with these conditions exists among spine surgeons. Overlapping clinical manifestations further complicate diagnosis. 2 , 3 , 6 Regarding motor dysfunction, many educational resources (textbooks, review articles, Web sites, etc.) or tables and figures found therein describe little more than the “classic” patterns of grip/finger flexor and finger abductor weakness for C8 and T1 lesions, respectively. 5 , 6 , 9 , 10 , 11 , 12 This simplistic approach is insufficient for the differentiation of C8–T1 radiculopathies and cubital tunnel syndrome. The intricacies of ulnar nerve anatomy are critical in arriving at the correct diagnosis and for proper use of diagnostic studies such as EMG, NCS, and magnetic resonance imaging. We undertook this study to assess the ability of spine surgeons to differentiate C8–T1 radiculopathies from cubital tunnel syndrome.
Our results suggest that even those who might consider themselves experts in cervical spine surgery may have inadequate knowledge of C8 and T1 myotomes and dermatomes. Fewer than two-thirds (63%) of 24 orthopedic and neurologic spine surgeons were able to characterize the sensory distribution of the ulnar nerve. None could correctly identify the intrinsic hand muscles that are innervated by the C8–T1 nerve roots but not the ulnar nerve.
The ulnar nerve provides sensation to the medial half of the fourth finger, entire fifth finger, and ulnar border of the hand (Fig. 1).13 This sensory distribution applies to both the palmar and dorsal sides of the hand and fingers.13 In contrast, the median nerve serves the medial palm as well as the entire palmar and distal dorsal surfaces of the lateral 3.5 digits.13 The ulnar nerve does not provide sensation to the medial forearm, which is innervated by the medial antebrachial cutaneous nerve.13 C8 and T1 supply the medial antebrachial cutaneous nerve via the medial cord of the brachial plexus, arising between the neck and proximal upper extremity (Fig. 2).13 Therefore, an ulnar lesion at the elbow—a common site of compression or trauma—would result in anesthesia of the ulnar hand and fingers but not the forearm.3,13 Furthermore, loss of sensation isolated to the ventral palm and fifth finger is suspicious for ulnar nerve compression in the Guyon canal.13 Dorsal sensation is provided by the dorsal sensory branch of the ulnar nerve, which branches approximately 5 to 6 cm proximal to the ulnar styloid.13
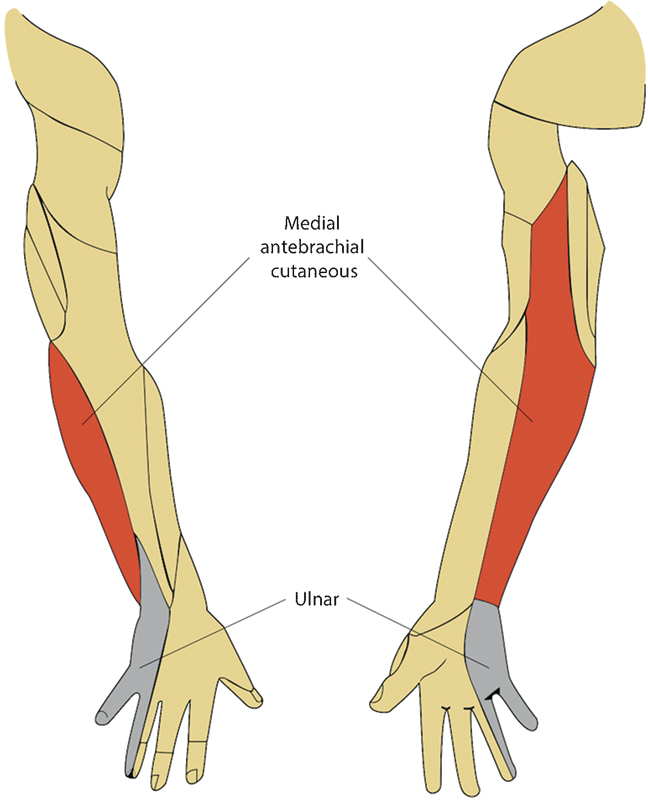
Diagram of the sensory distributions of the medial antebrachial cutaneous and ulnar nerves at the posterior (left) and anterior (right) upper extremity.
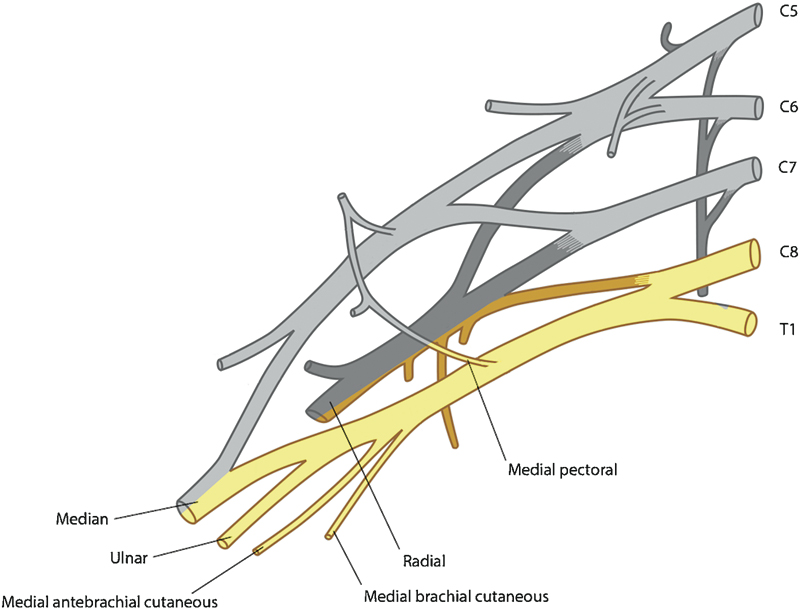
Illustration of the brachial plexus, with C8 and T1 root contributions highlighted and labeled.
Regarding the motor functions served by the C8–T1 roots and ulnar nerve, all but five intrinsic hand muscles are innervated by the latter.13 The abductor and flexor pollicis brevis, opponens pollicis, and lateral two lumbricals are innervated by C8–T1 via the median nerve, entering the hand through the carpal tunnel.13 The mnemonic AbOF the Law may be useful—the abductor (Ab) and flexor (F) pollicis brevis, opponens pollicis (O), and lateral lumbricals (Law) are “above the law” that intrinsic hand muscles are ulnar-innervated. By specifically examining these five muscles (Fig. 3), one can differentiate between cubital tunnel syndrome, which leaves their motor strength intact, and C8–T1 radiculopathies, which would result in weakness. For example, the abductor pollicis brevis elevates the thumb about the metacarpophalangeal joint to 90 degrees relative to the plane of the palm (Fig. 3B). Its strength is tested by the examiner attempting to adduct the thumb into the same plane as, or parallel to, the palm. The lumbricals engender flexion at the metacarpophalangeal joints and extension at the interphalangeal joints (Fig. 3C). The flexor pollicis brevis bends the thumb at the metacarpophalangeal joint in approximately the same plane as the palm (Fig. 3D), and the opponens allows the thumb to contact the fifth finger (Fig. 3E). Last, despite these canonical motor innervation patterns, the possibility of anomalous median-ulnar neural pathways such as a Riche-Cannieu or Martin-Gruber anastomosis should be kept in mind. 14 , 15
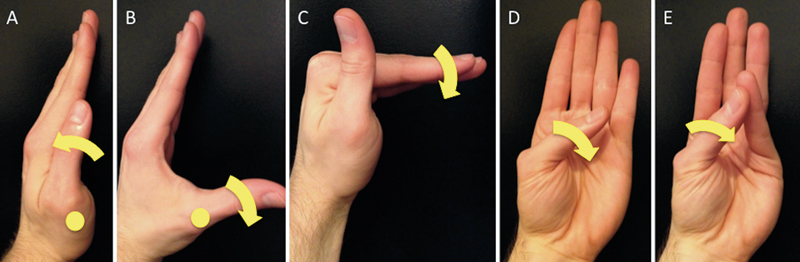
Motor actions of the adductor pollicis (A), abductor pollicis brevis (B), lumbricals (C), flexor pollicis brevis (D), and opponens pollicis (E). Metacarpophalangeal joints are indicated by yellow circles in A and B.
Although all of the surveyed physicians were currently practicing spine surgeons, this study reveals a surprisingly poor degree of knowledge concerning differentiation between C8–T1 radiculopathies and cubital tunnel syndrome. In large part, these results may be attributable to the spine component, or relative lack thereof, employed in modern medical school and resident training curricula. Anecdotally, the finer yet diagnostically crucial details of hand function, as it relates to spinal disorders, are too often neglected. Indeed, even basic musculoskeletal medical education seems to be lacking in the United States, despite the massive socioeconomic burden these conditions place on the country. 16 , 17 , 18 Recently, Scher et al demonstrated a substantial paucity of knowledge concerning common upper extremity/hand surgery conditions among internal and emergency medicine residents. 16 Fortunately, it appears that augmenting time devoted to upper extremity education in medical school (from approximately 7 to 21 hours) improves confidence in relevant physical examination performance. 19 We recommend analogous additions to spine curricula. Moreover, textbook authors should also strive to provide adequate physical examination instruction. The risks inherent in teaching overly simplistic examination techniques may ultimately fail to outweigh their benefits by instilling a false sense of security in the examiner.
It is our understanding that this is the first study to directly evaluate fundamental aspects of anatomical knowledge among a cohort of spine surgeons. In our estimation, the utilized questions were both comprehensive and straightforward. Accordingly, these results may provide insight into specific deficiencies in current medical education. Still, this investigation is not without limitations. A small number of surgeons were queried. Therefore, caution should be exercised before generalizing these findings to the spine surgeon community at large. Furthermore, the participants were attending a cervical spine course, so the study may lack external validity when attempting to generalize its results to those surgeons who focus on thoracolumbar pathology. The small number and lack of demographic data pertaining specifically to those who answered the survey precluded any in-depth statistical analysis of performance. Participants also held little incentive to answer to the best of their abilities, and there were no means to gauge each surgeon's confidence in his or her answers. In practice, should a surgeon feel uncomfortable with a diagnosis or the significance of a neurologic deficit, a reliable text, Internet resource, and/or colleague could be easily consulted before proceeding. Such alternatives were not utilized during the administration of our questionnaire.
In conclusion, even currently practicing orthopedic and neurologic cervical spine surgeons may lack complete knowledge of ulnar and C8–T1 neuroanatomy. To consistently avoid misdiagnosis, every spine surgeon should be intimately aware of the motor and sensory sequelae of C8–T1 radiculopathies. Of course, we would not expect our colleagues to pursue surgery without the corroboration of advanced imaging, but computed tomography and magnetic resonance imaging are expensive and not without risk to the patient. Further, EMG and NCS may facilitate proper diagnosis of C8–T1 radiculopathies and cubital tunnel syndrome, 2 , 3 , 5 , 6 but these and similar modalities should not serve as an excuse for subpar familiarity with fundamental anatomy.
Disclosures
None