
Abstract
The ideal treatment for unstable thoracolumbar fractures remains controversial with posterior reduction and stabilization, anterior reduction and stabilization, combined posterior and anterior reduction and stabilization, and even nonoperative management advocated. Short segment posterior osteosynthesis of these fractures has less comorbidities compared with the other operative approaches but settles into kyphosis over time. Biomechanical comparison of the divergent bridge construct versus the parallel tension band construct was performed for anteriorly destabilized T11–L1 spine segments using three different models: (1) finite element analysis (FEA), (2) a synthetic model, and (3) a human cadaveric model. Outcomes measured were construct stiffness and ultimate failure load. Our objective was to determine if the divergent pedicle screw bridge construct would provide more resistance to kyphotic deforming forces. All three modalities showed greater stiffness with the divergent bridge construct. The FEA calculated a stiffness of 21.6 N/m for the tension band construct versus 34.1 N/m for the divergent bridge construct. The synthetic model resulted in a mean stiffness of 17.3 N/m for parallel tension band versus 20.6 N/m for the divergent bridge (p = 0.03), whereas the cadaveric model had an average stiffness of 15.2 N/m in the parallel tension band compared with 18.4 N/m for the divergent bridge (p = 0.02). Ultimate failure load with the cadaveric model was found to be 622 N for the divergent bridge construct versus 419 N (p = 0.15) for the parallel tension band construct. This study confirms our clinical experience that the short posterior divergent bridge construct provides greater stiffness for the management of unstable thoracolumbar fractures.
Keywords
The central problem in osteosynthesis of unstable thoracolumbar fractures has been the inability to maintain a normal sagittal alignment postoperatively once the fracture has been reduced, causing kyphosis that can lead to back pain. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 There remains no consensus on the approach to be used to stabilize these fractures and to prevent subsequent sagittal deformity. 9 , 10 , 11 , 12 Posterior reduction and stabilization, anterior reduction and stabilization, and combined posterior and anterior reduction and stabilization have all been advocated for in the literature. 8 , 13 Successful nonoperative management of these fractures in neurologically intact patients is also supported in the literature with ample evidence of spinal canal remodeling regardless of the type of treatment chosen. 8 , 14 , 15 , 16 Among the surgical approaches, isolated posterior reduction and stabilization has the advantage of limiting blood loss, surgical time, and perioperative complications compared with anterior reduction and stabilization. 8 However, short posterior spinal instrumentation has been partly discredited on the basis of inadequate stability and need for subsequent anterior column reconstruction with cages to prevent collapse into kyphosis. 5 , 17 , 18 , 19
Contrary to reports in the literature, our clinical experience with short posterior spinal fixation for unstable thoracolumbar burst fractures has been very successful. We, therefore, continue to manage our unstable thoracolumbar fractures with short posterior spinal fixation without seeing clinically significant kyphosis. We hypothesize that our results differs from those reported in the literature due to the additional stability provided by the divergent bridge construct that we utilize. Rather than inserting the screws down the axis of the pedicles, which results in the classic parallel tension band construct, we insert the pedicle screws in an eccentric and divergently angulated fashion using intraoperative fluoroscopic guidance (Fig. 1). This results in a more secure bone–screw interface as the pedicle screws are resting in the subchondral bone just beside the end plates (Fig. 1). Additionally, owing to the oblique trajectory of the screws, better fixation is obtained in the pedicles. The resultant construct behaves as a bridge construct by offloading the anterior column, allowing it to heal before kyphosis develops. Biomechanical studies have confirmed that screw placement and direction does influence fixation strength. 20 However, none to date have evaluated the stiffness of the divergent screw bridge construct.
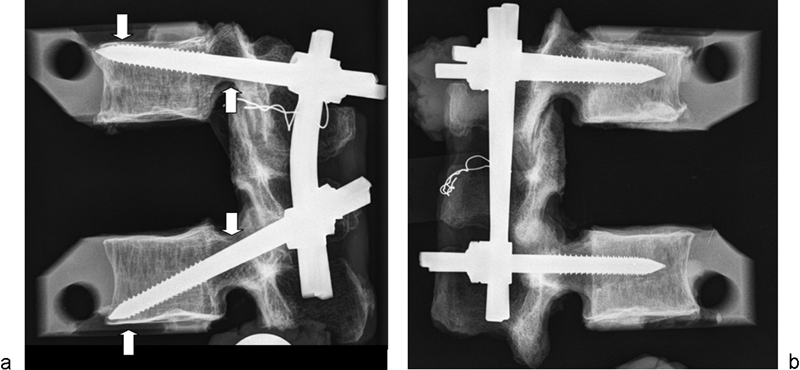
Specimen demonstrating (a) the divergent bridge construct with divergent pedicle screw placement. The vertebra is locked in with tip of pedicle screw in subchondral juxtacortical bone of the end plate and with abutment of the pedicle screw on the edge of pedicle as shown by the arrows. (b) Parallel tension band construct.
The objective of this study was to perform a biomechanical comparison of short posterior instrumentation from T11 to L1 of the divergent bridge construct versus the standard parallel tension band construct using three different anteriorly destabilized thoracolumbar spine models; (1) a finite element analysis (FEA) model, (2) a synthetic model made of ultra-high-molecular-weight polyethylene (UHMWPE), and (3) a cadaveric model. The outcomes analyzed were stiffness (Newton per meter) of the construct for all three models and the ultimate failure load (Newton) for the cadaveric model in response to compressive (kyphotic) anterior forces only as kyphosis is the main deformity that develops in these fractures postoperatively. We hypothesize that the divergent bridge construct will have a higher stiffness and a higher ultimate failure load than the parallel tension band construct.
Materials and Methods
Morphogenic Radiographic Analysis of Normal Patients
A preliminary morphogenic radiographic analysis was performed to establish the average sagittal angulation of the inferior and superior pedicle screws for the management of an unstable T12 fracture. The optimal and safe screw trajectory was determined by analyzing normal standing lumbar spine plain radiographs (X-rays) from 20 men and 20 women (Table 1) who were selected from a random sequential series of patients presenting to the emergency room. Normal X-rays showing no obvious spinal pathology in adult patients (age ≥ 18 years) included in the study. The optimal superior pedicle screw sagittal angulation was measured by drawing a line parallel to the upper end plate of T11 and drawing a line from the anterosuperior corner of T11 to a point 5 mm above the inferior cortex of the pedicle of T11 (Fig. 2). By doing so the tip of the pedicle screw would be located in the dense subchondral bone and the shaft of the pedicle screw would rest over the inferior cortex of the pedicle. Similarly, the angle for the inferiorly oriented screw at L1 was measured between a line parallel to the inferior end plate of L1 and a line connecting the anteroinferior corner of L1 to a point 5 mm below the superior cortex of the pedicle of L1 (Fig. 2). The 5-mm offset was used to provide ample space for a pedicle screw of 6-mm diameter. The average angles calculated from this analysis of pedicle screw orientations were then used to orient the pedicle screws in our models for the biomechanical analysis.
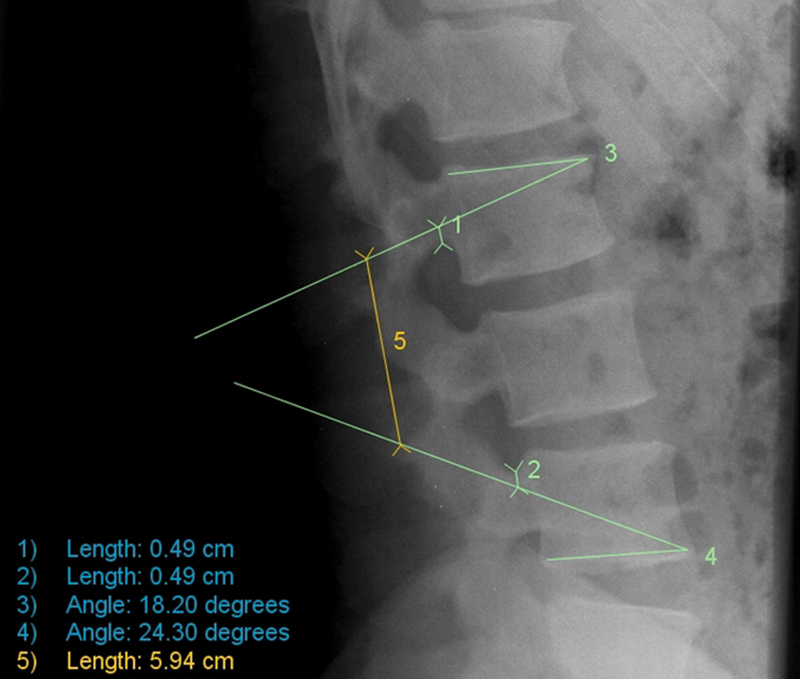
Sample morphogenic radiologic assessment of the ideal angulated pedicle screw position for the divergent bridge construct. Line (1) measures a 5-mm distance from the inferior edge of T11 pedicle; line (2) indicates a 5-mm distance from the superior edge of L1 pedicle; angle (3) is the insertion angle for the superior pedicle screw; angle (4) is the insertion angle for the inferior pedicle screw; line (5) measures the length of the rod for the divergent bridge construct.
Morphological analysis of radiographic parameters in normal subjects
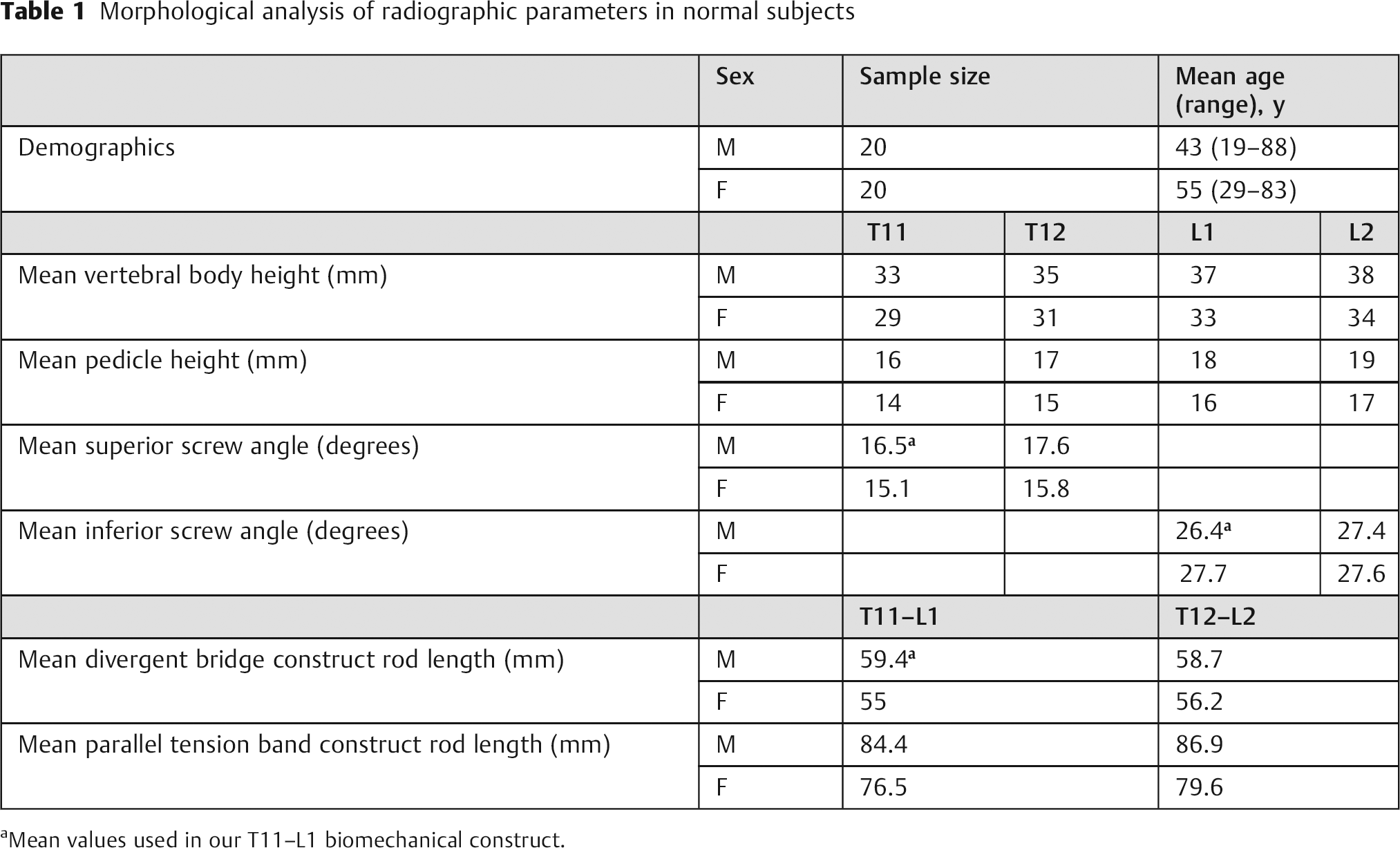
Mean values used in our T11–L1 biomechanical construct.
Biomechanical Models
The biomechanical analysis comprised of three distinct anteriorly destabilized (corpectomy) models: (1) a finite element analysis (FEA) model, (2) mechanical testing of a synthetic UHMWPE model, and (3) mechanical testing of a cadaveric model. The FEA and UHMWPE spine models were constructed based on the American Society for Testing and Material (ASTM) standard for corpectomy models (ASTM standard 1717; Fig. 3, Fig. 4). The corpectomy model standard was chosen because it represents an anteriorly destabilized construct enabling us to simulate the worst case scenario for a single-level thoracolumbar vertebral burst fracture. The parallel tension band constructs (Fig. 4) were built following the ASTM standard precisely. The divergent bridge constructs (Fig. 4) differed only in the sagittal angle of the pedicle screws, which was determined by the morphogenic radiographic analysis (Table 1).
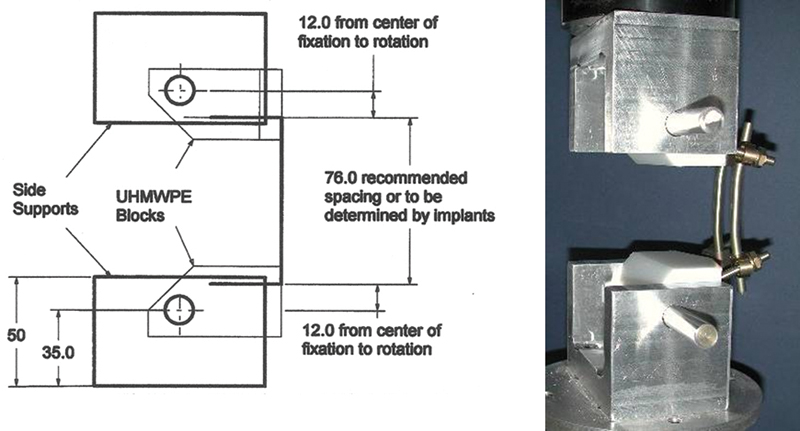
American Society for Testing and Materials (ASTM) drawings for the ultra-high-molecular-weight polyethylene (UHMWPE) corpectomy model with example of ASTM construct in testing machine fixtures.
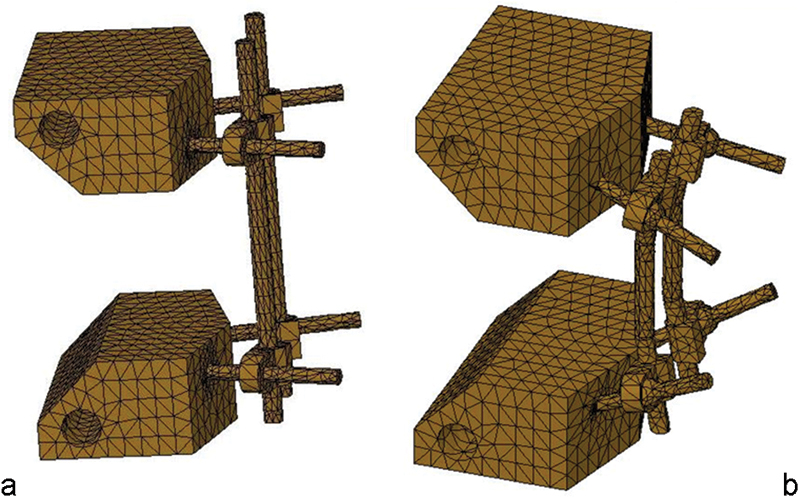
Finite element analysis models for the (a) parallel tension band construct and the (b) divergent bridge construct.
Finite Element Analysis
Linear FEA models for the parallel tension band construct and the divergent bridge construct were built using two software packages. SolidWorks (Dassault Systèmes SolidWorks Corp., Waltham, Massachusetts, United States), a parametric solid modeling software package, was used for building the three-dimensional geometric models. Subsequently, CosmosWorks (Structural Research and Analysis Corporation, Los Angeles, California, United States), an FEA software package, was used to create the mesh, apply loads and constraints, compute solutions, and display postprocessing results (Fig. 4). Linear tetrahedral elements were used to mesh the models for a total of 18,515 and 17,610 elements for the parallel and divergent models, respectively. Shanz screws, clamps, and rods were given the mechanical properties of titanium, whereas the ASTM blocks were given the mechanical properties of polyethylene. Each model was loaded with 100 N, 300 N, and 600 N sequentially, and the displacement solution was generated for each load. A load stiffness curve was generated with the three loads for each of the two models.
Synthetic Model
A total of six constructs were built according to the ASTM standard. The vertebral bodies for testing were made from UHMWPE with an ultimate tensile strength of 40 ± 3 MPa. One set of three constructs had holes drilled parallel to the plane of the end plates. This set was the control group representing the parallel tension band construct. A second set of constructs had holes drilled at 16.5 degrees cephalad in the superior vertebra (T11) and 26.5 degrees caudad in the inferior vertebra (L1) with respect to the horizontal plane of the T11 and L1 end plates, respectively, as determined by the morphogenic radiographic analysis (Table 1). This set represented the divergent bridge construct. The polyethylene blocks were instrumented using 6-mm titanium pedicle screws and 6-mm-diameter titanium hard rods (Synthes USA, Monument, Colorado, United States). The titanium screw-rod clamps (Synthes USA) allow for a maximum screw-rod angle of 16 degrees; thus, to accommodate for the maximal orientation of the divergent pedicle screws as per our morphogenic radiographic analysis, the rods for the divergent bridge constructs had to be bent 11 degrees to achieve the maximum combined angle of 43 degrees (16.5 + 26.5 degrees). The rods were bent using a calibrated rod bender to achieve a uniform contour between the bent rods. The construct to be tested was secured to the materials testing machine (858 Mini Bionix, MTS, Eden Prairie, Minnesota, United States) via side support forked fixtures with a half-inch stainless steel rod passing through each fixture (Fig. 3). Testing was done under controlled displacement at a rate of 0.4 mm/s (as per the ASTM standard) and the cross head was allowed to rotate freely about the z-axis using feedback control and a zero-torque command. The test was stopped when the load increased rapidly due to contact between the T11 and L1 UHMWPE blocks. The compressive load applied was sensed using the MTS OEM Axial Torsion Load Transducer (Model # 662.20D-03, Eden Prairie, Minnesota, United States) with a capacity of 10,000 N and an error in repeatability of 0.08% full scale. A linear variable displacement transformer (LVDT) was used to measure the axial compressive displacement. The LVDT has a linearity of 0.25% within the 100-mm full-scale range.
Cadaveric Model
Three matched pairs of six fresh frozen human thoracolumbar spines were selected based on sex, bone mineral density (BMD), and anatomical geometry (Table 2). Levels T11 through L1 for each spine were dissected, removing all muscular tissue surrounding the motion segments. One sample from each of the matched pairs was randomly instrumented with either a parallel tension band construct or a divergent bridge construct. For the parallel tension band construct, 6-mm titanium pedicle screws were inserted through the T11 pedicles (parallel to the superior end plate) and the L1 pedicles (parallel to the inferior end plate). The construct was then completed using 6-mm-diameter titanium hard rods and titanium clamps. Once rigidly fixed, a T12 corpectomy was performed. For the divergent bridge construct, the pedicle screws were inserted at the maximum anatomical angle. A custom aiming device (Fig. 5) was designed and built to reproducibly provide a 5-mm offset from either the superior or inferior aspect of the pedicle, as well as providing an accurate trajectory toward the anteroinferior or anterosuperior aspect of the end plate. For the divergent bridge construct, the rod was bent to 11 degrees as in the synthetic model. The constructs was then completed as in the parallel tension band construct with a T12 corpectomy. The T11 and L1 vertebra were then potted in polymethyl methacrylate (PMMA; DP-Pour, Denture Base Resin, DenPlus, Montreal, Quebec, Canada) using a custom potting device. To avoid artificially strengthening the end plates with PMMA, the pots were designed with windows filled with Play-doh (Hasbro, Cincinnati, Ohio), which would prevent PMMA binding to the superior end plate of the superior vertebra and the inferior end plate of the inferior vertebra. In addition, due to the variation in size and complexity of each vertebral body as well as the desire not to artificially strengthen the facets, the posterior wall of the pot was left open and was replaced with a wall of Play-doh, which could be conformed to the vertebral body. All specimens were then tested to failure using the same testing protocol described previously for the synthetic models.
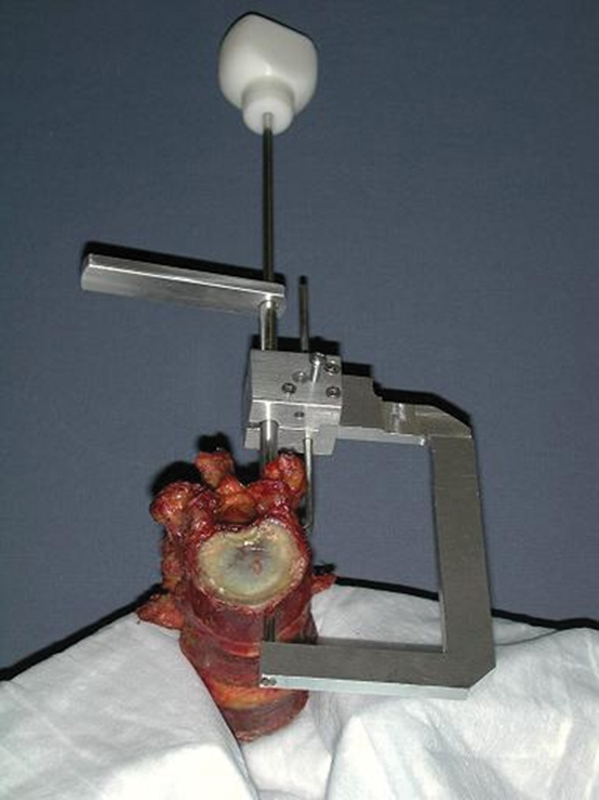
Pedicle screw aiming device made for standardized placement of pedicle screws in the cadaveric construct.
Cadaveric morphogenic and demographic data
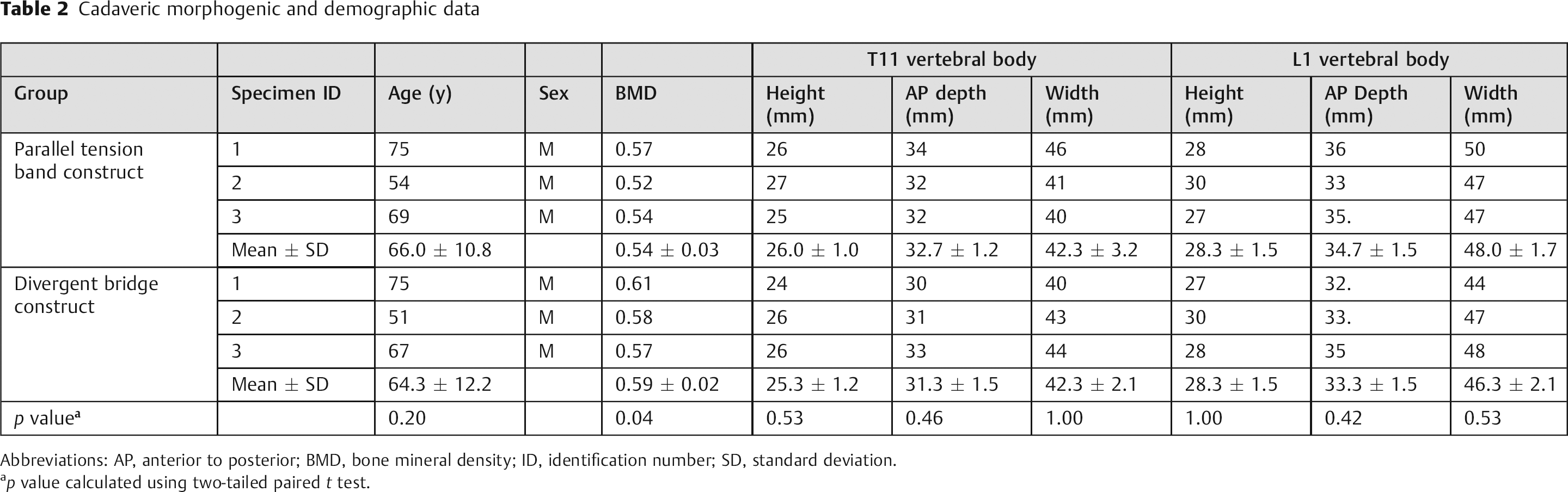
Abbreviations: AP, anterior to posterior; BMD, bone mineral density; ID, identification number; SD, standard deviation.
p value calculated using two-tailed paired t test.
Statistical Methods
Statistical analysis of the data was done with the two-tailed t test for paired data. A p value of less than 0.05 was considered significant. The results are also reported with the use of summary statistics such as mean and standard deviation (SD). A priori power analysis based on the predicted stiffness from the FEA models showed that a sample size of two items per group was needed to show a statistically significant difference (p < 0.05) with a power > 80%. We, therefore, chose a sample size of three items per group in an effort to ensure that the study would have adequate power.
Results
Morphogenic Radiographic Analysis of Normal Patients
The results of the morphological radiographic analysis (Table 1) revealed a mean cephalad angle of 16.5 degrees for the T11 vertebra in males and 15.1 degrees in females. The mean caudad angle for the L1 vertebra was found to be 26.4 degrees in males and 27.7 degrees in females. The mean rod length for the T11 to L1 parallel tension band construct was measured to be 84.4 mm for males and 76.5 mm for females, whereas the mean rod length for the T11–L1 divergent bridge construct was 59.4 degrees in males and 55 degrees in females. There were no statistically significant differences in the radiographic parameters between males and females.
Biomechanical Testing Results—FEA
The FEA model calculated a stiffness of 21.6 N/m for the parallel tension band construct versus a significantly higher stiffness of 34.1 N/m for the divergent bridge construct (Fig. 6), thereby supporting our hypothesis that the divergent bridge construct would have a higher stiffness than the parallel tension band construct for fixation of anteriorly destabilized thoracolumbar fractures.
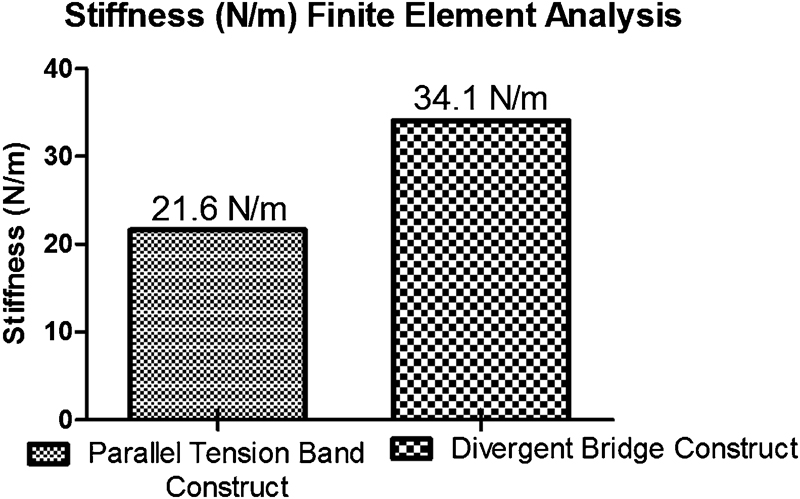
Stiffness (Newton per meter) of the two constructs tested using finite element analysis.
Biomechanical Testing Results—Synthetic Model
Testing of the synthetic UHMWPE model showed a statistically significant difference (p = 0.03) between the stiffness of the two constructs (Table 3), with the divergent bridge construct again having a higher stiffness of 20.6 (SD, 0.8) N/m compared with a stiffness of 17.3 (SD, 1.7) N/m for the parallel tension band construct. Statistical power for this analysis was calculated to be 86%.
Biomechanical testing results
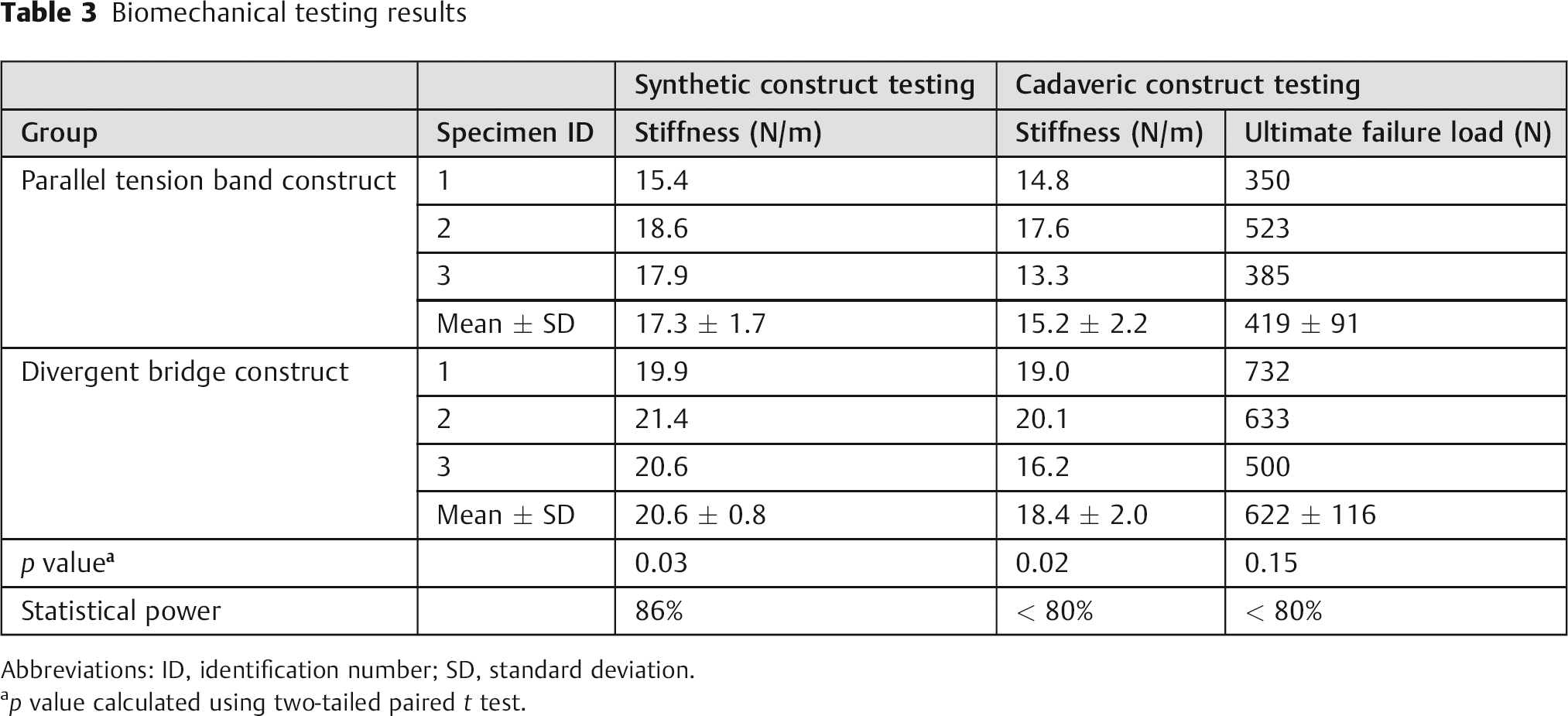
Abbreviations: ID, identification number; SD, standard deviation.
p value calculated using two-tailed paired t test.
Biomechanical Testing Results—Cadaveric Model
Similar results were seen with testing of the cadaveric models (Table 3). The mean stiffness of the divergent bridge construct was 18.4 (SD, 2.0) N/m and was greater than that of the parallel tension band construct that had a mean stiffness of 15.2 (SD, 2.2) N/m. This difference in the mean stiffness of the two constructs was statistically significant. The ultimate failure load (Fig. 7) for the divergent bridge construct was 622 (SD, 116) N and for the parallel tension band constructs it was 419 (SD, 91) N, therefore showing that the divergent bridge construct is able to withstand almost 50% more load than the parallel tension band construct. However, this difference in ultimate failure load was not statistically significant due to the small sample size that resulted in the analysis being underpowered.
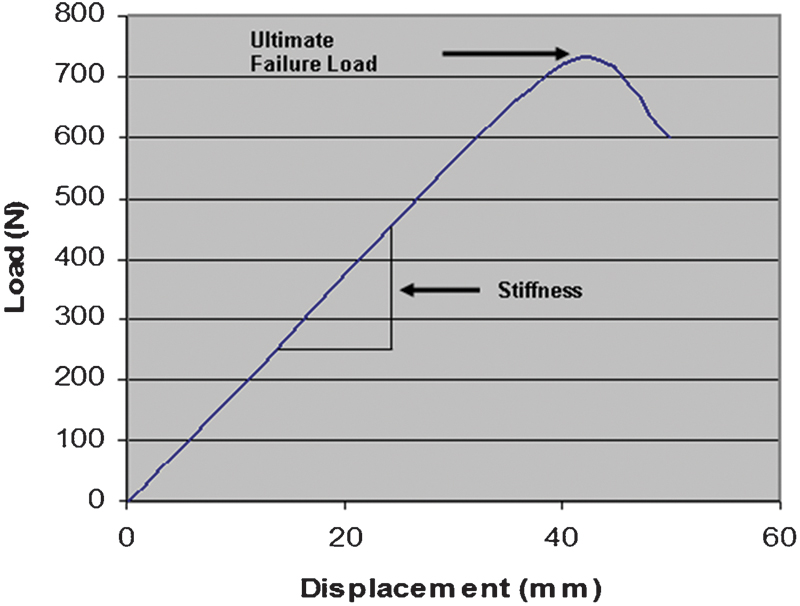
Sample graph of load (Newton) versus displacement (millimeter) showing calculation of construct stiffness (Newton per meter) and ultimate failure load (Newton).
Discussion
Biomechanical Considerations
The calculated stiffness from the FEA models was higher than that of the synthetic UHMWPE construct because the linear assumptions for the FEA models did not account for predicted plastic deformation for applied loads that are greater than the yield strength of the constructs. Similarly, the stiffness for the synthetic UHMWPE constructs was higher than that of the cadaveric constructs as the bone–screw interface was likely weaker in the cadaveric constructs. Nevertheless, the results from the three different biomechanical models support our hypothesis that the divergent bridge construct has a higher stiffness than the parallel tension band construct with the difference being statistically significant. Additionally, in the cadaveric model we noticed a trend for the divergent bridge construct to have a higher ultimate failure load than the parallel tension band construct; however, statistical significance was not reached for this comparison due to the small sample size.
These results are in keeping with previous studies looking at a similar effect of screw placement and its influence on stability. 20 , 21 , 22 From a biomechanical perspective, it is intuitive that the divergent bridge construct should provide greater stability to the spine, as it takes advantage of some basic mechanical principles:
Three-point fixation: The higher stiffness in the divergent bridge construct is seen because of added bone–screw interface strength as the tip of the screws rests in subchondral bone as opposed to purely cancellous bone in the parallel tension band construct. The angulated trajectory of the screws also gives them strong fixation points in the pedicles, resulting in an overall three-point fixation construct (Fig. 1) that results in increased stiffness.
Vectors: The angulated orientation of the pedicle screws causes the compressive force (F) on the pedicle screws to be split into two vectors (Fig. 8). This split of force vectors results in a smaller anteriorly directed compressive force (Fy) being applied across the divergent bridge construct and thus it partially offloads the anterior column. However, part of the divided force (Fx) is dissipated within the screw–clamp–rod construct that the instrumentation must resist. Therefore, the instrumentation must be designed to withstand such forces to be successful. Other biomechanical studies have shown that there is an increase in stress within the screws at the bone–screw interface, 23 again emphasizing that if short posterior fixation is to be undertaken, it must be done with adapted spinal implants designed to withstand the added loads. We suspect that the previous studies documenting high implant failure in the management of thoracolumbar fractures were utilizing standard low back spinal implants with small-diameter screws in a tension band construct that were not designed to carry the higher loads. 5 , 7 , 24 , 25 , 26
Short lever arm: The divergent orientation of the screws in the divergent bridge construct results in a shorter length for the connecting rod between the superior and inferior screws. The shorter rod length decreases the lever arm of the construct thus decreasing the overall moment of force or torque applied on the divergent bridge construct compared with the parallel tension band construct.
Opposing bend in the rod: In the divergent bridge construct, the rod has to be prebent into a lordotic alignment. This lordotic alignment of the rod might in theory increase the capacity of the rod to resist the kyphotic deforming forces incurred by a short posterior instrumentation construct for anteriorly unstable thoracolumbar fractures. However, by bending the rods, one also fatigues the metal, which can potentially lead to failure under cyclic loads. Therefore, to avoid this possible late failure, the clamps for the posterior instrumentation should be redesigned with a greater degree of freedom to maximize screw angulation without having to bend the rods.
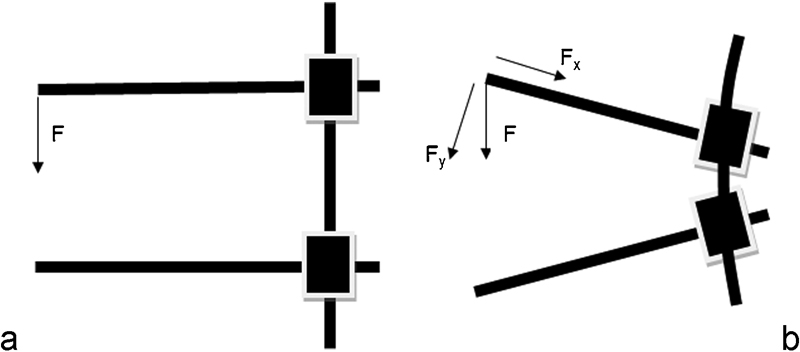
Schematic drawings showing (a) the parallel tension band construct experiencing the force vector F, whereas (b) the divergent bridge construct experiencing force vectors Fx and Fy, where F = Fx + Fy .
Anatomical Considerations
The divergent bridge construct aims to place the pedicle screws in the dense vertebral bone, thereby enhancing the bone–screw interface and thus adding greater stability to the construct. 20 This dense bone is located within the pedicles and in the juxtacortical regions of the vertebral end plates. By inserting the screw obliquely in the sagittal plane, the goal is not only to engage the lateral cortical borders of the pedicle, but also to engage the inferior and superior cortical borders of the pedicles (Fig. 1). Additionally, the tip of the pedicle screw engages the dense subchondral bone adjacent to the end plate, providing greater bone–screw interface (Fig. 1). The angulated orientation of the screw within the vertebra also impedes the vertebra from rotating into kyphosis as is seen with failure of the more conventional central pedicle screw in the tension band construct.
Clinical Application
Recent studies have shown that conservative treatment of unstable thoracolumbar fractures in neurologically intact patients do as well, if not better, than patient undergoing surgical management. 27 The indications for surgical management of these fractures are becoming more selective. 28 , 29 If a decision is made to proceed with surgical stabilization, then fundamental modern principles dictating management of thoracolumbar fractures must be followed. These include immediate rigid spinal stabilization, maintenance of neurologic integrity, minimalistic approach sparing maximal vertebral motion, and early mobilization. The current surgical practice of long posterior constructs or combined anterior and posterior spinal stabilization does not follow these modern principles. Patients with long constructs have loss of spinal flexibility and are at an increased risk of subsequent adjacent degeneration disease. 30 , 31 Additionally, anterior approaches are associated with the risk of vascular injury, significant blood loss, sympathetic dysfunction, prolonged surgical time, and visceral injury. These risks associated with long constructs or anterior surgery can be avoided by performing isolated short posterior spinal instrumentation. 32 , 33 In our clinical experience of more than 50 patients that will be reported separately, we have been able to manage the majority of thoracolumbar fractures with short posterior spinal instrumentation using a divergent bridge type spinal fixation spanning one vertebra above and one below the fractured vertebra. With this current biomechanical study using three different models, we have demonstrated that the divergent construct increases the stiffness of the posterior spinal instrumentation construct, thus partially off-loading the unstable anterior column with its added stability, thereby avoiding the need for anterior column reconstruction and associated comorbidities. It is worth mentioning that in certain cases it is possible to insert a short pedicle screw in the fractured vertebra when using the parallel tension band construct, thereby potentially increasing the construct stiffness. The placement of such a screw in the fractured vertebra is not possible in the divergent bridge construct.
A limitation of this study is that the morphological analysis to calculate screw angles was performed on T11 and L1 vertebrae for unstable T12 fractures only. Therefore, the results may not be applicable to fractures of the more proximal thoracic levels as it may not possible to achieve such divergent angles in the more kyphotic thoracic spine. A second limitation of the study is that there was a statistically significant difference (p = 0.04) in the BMD of the cadaveric vertebrae used for the divergent bridge construct (BMD = 0.59) versus those for the parallel tension band construct (BMD = 0.54). It is, therefore, possible that the higher BMD of the divergent bridge construct group also contributed to the higher stiffness and higher ultimate load to failure of the divergent bridge construct in the cadaveric model.
Conclusion
Our results show that the divergent bridge type construct provides greater stiffness than the classic parallel tension band construct. We continue to use short segment posterior spinal fixation for unstable thoracolumbar fractures that require surgical stabilization.
Disclosures
Jean A. Ouellet, Consulting: Synthes; Research Support: AO Foundation
Corey Richards, None
Zeeshan M. Sardar, None
Demetri Giannitsios, None
Nicholas Noiseux, Research Support: AO Foundation
Willem S. Strydom, None
Rudy Reindl, None
Peter Jarzem, None
Vincent Arlet, None
Thomas Steffen, Consulting: Ranier Ltd; Research Support: AOSpine, Canadian Institutes of Health Research; Stock/Options: Ranier Ltd
Footnotes
Acknowledgments
This research was assisted by a financial research grant by the AO Foundation.